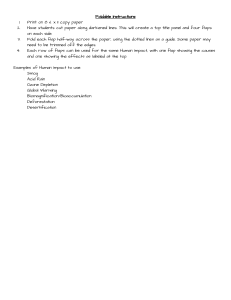
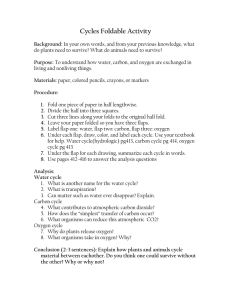
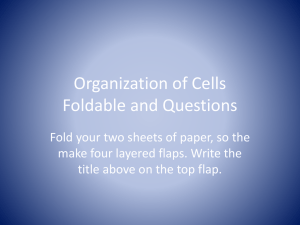
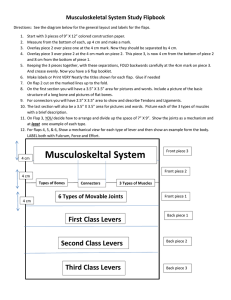
0733-8635/98 $8.00 EXCISION AND REPAIR + .OO NASAL ANATOMY AND RECONSTRUCTION Dan H. Meirson, MD Reconstruction of the nose poses a vitally important challenge to the dermatologic surgeon. This is the most prominent feature on the human face. Due to the high incidence of cutaneous malignancies in this area, knowledge of unique anatomic considerations of the nose and the ability to apply this knowledge are essential to repair defects in this region. The nose has many features such as differing surfaces that make reconstruction challenging, because these surfaces are in close proximity and are both convex and concave.27 Because the nose does not have a great deal of tissue laxity, making closure of defects difficult, its texture, with its high concentration of sebaceous glands, makes tissue matches for full-thickness skin grafts and local flaps challenging. This article reviews the anatomy and the anesthesia of the nose. The reconstruction of defects of the nose by secondary intention, primary closures, grafts, and local flaps is also discussed. ANATOMY The nose is divided into upper and lower portions. The upper two-thirds of the nose is divided into the root, dorsum, and lateral sidewall. The lower one-third is the lobule, which can be subdivided into the tip, alae nasi, columella, alar rim, nasal sill, and soft Skin in the upper portion triangle (Fig. 1).21 of the nose is mobile and loosely attached to the bony framework below; therefore, the limiting factor in closure of this area is the underlying prominence of the bony skeleton. In contrast, the skin on the inferior aspect of the nose is thick and densely adherent to the underlying cartilaginous structures.6 Consequently, primary closure of defects in this area can result in distortion of the alar rim and the nasal tip. Beneath the skin and muscle of the nose is the bony-cartilaginous infrastructure that gives the nose its shape and functional integrity. This infrastructure consists of the paired nasal bones superiorly. The bones form the upper border of the pyriform aperture, which rings the opening of the nose into the skull. Beneath these rigid nasal bones are the movable, paired lateral cartilages, which are supported by the septa1 cartilage. Beneath the lateral cartilages are the alar cartilages, which are both extremely mobile. Alar cartilages give the lower nose its shape and contours. The medial crura of the alar cartilage form the columella. The lateral crura form the alar rim. The area between the crura is the hinge area where the crura join. This area forms the dome that becomes the nasal tip. The lateral crura then pass obliquely and superiorly from the dome and determine the contour of the alae nasi (Fig. 2). The majority of the alar rim contains no cartilage. This portion of the alar Private Practice, Pompano Beach, Florida DERMATOLOGIC CLINICS - VOLUME 16 NUMBER 1 *JANUARY 1998 91 92 MEIRSON 6 2 triangle Columella Alar rim Colnmella Nasolabial fold , A B Figure 1. A and 6, The nose and its components. rim consists of tissue that has a thick dermis, numerous sebaceous glands, and muscle. There is very little subcutaneous fat in this area.*l There are numerous aesthetic units into which the nose is divided. The aesthetic subunits are the root, dorsum, lateral sidewalls, nasal tip, alae nasi, and columella. These areas create important considerations for reconstruction. The subunits are bordered by contour lines that represent where a concave and convex surface meet. These are the nasofacial sulcus, lateral ridge, and alar rim (Fig. 3).2 The re-creation and lack of distortion of these subunits are essential to reconstruction. Often when a large portion of a subunit is lost, it may create a better aesthetic result to excise the subunit and reconstruct the entire area? Relaxed skin tension lines are also important for proper nasal reconstruction. The relaxed skin tension lines are the lines in which scars are best hidden when reconstruction is performed.17 On the nose, these lines i=- run horizontally at the nasal root and then run obliquely from the medial canthus, crossing the lateral sidewall, where they become vertical along the dorsum of the nose (Fig. 4). When attempting primary closures on the nose, it is important to follow the relaxed skin tension lines when possible. ANESTHESIA The nose can be anesthetized