- No category
Cultural Competence Theories in Nursing: Comparison Chart
advertisement
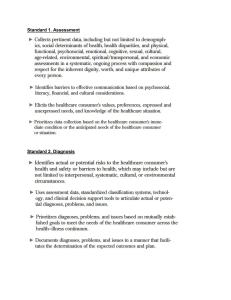
Title of theory Culture Care Diversity and Universality Cultural Competence Model Author of theory Year theory started Madeleine Leininger Larry Purnell 1950 1991 Reason for developing the theory To provide knowledge on these factors so that “culturally congruent care” will be acknowledged and delivered by modifying health care to individuals, families and communities. • • • Sunrise Enabler Model Name and illustration of the theoretical model • • to learn concepts and characteristics of culture; to define situations and understand the unique ethno-cultural environment; know the relationship of culture and health; to facilitate culturally-sensitive care, and; have basis for analysis of culture. Purnell Cultural Competence Model Assumptions of the theory 1. Care is the essence and the central dominant, distinct, and unifying focus of nursing. 2. Humanistic and scientific care is essential for human growth, wellbeing, health, survival, and to face death and disabilities. 3. Care (caring) is essential to curing or healing for there can be no curing without caring. (This assumption was held to have profound relevance worldwide.) 4. Culture care is the synthesis of two major constructs which guides the researcher to discover, explain, and account for health, wellbeing, care expressions, and other human conditions. 5. Culture care expressions, meanings, patterns, processes and structural forms are diverse but some commonalities (universals) exist among and between cultures. 6. Culture care values, beliefs, and practices are influenced by and embedded in the worldview, social structure factors (e.g. religion, philosophy of life, kinship, politics, economics, education, technology, and cultural values) and the ethnohistorical and environmental contexts. 7. Every culture has generic [lay, folk, naturalistic; mainly emic] and usually some professional [etic] care to be discovered and used for culturally congruent care practice. 8. Culturally congruent and therapeutic care occurs when culture care values, beliefs, expressions, and patterns are explicitly known and used appropriately, sensitively, and meaningfully with people of diverse or similar cultures. 9. Leininger’s three theoretical modes of care offer new, creative, and different therapeutic ways to help people of diverse cultures. 10. Qualitative research paradigmatic methods offer important means to discover largely embedded, covert, epistemic, and ontological culture care knowledge and practices. 1. All healthcare professions need similar information about cultural diversity. 2. All healthcare professions share the metaparadigm concepts of global society, family, person, and health 3. One culture is not better than another culture they are just different 4. Core similarities are shared by all cultures. 5. Differences exist within, between, and among cultures 6. Cultures change slowly over time 7. The primary and secondary characteristics of culture determine the degree to which one varies from the dominant culture. 8. If clients are coparticipants in their care and have a choice in health-related goals, plans, and interventions, their compliance and health outcomes will be improved. 9. Culture has a powerful influence on one's interpretation of and responses to health care. 10. Individuals and families belong to several cultural groups. 11. Each individual has the right to be respected for his or her uniqueness and cultural heritage. 12. Caregivers need both cultural-general and cultural specific information in order to provide culturally sensitive and culturally competent care. 13. Caregivers who can assess, plan, intervene, and evaluate in a culturally competent manner will improve the care of clients for whom they care. 14. Learning culture is an ongoing process that develops in a variety of ways, but primarily through cultural encounters (Campinha-Bacote, 2004). 15. Prejudices and biases can be minimized with cultural understanding. 11. Transcultural nursing is a discipline with a body of knowledge and practices to attain and maintain the goal of culturally congruent care for health and wellbeing. 16. To be effective, health care must reflect the unique understanding of the values, beliefs, attitudes, lifeways, and worldview of diverse populations and individual acculturation patterns. 17. Differences in race and culture often require adaptations to standard interventions. 18. Cultural awareness improves the caregiver's self- awareness 19. When individuals of dissimilar cultural orientations meet in a work or therapeutic environment, the likelihood for developing a mutually satisfying relationship is improved if both parties in the relationship attempt to learn about each other's culture. 20. Culture is not border bound. People bring their culture with them when they migrate. 21. Professions, organizations, and associations have their own culture, which can be analyzed using a grand theory of culture. Title of theory Author of theory Year theory started Reason for developing the theory The Process Of Cultural Competence In the Delivery Of Healthcare Services: A Model Of Care Transcultural Assessment Model Josepha Camphina-Bacote 1991 • to become culturally competent, the health care provider should integrate five processes including cultural awareness, cultural knowledge, cultural skill, cultural encounters and cultural desire Cultural Competence in the Delivery of Health Care Services Model Joyce Newman Giger and Ruth Davidhizar 1988, 2002 • to create an assessment tool to be used by the students and guide them in their communication with culturally diverse patients. Giger and Davidhizar’s Transcultural Assessment Model Name and illustration of the theoretical model Assumptions of the theory 1. Cultural competence is a process, not an event. Metaparadigm for the Model 2. 3. 4. 5. Cultural competence consists of five constructs: cultural awareness, cultural knowledge, cultural skill, cultural encounters, and cultural desire. There is more variation within ethnic groups than across ethnic groups (intra-ethnic variation). There is a direct relationship between the level of competence of health care providers and their ability to provide culturally responsive health care services. Cultural competence is an essential component in rendering effective and culturally responsive services to culturally and ethnically diverse clients. 1. Transcultural nursing: A culturally competent practice field that is client centered and research focused. 