Transversus Abdominis Plane (TAP) Block: Techniques & Efficacy
advertisement
 Block: Techniques & Efficacy")
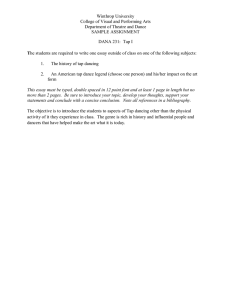
M a y THE JOURNAL OF NEW YORK SCHOOL 2 OF REGIONAL ANESTHESIA V o l u m 1 2 e 0 0 9 TRANSVERSUS ABDOMINIS PLANE (TAP) BLOCK By Karim Mukhtar, MB BCh, MSc, FRCA Royal Liverpool and Broadgreen University Hospitals, Liverpool U.K. Abd o min al field blocks h ave b een arou n d f or a lon g time an d h ave b een exten sively use d as th ey are mostly tech nically unch allen gin g. Th ey, h ow ever, provide limited an algesic fields, h en ce multiple injections are usu ally required. Tradition ally th ese blocks h ave blin d en d poin ts (pops) makin g th eir success unpredictable. Th e description of th e lan dmark techniqu e f or performin g transversu s abdominis plan e (TAP) block advoc ate d a sin gle en try poin t, th e trian gle of Petit, to access a n u mber of abd o min al w all n erves h en ce providin g more w idespread an algesia . (1) More recen tly, ultrasou n d guided TAP block h as be en describe d w ith pro mises of better localization an d de position of th e local an aesth etic with improved accuracy (2). The Journal of NYSORA 2009; 12: 28-33 TRANSVERSUS ABDOMINIS PLANE (TAP) BLOCK INTRODUCTION Abdominal field blocks have been around for a long time and have been extensively used as they are mostly tech nically u n ch allen gin g. Th ey, h ow ever, provide limited analgesic fields, hence multiple injections are usu ally required. Tra dition ally th ese blocks h ave blin d en d points (pops) makin g their success unpredicta ble . The description of the landmark technique for performing transversus abdominis plane (TAP) block advocated a single entry point, the triangle of Petit, to access a number of abdominal wall nerves hence providin g more w idespre a d an algesia . (1) More recen tly, ultrasound guided TAP block has been described with pro mises of better localization an d d ep osition of th e local anaesth e tic with improve d accur acy (2). arises from the anterior rami of spinal nerves T7 to L1. These include the intercostal nerves (T7 -T11), the subcostal nerve (T12), and the iliohypogastric and ilioinguinal nerves (L1). Anatomy Innervation of the anterolateral abdominal wall COPYRIGHT © 2009 BY THE NEW YORK SCHOOL OF REGIONAL ANESTHESIA (WWW.NYSORA.COM) VOLUME 12 28 Figure 1. Cutaneous innervation of the abdominal wall . Coloured region is mostly blocked by a single injection posterior TAP block. COPYRIGHT © 2009 BY THE NEW YORK SCHOOL OF REGIONAL ANESTHESIA (WWW.NYSORA.COM) VOLUME 12 28 THE JOURNAL OF THE NEW YORK SCHOOL OF REGIONAL ANESTHESIA (WWW.NYSORA.COM) TRANSVERSUS ABDOMINIS (TAP) BLOCK Th e anterior divisions of T7-T11 con tinu e from th e intercostal spac e to en ter th e ab do min al w all betw een th e intern al obliqu e an d transversu s ab do minis mu scles u ntil th ey reach th e rectus abdominis, which th ey perforate an d su pply, en din g as an terior cutan e ou s bran ch es su pplyin g the skin of the front of the abdomen. Midway in their course th ey pierce th e extern al obliqu e mu scle givin g off th e lateral cu tan eou s bran ch w hich divides in to an terior an d post erior bran ch es th at su pply th e extern al o bliqu e muscle and latissmu s dorsi respectively. Th e an terior bran ch of T12 co mmu n icates with th e iliohypogastric n erve an d gives a bran ch to th e pyramidalis. Its lateral cutaneous branch perforates the internal and extern al obliqu e mu scles an d d escen ds over th e iliac crest and supplies sensation to the front part of the gluteal region. Th e ilioh ypogastric n erve (L1) divides betw een th e intern al obliqu e an d tran sversu s ab do minis n ear th e iliac crest into lateral and anterior cutaneous branches, the former su pplyin g part of th e skin of th e gluteal region while the latter supplies the hypogastric region . Th e ilioin guin al n erve (L1) co mmu nicates with th e iliohypogastric nerve between the internal oblique and tran sversu s abd o minis n e ar th e an terior part of th e iliac crest. It su pplies th e u pper an d medial part of th e thigh an d part of the skin coverin g the genitalia.