by the use of three nerve blocks. The nose is supplied by branches of the ophthalmic and maxillary branches of trigeminal nerve V. Two branches of the ophthalmic nerve, the infratrochlear and the external nasal branches of the anterior ethmoidal nerve, are responsible for a large portion of noses' sensory innervation. The infratrochlear nerve is a branch of the nasociliary portion of the ophthalmic nerve. It emerges above the medial canthal ligament and runs medially across the nasal dorsum. Nasal bone Lateral cartilage Nasal Ti0 I Septal angle Medial c m A B Figure 2. A and 6,The infrastructure of the nose. NASAL ANATOMY AND RECONSTRUCTION Nasofacial Sulcus Lateral Ridge 93 Lateral Sidewall Dorsum Alar Crease Tip Figure 3. The aesthetic units and contour lines of the nose. This nerve supplies the root, upper bridge, and upper sidewalls. The external nasal branches of the anterior ethmoidal nerve emerge on the surface of the nose between the nasal bones and lateral nasal cartilages, which supply a section of the nasal dorsum and the nasal tip. The infraorbital nerve is the largest terminal branch of the maxillary division. This nerve innervates the nasal ala, columella, and lower portions of the lateral sidewalls on the nose (Fig. 5).21,22, 25 The superior aspect is anesthetized using a bilateral infratrochlear nerve block. This is accomplished by inserting a needle in the center of the root and injecting towards each medial canthus. Anesthesia of the nasal tip is accomplished by a fanning injection at the junction of the nasal bones and the upper lateral cartilages. This anesthetizes the external nasal branch of the anterior ethmoidal nerve. Finally, an infraorbital nerve block can be performed either intraorally or percutaneously. When anesthetized percutaneously, the nerve is anesthetized by injecting slightly lateral to the ala and then up the nasofacial sulcus. It can be administered intraorally (by inserting the needle in the canine fossa and advancing it slowly to the vicinity of the infraorbital foramen) and can be less painful for the patient.25This foramen is located in the midpupillary line 1 centimeter below the infraorbital rim. RECONSTRUCTION Burget5 defined seven principles unique to facial reconstruction. Figure 4. The relaxed skin tension lines of the nose. 1. The normal facial contour, learned from daily observation of normal faces, is the desired end result and nothing else accepted. 2. A missing facial part is restored in three dimensions. For each layer the raw material that most matches the missing layer is chosen. 3. Flaps and grafts are designed from exact three-dimensional patterns using normal facial features as a template rather than geometric forms or letters of the alphabet. 4. Donor scars are camouflaged or hidden. 5. When practical, entire topographic facial units are replaced by a single flap or graft. 6. Cartilage grafts are used to create sur- 94 MEIRSON OPHTHALMIC N. (V1) Infratrochlear n. External nasal branch of the anterior ethrnoidal n. MAXILLARY N. (VZ, Infraorbital n. Figure 5. The sensory innervation of the nose. face contours and to brace the soft tissues against contraction or collapse. 7. As a final reconstructive step subcutaneous sculpting is employed to refine the contour of the restored part.5 Therefore, it is imperative that the dermatologic surgeon adhere to these seven principles when reconstructing defects of the nose. This is essential to provide nasal reconstruction with proper aesthetic and functional results. HEALING BY SECONDARY INTENTION The key to proper healing by secondary intention is wound management. Each day the wound should be cleansed with 3% hydrogen peroxide solution to soften and remove crusts. Then an antibiotic ointment such as polymyxin B-bacitracin (Polysporin) is applied to the defect. The area is then covered with a semiocclusive bandage (Telfa, Kendall Healthcare, Manfield, MA) or a Band-Aid. These steps are repeated until the’ wound is healed.28 There are important considerations when deciding if a wound will heal with a good aesthetic result by secondary intention. The surgeon must consider location, depth, and whether the defect is on a concave or a convex surface. The defects that heal best by secondary intention are on concave surfaces. Nasal defects on convex surfaces do not heal as well by secondary intention and may leave irregular or depressed scars, especially if the defect is deep and involves cartilage or bone.2,28 The areas that heal best by