2. Culturally competent care: A dynamic, fluid, continuous process whereby an individual, system, or health care agency finds meaningful and useful care delivery strategies based on knowledge of the cultural heritage, beliefs, attitudes, and behaviors of those to whom they render care (Davidhizar & Giger, 1998). Cultural competence connotes a higher, more sophisticated level of refinement of cognitive skills and psychomotor skills, attitudes, and personal beliefs. To develop cultural competency, it is essential for the health care professional to use knowledge gained from conceptual and theoretical models of culturally appropriate care. Attainment of cultural competence can assist the astute nurse in devising meaningful interventions to promote optimal health among individuals regardless of race, ethnicity, gender identity, sexual identity, or cultural heritage. 3. Culturally unique individuals: An individual is culturally unique and as such is a product of past experiences, cultural beliefs, and cultural norms. 4. Culturally sensitive environments: Culturally diverse health care can and should be rendered in a variety of clinical set- tings. Regardless of the level of care, primary, secondary, or tertiary knowledge of culturally relevant information will assist in planning and implementing a culturally competent treatment regime. 5. Health and health status: Health and health status is based on culturally specific illness and wellness behaviors. An individual’s cultural beliefs, values, and attitudes all contribute to the overarching meaning of health for each individual. Title of theory Author of theory Year theory started Reason for developing the theory Name and illustration of the theoretical model Cultural Competence and Confidence (CCC) Model Bureaucratic Caring Theory Marianne R. Jeffreys 2004 • to interrelate concepts that explain, describe, influence, and/or predict the phenomenon of learning (developing) cultural competence and incorporates the construct of TSE (confidence) as a major influencing factor Cultural Competence and Confidence Model Marilyn Anne Ray 1981 • To illustrate caring as not only humanistic, ethical, spiritual, social, cultural and educational but also as part of the structural. Political, economic, legal and technological characteristics of a complex organization. Holographic Theory of Bureaucratic Caring Assumptions of the theory 1. Cultural competence is an ongoing, multidimensional learning process that integrates transcultural skills in all three dimensions (cognitive, affective, and practical), involves transcultural self-efficacy (confidence) as a major influencing factor, and aims to achieve cultural congruent care. 2. Transcultural self-efficacy is a dynamic construct that changes over time and is influenced by formalized exposure to culture care concepts (transcultural nursing)." 3. The learning of transcultural nursing skills is influenced by self-efficacy perceptions (confidence). 4. The performance of transcultural nursing skill competencies is directly influenced by the adequate learning of such skills and by transcultural self-efficacy perceptions. 5. The performance of culturally congruent nursing skills is influenced by self-efficacy perceptions and by formalized educational exposure to transcultural nursing care concepts and skills throughout the educational experience. 6. All students and nurses (regardless of age, ethnicity, gender, sexual orientation, lifestyle, religion, socioeconomic status, geographic location, or race) require formalized educational experiences to meet culture care needs of diverse individuals." 7. The most comprehensive learning involves the integration of cognitive, practical, and affective dimensions. 8. Learning in the cognitive, practical, and affective dimensions is paradoxically distinct yet interrelated." 9. Learners are most confident about their attitudes (affective dimension) and least confident about their transcultural nursing knowledge (cognitive dimension)." 1. Nursing is holistic, relational, spiritual, and ethical caring that seeks the good of self and others in complex community, organizational, and bureaucratic cultures. Dwelling more deeply with the nature of caring reveals that the foundation of spiritual caring is love. Through knowledge of the inner mystery of the inspirational life within, love calls forth a responsible ethical life that enables the expression of concrete actions of caring in the lives of nurses. As such, caring is cultural and social. Transcultural caring encompasses beliefs and values of compassion or love and justice or fairness, which find significance in the social realm, where relationships are formed and transformed. Transcultural caring serves as a unique lens through which human choices are seen, and understanding in health and healing emerges. Thus, through compassion and justice, nursing strives toward excellence in the activities of caring through the dynamics of complex cultural contexts of relationships, organizations, and communities 2. A person is a spiritual and cultural being. Persons are created by God, the Mystery of Being, and they engage co-creatively in human organizational and transcultural relationships to find meaning and value 3. Health provides a pattern of meaning for individuals, families, and communities. In all human societies, beliefs and caring practices about illness and health are central features of culture. Health is not simply the consequence of a physical state of being. People construct their reality of health in terms of biology, mental patterns, characteristics of their image of the body, mind, and soul, ethnicity and family structures, structures of society and community (political, economic, legal, and technological), and experiences of caring that give meaning to lives in complex ways. The social organization of health and illness in society (the 10. Novice learners will have lower self-efficacy perceptions than advanced learners." 11. Inefficacious individuals are at risk for decreased motivation, lack of commitment, and/ or avoidance of cultural considerations when planning and implementing nursing care. 12. Supremely efficacious (overly confident) individuals are at risk for inadequate preparation in learning the transcultural nursing skills necessary to provide culturally congruent care. 13. Early intervention with at-risk individuals will better prepare nurses to meet cultural competency. 14. The greatest change in transcultural self-efficacy perceptions will be detected in individuals with low self-efficacy (low confidence) initially, who have then been exposed to formalized transcultural nursing concepts and experiences. healthcare system) determines the way that people are recognized as sick or well. It determines how health professionals view health and illness, and how individuals view health and illness. Health is related to the way that people in a cultural group or organizational culture or bureaucratic system construct reality and give or find meaning
 0
0
advertisement

Download
advertisement
Add this document to collection(s)
You can add this document to your study collection(s)
Sign in Available only to authorized usersAdd this document to saved
You can add this document to your saved list
Sign in Available only to authorized users