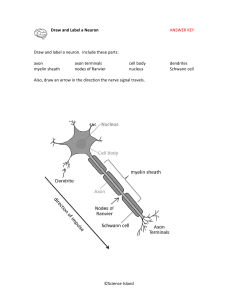
NEUROLOGICAL SYSTEM S.Y. 2223 2ND SEMESTER MEDICAL-SURGICAL NURSING PROFESSOR CEDDIE LOMIBAO 17/02/2022 MULTIPLE SCLEROSIS Autoimmune disease that affects myelin sheath of neurons in the CNS. It is also called MS = Myelin Sheath. CNS: consists of the brain and spinal cord. When myelin sheaths are being attacked by the body, it causes inflammation and scarring of the neuron decrease in nerve signal transmission which may cause motor and sensory symptoms. Role of neuron is to transmit electric signals to another neuron, gland or a muscle. QUICK FACTS Immune related immune system attacks the myelin sheath that is protecting the axons, therefore damage to the myelin sheath may cause ineffective transmission of signal of the axon. Systems vary specifically where the lesions are in the CNS. o Cerebellar: tremors, dysarthria, ataxia, cognitive o Optic Nerve: pain when moving eyes, blurry vision, dark spots Most common form of MS: relapsing-remitting MS (patients will have symptoms that will appear and disappear) Common in: o Women o 20-40 years old Cause: unknown No cure: however, lifestyle changes & medications may help to improve signs and symptoms. PATHOPHYSIOLOGY Myelin sheath has experienced damage called demyelination. Signal will be transferred ineffectively because the myelin sheath was damaged which was responsible for insulating and protecting the axon for a complete and effective transmission of signal. Normal: Dendrites Soma (body) Axon (insulated and protected by myelin sheath) Axon terminal neuron/muscle /gland to initiate a certain response/action. It is normally expected for patients with MS to have sensory and some motor symptoms. DIAGNOSTIC PROCEDURES It takes time to diagnose MS so the neurologist needs to assess various things; there is no single test that is indicative of MS. Assess signs and symptoms to rule out other diseases. MRI – to check for lesions on the neurons of the CNS Lumbar puncture – assess CSF for elevated proteins, specifically oligoclonal bands showing inflammation is present in the CNS which correlates to MS. Evoked potential studies: electrical signals are transmitted to the CNS and response shall be assessed afterwards. SIGNS AND SYMPTOMS EMOTION & COGNITIVE Drained (fatigue) Depressed Speech issues – swallowing Mood swings Trouble thinking (focus, problem solving) SENSATION Tremors Spasms Clumsy Numbness & tingling Dizzy Coordination Positive Romberg’s sign lesions on cerebellar area which is responsible in knowing where your body is in space when you close your eyes. (they lose their balance when they walk with eyes closed) LHERMITTES SIGN If patient moves their head in various motions, they may experience electric shock sensation. VISION Nystagmus Optic neuritis o Double vision o Blurry vision o Dull/gray vision o Pain moving eyes o Dark spots vision ELIMINATION Urine o Can’t hold urine: nocturia, overactive bladder o Problems w/ contraction to void: retention Bowel: constipation/diarrhea, can’t hold stool UHTHOFF’S SIGNS Heat makes signs and symptoms WORST! NURSING INTERVENTIONS SAFETY (vision, coordination, decreased perception of pain, bowel/bladder, RRMS prevention, medications) Prevent increase of signs and symptoms o Heat can make it worst, so maintain temperature (nice and cool) o Stress can worsen the symptoms – perform stress relief exercises or techniques o Avoid infection and overexertion Exercise very important: increase energy, decrease depression DO NOT OVER DO IT! o Swimming o Water aerobics Use assistive devices: showering standing is hard for them so provide shower chair, handrails to hold on to, clutter-free space and scan the environment due to vision changes Consult SLP (speech and swallowing difficulties) and PT (exercise, devices) and SUPPORT GROUPS. Bladder: o If overactive bladder, client should have easy access to bathroom that is clutter free so they could go back and forth. o Assess for skin breakdown and encourage skin care especially if client is immobile. 1 PREPARED BY: SOPHIA NICOLE UGTO o If retention problems, client may have to be taught on how to self-catheterization, to remove urine in the bladder. If urine stays in the bladder for too long, it is a good medium for bacterial growth leading to UTI and stone formation. o Maintain 1-2L of fluids a day to keep urine not concentrated. Bowel: o Increase fiber intake – lots for fruits and vegetables to keep stool soft and easy, bulky to pass o Stool softeners if needed o If patients are incontinent of stools – assess their skin and make sure it’s not breaking down and use barrier creams MEDICATIONS Beta interferon: decreases the number of relapses of symptoms by decreasing inflammation and the immune system’s response. o Risk for infection because it decreases WBCs o Drug Names: Avonex (Interferon Beta 1a) Rebif Betaferon Corticosteroids: for relapses of MS symptoms; help decrease inflammation and immune system response’ o Drug Names: Methylprednisolone, Prednisone Bladder Issues o Oxybutynin: anticholinergic that helps with overactive bladder by relaxing the bladder muscle to prevent contractions. o Bethanechol: cholinergic that helps with emptying the bladder by helping with bladder contraction Fatigue o Amantadine (antiviral & antiparkinsonian) – it has CNS effects that helps improve fatigue in patients with MS o Modafinil - CNS stimulant Spasms o Baclofen – skeletal muscle relaxant that acts centrally o Diazepam (Valium) Tremors o Propanolol: beta blocker Warn the diabetic patient because it mask-out symptoms of hypoglycemia such as tremors and shakiness. o Isoniazid: antibiotic used for infections, especially TB; helps with certain tremors in MS MYASTHENIA GRAVIS 2 PREPARED BY: SOPHIA NICOLE UGTO