secondary intention are lesions on the lateral root of the nose adjacent to the medial canthus and the alae nasi along the alar crease. Even deep defects in these regions heal extremely well with good aesthetic results.28 PRIMARY CLOSURE Primary closure is useful for defects on the nose; however, the subunits on the upper nose are better suited to primary closure than the subunits on the lower portion of the nose, where the skin is thick and immobile. When closures on the upper portion of the nose are performed, it is important to follow the relaxed skin tension lines of the nose and place the scars within them. Therefore, the fusiform closure should be transverse across the nasal root, vertical along the nasal dorsum, and oblique on the sidewall^.^ An important consideration when performing fusiform closures on the nasal sidewalls is to avoid placing excessive tension on the wound causing retraction of the alar rim and a subsequent asymmetric appearance.28 Defects on the nasal dorsum can be repaired vertically; however, when closing an ellipse in this location, it is important not to NASAL ANATOMY AND RECONSTRUCTION place the superior pole of the ellipse at the junction of the nasal bones and lateral cartilages. If the superior pole is placed at this location, it will cause a protrusion. Because the tension vector of this closure will be along the dorsum, it will tend to depress the tissue centrally, causing the appearance of the superior pole to be exaggerated. Also, the inferior pole should not end at the nasal tip; it should either end superior to it or be continued onto the columella. Ending the inferior pole on the nasal tip can cause a distortion of this subunit. Owing to these caveats, it is often necessary to extend these fusiform closures beyond the usual 3:l length to defect ratio (Fig. 6).28 Only small defects on the lower one-third of the nose can be reconstructed primarily, due to the thick, immobile skin in this area. When defects on the tip or alae nasi are closed primarily, excessive tension should not be present. This may cause an upward retraction of these subunits and an asymmetric appearance. When larger defects in these subunits are reconstructed primarily, distortion of the nasal tip or alar rim may result. RECONSTRUCTION USING SKIN GRAFTS Skin grafting began approximately 2500 to 3000 years ago in India. These ancient surgeons used skin grafts from the gluteal region 95 to replace noses that had been amputated for punishment of theft or ad~1tery.I~ Although grafts for this purpose are not commonly seen today, skin grafting has evolved into an important tool in nasal reconstruction. There are three types of skin grafts, the split-thickness skin graft, full-thickness skin graft, and composite graft. Split-Thickness Skin Grafts Split-thickness skin grafts consist of epidermis and a partial thickness dermis. They have the advantages of containing less tissue that requires revascularization than full-thickness skin grafts. Also, they can be placed over surfaces with a limited vascular supply such as bone or cartilage. However, there are disadvantages that make split-thickness skin grafts of little use in nasal reconstruction.* These grafts tend to be white, smooth, and have a great deal of graft contraction over time.I4 This contraction can be deforming to the adjacent tissue; therefore, due to the poor aesthetic qualities of this method of grafting, split-thickness skin grafts are a poor choice for nasal reconstruction. Full-Thickness Skin Grafts Full-thickness skin grafts are composed of epidermis and a full-thickness dermis, includ- Figure 6. Primary closure. A, Defect on the nasal dorsum. 5, Vertical primary closure on the nasal dorsum. 96 MEIRSON mature follicle^.^^ Also, if the recipient area ing adnexal structures. This graft is more has a great deal of sebaceous hyperplasia, slowly revascularized than a split-thickness there is no donor site that will provide a skin graft; therefore, an adequate blood supproper texture match for this defect. As stated ply in the recipient bed is essential for surpreviously, defects in the nasal tip, medial vival of the graft. These grafts develop a relacanthus, and alar crease do extremely well tively normal skin texture when the donor with skin grafts. If a defect in this region sites are chosen appropriately. takes up greater than 50% of the subunit, the Full-thickness skin grafts are suited for sucosmetic result is improved when the entire perficial, well-circumscribed defects. Howsubunit is excised and then grafted. ever, they are poor choices over large surfaces There are many varying techniques in fullof exposed cartilage or bone due to the relatively poor blood supply in these structure~.