(3) Block Technique Figure 2. T7 to T12 spinal nerves pathway and branches in the abdominal wall Blind TAP The point of entry for the blind TAP block is the lumbar trian gle of Petit. Th is is situ ate d betw e en th e low er costal margin an d iliac crest. It is boun d an teriorly by th e extern al obliqu e mu scle an d posteriorly by th e latissmis dorsi. Th is technique relies on feeling double pops as the needle traverses th e extern al obliqu e an d intern al obliqu e muscles. A blunt needle will make the loss of resistance more appreciable. The aim of a TAP block is to deposit local an aesth etic in th e plan e b etw een th e in tern al obliqu e an d transversus abdominis mu scles targetin g th e spin al n erves in this plan e. Th e inn ervation to ab do min al skin , mu scles and parietal peritoneum will be interrupted. If surgery traverses the peritoneal cavity, dull visceral pain (from spasm or inflammation f oll owin g surgical insult) will still be experien ced. Th e block can be perf ormed blin d or u sin g the ultrasound Figure 3. Lumbar triangle of Petit between external oblique muscle and latissmis dorsi. CM: costal margin, IC: iliac crest. COPYRIGHT © 2009 BY THE NEW YORK SCHOOL OF REGIONAL ANESTHESIA (WWW.NYSORA.COM) VOLUME 12 29 THE JOURNAL OF THE NEW YORK SCHOOL OF REGIONAL ANESTHESIA (WWW.NYSORA.COM) Ultrasound- guided TAP The ultrasound probe is placed in a transverse plan e to th e lateral abd o min al w all in th e midaxillary lin e, betw een th e low er costal margin an d iliac crest. Th e u se of ultrasound allows for accurate deposition of the local anaesth e tic in the correct neurovascular plane. If prolon g ed analgesia is required beyon d the duration of a single shot of local anaesth etic , a catheter can be introdu ce d into the transversus abdominis plane through a touhy needle. After opening up the plane with 2 ml of saline, the catheter is introduce d aroun d 3 cm beyond the needle tip . Position is verified by injecting the local anaesth etic bolus (20ml). An infusion of a dilute local anaesth e tic is started at a rate of 7 to 10 ml per hour. TRANSVERSUS ABDOMINIS (TAP) BLOCK Performing the ultrasound-guided block Requirements -Ultrasou n d machin e with a high frequ en cy probe (10-5 MHz) -Ultrasound probe cover -Antiseptic for skin disinfection -Sterile ultrasound gel -Needle: 50 mm or 80 mm needle -20ml needle and injection tubing -20 to 30 ml local anaesthetic (any local anaesthetic concen tration , this block relies on local an aesth etic spread rather than concen tration ,i.e. is volume depen dan t.) Indications This block is indicated for any lower abdominal surgery inclu din g appen dectomy, h ernia repair, caesarean section (4), abdomin al hysterectomy (5) and prostatectomy (6). Efficacy in laparoscopic surgery has also been demon strated (7). Bilateral blocks can be given f or midlin e incision s or laparosc opic surgery. C are sh ou ld b e tak en not to exceed recommended safe doses of local anaesth e tic agent with bilateral injection s. There has been controversy in the literature regarding the spread and level of block achieved with a sin gle TAP in jection . Wh ilst early stu dies sh ow ed a T7 t o L1 spread with a sin gle posterior injection makin g th e block suitable f or midlin e abd o min al in cision s (8), oth er stu dies, h ow ever, f ailed t o d e mon strate a s prea d ce ph alad to T1 0 makin g it more suited for lower abdomin al surgery (9). Figure 4. Schematic view of an ultrasound-guided tranaversus abdominis plane block. EO: external oblique, IO: internal oblique, TA: transversus abdominis, LA: local anaesthestic In a small ca dav eric stu dy, T1 1, T1 2 an d L1 w er e most con sisten tly presen t in th e tran sversu s ab d o min is plan e, while T10 w as present in 50% of th e cases (10). It is reason able to expect a g oo d an algesic eff ect in th e region betw e en T10 an L1 f ollowin g a sin gle posterior in jection . Au g men tation with a su bcost al in jection will h elp attain a high er block u pto T7. Th e su bcostal TAP is a modification of th e origin al techniqu e in w hich th e ultrasou n d pro be is placed ju st ben eath th e costal margin an d parallel to it. Th e needle is th en introduced from th e lateral side of th e rectus mu scle in plan e of th e ultrasou n d b ea m an d 10 ml of local injected in to th e tran sversus abdominis plan e to exten d th e an algesia provide d by th e p osterior TAP block ab ove th e umbilicus (11). COPYRIGHT © 2009 BY THE NEW YORK SCHOOL OF REGIONAL ANESTHESIA (WWW.NYSORA.COM) VOLUME 12 30 M a y 2 0 0 9 THE JOURNAL OF NEW YORK SCHOOL OF REGIONAL ANESTHESIA V o l u m 1 2 e T ECHNIQUE Whilst the patien t is in