~ thickness skin grafting; however, some basic principles are observed in all the differing Therefore, over these surfaces, full-thickness methods. First, a template of the recipient site skin grafts will not heal uniformly. can be made with paper, foil, surgical gauze, In nasal reconstruction, the sites that do or Telfa pressed into the defect. The template best with full-thickness skin grafts are the is applied to the donor site prior to the infilnasal tip, medial canthus, and alar crease. The tration of local anesthetic, then the area is usual donor sites used for these grafts are marked with a surgical marker. A 5% to 10% the preauricular area, postauricular area, and allowance for graft shrinkage is made, and a supraclavicular area.I4Other donor sites such slightly larger donor graft is obtained. The as the nasolabial fold have been reported as donor site is then prepared and anesthetized donor sites for defects on the nasal tip.3 with lidocaine with epinephrine 1:200,000. The most versatile donor site is the preauEpinephrine can be used without any comricular area, because it provides suitable texpromise in graft survival.24The donor site is ture and tissue match for nasal reconstructhen closed primarily, and the graft is sutured tion. This is due to its thickness and solar into the recipient site using 5-0 or 6-0 nylon damage that may mirror the nasal subunit sutures (Fig. 7). The graft must then be immobeing reconstructed. It is important that when bilized to prevent hematoma and seroma fora donor graft is taken from this area, it does mation. This is done by using a pressure not contain mature hair follicles that could dressing to hold the graft in place and proresult in hair growing in the recipient site. vide tissue apposition. Usually, a tie over bolMost people have a 1 to 2 centimeter area in ster dressing is used, which can consist of the preauricular area that is devoid of many Figure 7. Full-thickness skin graft. A, Defect on the nasal ala. €3, Reconstruction with a full-thickness skin graft sutured into place. NASAL ANATOMY A N D RECONSTRUCTION A 97 6 Figure 8. Composite graft. A, Full-thickness defect on the alar rim. 6,Composite graft sutured into place to reconstruct the alar rim. Xeroform gauze and sutures. However, foam rubber, cotton balls, and sponges have all been used as pressure dressings with a nonadherent dressing on the graft. It is important to achieve proper hemostasis before suturing the graft in place. However, it is necessary to avoid excessive cautery in the recipient site, which could impede reva~cularization.~ The bolster dressing and sutures are removed at approximately 7 days. If a total graft is not obtained, then the resulting defect will heal by secondary intention and can result in some scarring.2 then trimmed and sutured in place at the recipient site and the vascular bed is prepared with extreme caution. Any excessive cauterization should be removed, and care is needed to make sure only essential cautery is used.'" Then the graft is sutured into place with a few fine absorbable sutures on the inner surface, and the outer surface is sutured in place with a 5-0 or 6-0 nylon suture.23The composite graft is extremely susceptible to any injury or trauma. A packing gauze can be placed in the nasal vestibule, and the outer surface can be covered with antibiotic ointment and a nonadherent dressing. The sutures should be removed at approximately 1 week (Fig. 8). Composite Grafts A composite graft is defined as consisting of two differing types of tissue. The standard composite graft for a full-thickness defect of the nasal ala is a graft taken from the ear consisting of skin and cartilage. Composite grafts require rapid revascularization, but are successful owing to the rich vascular supply of the recipient (nose) and the donor (ear). The largest size these grafts can be is approximately 2.5 centimeters in size. Grafts larger than this size will usually necrose and rarely s ~ r v i v eHowever, .~ the smaller the composite graft, the quicker the revascularization and the better chance of survival.16 If a small composite graft is needed, the usual donor location is the helical crus. For larger defects, donor sites on the helical rim, antihelix, or tragus can be used.I4 The composite graft is harvested, and the donor site is then reconstructed primarily. The graft is FLAP RECONSTRUCTION Local flaps are important reconstructive considerations for defects on the nose. For deep defects involving significant amounts of exposed cartilage or bone, the only two options are a primary closure or a flap. Flaps have many distinct advantages over grafts.I2 First, they carry their own blood supply and are not dependent on the vascular supply of the defect. Also, they provide a reliable tissue match since they are from adjacent skin. If flaps are planned appropriately and the scars are placed in the proper lines, they can provide a far better cosmetic result than a fullthickness skin graft or a composite graft.* Local flaps on the nose are divided into three basic types: advancement, rotation, and transposition flaps. The majority of flaps in nasal reconstruction are derived from these 98 MEIRSON three types of flaps. In the discussion that follows, each subunit and some of the flaps used in its reconstruction are addressed. inverted V in the glabellar region. The flap is then elevated and rotated into the defect, and the incision lines in the glabella are closed in an inverted Y. This can place them in the vertical glabellar furrow, and the flap is suAlso, tured in place in the defect (Fig. 11).2~22 a superiorly based rotation flap from this area can be performed leaving an incision line in the glabellar furrow (Fig. 12). Finally, if there is sufficient tissue laxity in the glabellar region, an advancement flap can be performed. A simple advancement flap can be used for midline defects in this subunit. The incision lines are made from the lateral aspects of the defect superiorly into the glabellar furrows. The flap is then undermined, and Burow’s triangles are removed superiorly. The tissue is then advanced inferiorly into the defect, and the flap is sutured in place (Fig. 13). Flap Reconstruction of the Nasal Root Defects of the nasal root to the medial canthal regions can be reconstructed using a variety of glabellar flaps.22These flaps are excellent reconstructive options. This is due to the fact that the skin in the glabella is usually mobile, nonhair bearing, and there is tissue available to borrow in this area. Also, the vertical furrows are excellent places to hide incision lines. The glabellar transposition flap, rotation flap, and advancement flap are glabellar flaps that can be used in reconstruction. A glabellar transposition flap is commonly used to reconstruct the nasal root. This can be performed as a banner transposition flap where the flap is placed into the defect from the glabellar area. The secondary defect is then reconstructed in the glabellar furrow, and the flap is then sutured into place in the defect. This is an excellent reconstructive option for the root and medial canthal regions, because the superior limb of this flap is in the glabellar furrow and the other limbs of the flap end inferiorly in the relaxed skin tension lines (Figs. 9 and l0).l1 Another glabellar flap is a rotation flap. This can be done as the V-to-Y glabellar flap or a standard rotation flap from the loose glabellar skin. This flap is superiorly based and rotates the skin from the glabella into the defect on the nasal root. In the V-to-Y glabellar flap the incisions are first made as an A Flap Reconstruction of the Lateral Sidewalls A variety of flaps work well for defects on the lateral sidewalls of the nose. Transposition flaps are useful in this subunit for defects that are small. Rotation flaps from the glabellar region can be used to repair defects, especially on the superior portion of the lateral sidewall. However, for large defects, the flaps that are most effective are the lateral cheek advancement and rotation flaps. In these flaps, tissue is advanced superiorly and medially into the defect. This is done by using the cheek tissue, especially in older persons in whom there is increased laxity. The lateral cheek advancement flap is performed by incising the tissue along the nasolabial fold. The B C Figure 9. A and 6,Glabellar transposition flap. A, Defect and proposed flap. B, Flap movement. C, Flap sutured into place. NASAL ANATOMY AND RECONSTRUCTION 99 Figure 10. A, Glabellar transposition flap. Defect and proposed flap. 13,Flap movement demonstrated prior to suturing. C, Flap sutured into place and the secondaty defect reconstructed. entire nasolabial fold should be incised, and Burow’s triangle should be removed at the inferior