the supine position , a high frequen cy ultrasou n d probe is placed transverse to the abdomin al wall betw een the costal margin and iliac crest. The image produced shows (from above downwards) skin, subcutaneous tissue, fat, external oblique, internal oblique, transversu s abdominis. The peritoneu m and bowel loops may also be visualized deeper to the muscles. Figure 6. Image of the abdominal wall. E0: external oblique, IO: internal oblique, TA: transversus abdominis COPYRIGHT © 2009 BY THE NEW YORK SCHOOL OF REGIONAL ANESTHESIA (WWW.NYSORA.COM) VOLUME 12 31 THE JOURNAL OF THE NEW YORK SCHOOL OF REGIONAL ANESTHESIA (WWW.NYSORA.COM) TRANSVERSUS ABDOMINIS (TAP) BLOCK Th e n eedle is in trodu ced in plan e of th e ultrasoun d probe directly un der th e probe an d advanced un til it reach es th e plan e betw e en th e in tern al obliqu e an d tran sversu s a bd o minis mu scles. Th e n e edle can also be in tro du ced a f ew cen timeters medial to th e prob e (a distance e quivalen t to th e de pth of th e plan e as view ed on th e ultrasou n d i ma g e). Th e pro be w ill h ave to f ollow th e n ee dle en try poin t me dially in its su perficial path an d is th en return ed to its origin al position in the midaxillary line as the needle is directe d deep er. U pon reachin g th e plan e, 2 ml of salin e is in jected to confir m correct n ee dle position after which 20 ml of local an aesth etic solution is in jected. Th e tran sversus abdominis plan e is visu alized expan din g with th e in jection ( appears as a hypoechoic space). Figure 7. Correct local anaesthetic deposition in the transversus abdominis plane. CLICK HERE TO VIEW VIDEO OF THIS TECHNIQUE. Complications Th er e h ave b een n o rep orted co mplication s to d ate w ith th e ultrasou n d gu ided t ech niqu e. A f ew complication s h ave been reported with blin d TAP block, th e most significant of which w as a case report of in trah epatic injection (12). Other complication s inclu de: intraperiton eal in jection , bow el h emato ma an d tran sien t femoral n erve palsy . Local an aesth etic toxicity could also occur du e to th e large volu mes required to perf or m this block especially if it w as don e bilaterally. As with any regional technique, careful aspiration will help avoid intravascular injections. COPYRIGHT © 2009 BY THE NEW YORK SCHOOL OF REGIONAL ANESTHESIA (WWW.NYSORA.COM) VOLUME 12 32 THE JOURNAL OF THE NEW YORK SCHOOL OF REGIONAL ANESTHESIA (WWW.NYSORA.COM) TRANSVERSUS ABDOMINIS (TAP) BLOCK R EFERENCES 1. Rafi A. Abdomin al field block: a new approa ch via the lumbar triangle. Anaesth esia 2001; 56: 102426. 2. Hebbard P, Fujiwara Y, Shibata Y, Royse C. Ultrasou n d-guid ed tran sversu s abd o minis plan e (TAP) block. Anaesthesia and Intensive Care 2007; 35: 616-7. 3. Gray H . An ato my of hu man th e bo dy. 12 th edition . New York. Bartleby.co m; 2000: 211-1 2 4. McDonnell JG, Curley G, Carney J, et al. The an algesic efficacy of tran sversus abdo minis plan e block after cesarean delivery: a randomized controlled trial. Anesth Analg 2008; 106:186 –9 1 5. Carney J, McDonnell JG, Ochana A, et al. The transversus abdominis plane block provides effective postoperative analgesia in patients un dergoin g total abd o min al hysterecto my. An esth Analg 2008; 107:2056-60 6. O'D on n ell BD , McD on n ell JG, McSh an e AJ. Th e tran sversu s ab do minis plan e ( TAP) block in op en retro pu bic prostat ecto my. R e g A nesth Pain Med 2006 ; 31:91 7. Mukh tar K, Sin gh S. Transversu s abdominis plan e block f or laparoscopic su rgery. Br J Anaesth 2009; 102(1):143-4 8. McDonnell J, Laffey J. Transversus Abdominis Plan e Block. Anesthesia and Analgesia 2007; 105: 883. 9. Shibata Y, Sato Y, Fujiwara Y, Komatsu T. Tran sversu s Abdo minis Plan e Block. Anesth esia and Analge sia 2007; 105: 883. 10. Tran TMN, Ivanusic JJ, Hebbard P, et al. Determination of spread of injectate after ultrasou n d-guide d transversu s ab do minis plan e block: a cadaveric study. Br J Anaesth 2009; 102(1): 123-7 11. H eb bard P. Tr an sversu s ab d o minis plan e ( TAP) block. 2007; Website: www.heartw e b.com.a u/d ow nloa ds TAPblock.pdf 12. Faro oq M, C arey M. A C ase of Liver Trau ma With a Blunt Regional Anesthesia Needle While Perf ormin g Tran sversu s Abd o minis Plan e Block Regional Anesthesia and Pain Medicine 2008; 33: 274-5. COPYRIGHT © 2009 BY THE NEW YORK SCHOOL OF REGIONAL ANESTHESIA (WWW.NYSORA.COM) VOLUME 12 33