aspect. The second limb of this flap is cut along the border of the lower eyelid and the cheek. Then the flap is advanced medially and superiorly into the defect and sutured into place. It is important that wide undermining be performed so that the flap is not under a great deal of tension and to prevent necrosis of the flap tip (Fig. 14).24 Also, inferiorly based rotation flaps are use- ful for defects in this region. They are performed by elevating the tissue along the nasolabial fold into the defect. Burow’s triangle is then removed inferiorly and the skin is rotated superiorly into the defect. The ‘dog-ear’ can be removed along the infraorbital rim. It is important that the flap be cut along the nasolabial fold below the oral commissure. Otherwise, subsequent scar contracture can cause retraction of the oral commissure superiorly. 100 MEIRSON 'I A B C Figure 11. Glabellar rotation flap. V- to -Y type. A, Defect on the nasal root and proposed flap. 5, Flap movement. C,Flap sutured into place in the defect. Figure 12. Glabellar rotation flap. A, Defect on the nasal root and proposed glabellar rotation flap. 6,Flap sutured into place in the defect. Figure 13. Advancement glabellar flap. A, Defect and proposed flap. 5, Flap movement. C,Flap sutured into place. NASAL ANATOMY AND RECONSTRUCTION . ----- 1 A 101 \ C Figure 14. Cheek advancement flap. A, Defect and proposed flap. 6, Flap movement. C, Flap sutured into place. Flap Reconstruction of the Nasal Dorsum There are a variety of options for closure of defects on the nasal dorsum. Among these are the advancement flap, which advances tissue from the glabella and the upper nose into the defect. The tissue is then incised and stretched into the defect. The incisions are made along the lateral ridge of the nose at the border of the dorsum and lateral sidewall subunits. The incision extends into the glabellar furrows where Burow's triangles are removed. This enables the limbs to be placed in anatomic lines and to use the glabellar skin. Rotation flaps that use glabellar skin can also be applied. In reconstruction of a defect on the nasal dorsum, the incision lines of the flap should be along the lateral ridge of the nose and into the vertical glabellar furrow.7,24 To decrease the tension on this closure, it is important that the flap length is significantly longer than the diameter of the defect. A backcut on this flap is needed to allow adequate tissue m ~ v e m e n tIf. ~the defect is small and less tissue movement needed, the flap can be shortened, and the backcut can be along the nasal root (Fig. 15). Other useful flaps in this area are transposition flaps. These closures are often preferred because they can reconstruct the defect on the dorsum under little tension and place the secondary defect on the loose forehead or glabellar skin. Variations of transposition flaps are the rhombic flaps, Webster 30-degree flaps, Dufuromental flaps, Limberg flaps, and banner flaps. All can be used in this subunit with success. The important feature of choosing the proper repair should be that the final incision lines provide a cosmetically acceptable result. Flap Reconstruction of the Nasal Ala The nasal ala is a subunit'that is convex, devoid of cartilage, and firmly bound to the underlying tissue. As stated previously, primary closures can only be performed for very small defects; otherwise a deformity of the alar rim will result. The various flaps that can be used are usually transposition flaps. These include single transposition flaps such as the banner, rhombic, Webster, and nasolabial flaps. The double transposition or bilobed flap is used for larger defects. The rhombic flap is a transposition flap that is useful for small defects on the ala.I3 This is due to the immobility of the skin along the lower third of the nose.z6In this flap the tissue is placed in the defect after first measuring the defect diameter then designing the flap so that the incision lines will end in cosmetically acceptable lines. The flap is then undermined and brought into the defect. The secondary defect is reconstructed, the flap is sutured into place, and the "dog-ear" is then repaired (Figs. 16 and 17). For larger defects on the alae nasi, a single transposition flap from the nose is not useful. A bilobed flap or nasolabial flap is then needed. The bilobed flap is well suited for defects on the ala. This double transposition flap allows tissue to be moved over a longer distance than a single transposition flap, allowing the defect to be reconstructed with tissue that is an excellent texture and color 102 MEIRSON Figure 15. Rotation flap on the nasal dorsum. A, Defect. 6, Rotation flap sutured into place. match." It also allows for greater tissue movement and the closure of defects on the lower one-third of the nose without tissue distortion. There are two designs of this flap. In one flap design, the tissue is transposed over a total of 180 degrees with each limb moving 90 degrees (Fig. 18). This design can result in pincushioning or a trapdoor deformity of the flap, which is the dome-like elevation of the flap as compared to the surrounding tissue.26 A way to minimize this deformity is to change the flap design, with each flap being A B rotated 45 degrees into the defect.l3,24 The entire area must be widely undermined to allow for tissue movement and to decrease pincushioning or the trapdoor deformity. The secondary defect is then reconstructed, and both flaps are then sutured into place (Figs. 19 and 20). This modification decreases the risk of pincushioning and is an excellent choice for defects on the lower one-third of the nose, 1.5 centimeters or less.26 Another extremely useful flap for defects on the alae nasi is the nasolabial flap. This is C Figure 16. Rhombic flap on the nasal ala. A, Proposed rhombic flap. 6, Flap movement. C, Flap sutured into place. NASAL ANATOMY AND RECONSTRUCTION 103 Figure 17. Rhombic flap. A, Defect and proposed flap. 13, Flap sutured into place. (Courtesy Blas Reyes, MD, Miami, Florida.) a transposition flap that makes use of the lax medial cheek skin. This tissue is abundant in older persons. In these patients large flaps can be created to repair alar defects. The secondary defect can be closed in the nasolabial fold without cosmetic deformity. In the reconstruction of defects on the ala, the best design of this flap is a superiorly based nasolabial flap.12The flap is cut along the nasolabial fold and superiorly along the cheek. The base of the flap must extend superiorly to the top of the primary defect. The area is then exten- A sively undermined, and the tissue is transposed into the defect above this fixed point. The secondary defect is reconstructed along the nasolabial fold, and the flap is sutured in place in the defect (Figs. 21 and 22). Full-thickness defects of the ala can be reconstructed with a modification of this technique. This is done by lengthening the flap and then folding the distal aspect of the flap inward to reconstruct the inner lining of the ala.', l2 The area is then sutured into place to reconstruct the missing ala. B C Figure 18. Bilobed transposition flap with 180 degrees of tissue movement. A, Defect and proposed flap. B, Flap movement. C, Flap sutured into place. 104 MEIRSON A B C Figure 19. Bilobed transposition flap on the nasal ala with 90-degree total flap movement. A, Defect and proposed flap. 6, Flap movement. C,Flap sutured into place. While the nasolabial flap is extremely useful for defects on the ala, it has complications. The most common is a trapdoor phenomenon. As discussed previously in this article, this is the dome-like elevation of the undersurface of the flap.13This flap may need revision to correct this trapdoor. This is done by defatting or dermabrasion of the area. Also, this flap can cause the obliteration of the nasofacial groove. This occurs most commonly when the flap is not designed correctly and the base is not superior to the defect along If this does occur, the the nasofacial SU~CUS.*~ flap may need revision and debulking to recreate the nasofacial sulcus.ls Flap Reconstruction of the Nasal Tip The nasal tip provides many challenges for reconstruction. Small defects can be reconstructed with transposition flaps such as banner or rhombic flaps. Also, the bilobed flap can be extremely useful. This flap can use the tissue from the dorsum and the glabella to reconstruct this area. It can be used as a classic bilobed flap by moving each limb of the Figure 20. A and 6,Bilobed transposition flap on the nasal ala. A, Defect and proposed flap. 6, Flap sutured into place. (Courtesy Leonard H. Goldberg, MD, Houston, Texas.) NASAL ANATOMY AND RECONSTRUCTION A B 105 C Figure 21. Nasolabial flap for defect on the nasal ala. A, Defect on the nasal ala and the proposed flap. 6, Flap movement. C,Flap sutured into place. flap 90 degrees into the defect for a total of 180 degrees. Also, the flap angles can be decreased as described earlier. Another flap that is useful in reconstruction of the nasal tip is a rotation flap, which is the dorsal nasal flap. This uses the skin of the upper two-thirds of the nose and the glabella and rotates it or slides it onto the nasal tip.l9rZ6 This is done by incising the flap along the lateral ridge and then superiorly. The backcut is made into the glabellar area. Wide un- dermining is then necessary, and this allows for proper movement of the flap.l5-24 Smaller defects on the tip can be reconstructed using a variation of this flap that is backcut along the nasal bridge (Fig. 23). The excellent vascular supply of the nose allows for the flap to have a significant backcut enabling tissue movement and still allow for its survival. Another flap with limited usefulness on the nasal tip is the Rintuala flap, which is an advancement flap used to resurface the nasal Figure 22. Nasolabial flap for defect on the nasal ala. A, Defect on the nasal ala and the proposed flap. B, Flap sutured into place. (Courtesy Leonard H. Goldberg, MD, Houston, Texas.) 106 MEIRSON Figure 23. Dorsal nasal flap. A, Defect and proposed flap. 6,Flap sutured into place. tip. This flap is incised along the sides of the nasal dorsum (the lateral ridges) and ends in the glabellar furrows where Burow's triangles are removed (Fig. 24). However, this flap has many disadvantages. There can be ischemia and flap necrosis at the distal aspect of the flap, which can lead to scarring. Also, it can be difficult in many patients to achieve significant advancement of the flap to reconstruct large defects on the tip.I3 The midline forehead flap is useful for large defects on the nasal tip. This is a delayed flap in which the pedicle is based on the supply of the supratrochlear artery. First, the nasal tip defect is measured and then drawn on the upper mid-forehead. This should be at a distance above the eyebrows equal to the distance from the eyebrow to the / \ / actual defect. The flap is then cut superiorly in two vertical incisions and then undermined in the subgaleal plane below the frontalis muscle. This ensures that the supratrochlear artery is included in the pedicle. The portion of the flap that will actually be used to cover the defect may be debulked of fat to approximate the thickness of the nasal defect. Then the flap is rotated on its pedicle at the level of the eyebrow. The distal aspect is then sewn in at the tip, and the defect on the forehead is closed primarily. The pedicle is cut and discarded at approximately 3 weeks. The rest of the flap is then sewn in at the tip and in the forehead area (Fig. 25).13This flap tends to remain thick for months. If this does not resolve with time, the tip can be debulked in another procedure. \ 'I A Figure 24. Rintuala flap. A, Defect and flap design. 6,Flap movement. C C,Flap sutured into place. NASAL ANATOMY AND RECONSTRUCTION A B C 107 D Figure 25. Midline forehead flap. A, Nasal tip defect and proposed flap. The length from the defect on the nasal tip to the eyebrow is equal to the length of the flap on the forehead. a-b equals b-c, 8 , Flap movement. C,Flap sutured into place on the nasal tip with pedicle in place. The forehead defect is reconstructed primarily. 0,The pedicle is cut and discarded and then the flap is sutured into place at the tip and on the forehead. SUMMARY Reconstruction of the nose provides many challenges owing to its differing subunits and varied surfaces. In this article, the nasal anatomy, anesthesia, and some of the reconstructive options available to the dermatologic surgeon are reviewed. These reconstructive options are based on the subunit and depth of the defect. This subunit approach may provide a framework of decision making and options that will help the dermatologic surgeon in reconstruction of defects on this unique anatomic structure. References 1. Becker FF: Local flaps in facial plastic surgery. J Dermatol Surg Oncol 14635, 1988 2. Becker FF, Hillstrom RP: Reconstruction of the nose and midface. In Papel ID, Nachlas NE (eds): Facial Plastic and Reconstructive Surgery. St. Louis, MosbyYear Book Inc, 1992, p 407 3. Booth SA, Zalla MJ, Roenigk RK, et al: The nasolabial fold donor site for full thickness skin grafts of nasal tip defects. J Dermatol Surg Oncol 19:533, 1993 4. Burget GC, Menick FJ: The subunit principal in nasal reconstruction. Plast Reconstr Surg 76:239, 1985 5. Burget GC: Aesthetic restoration of the nose. Clin Plast Surg 12:463, 1985 6 . Dingman RO, Natvig P: Surgical anatomy in aesthetic and corrective rhinoplasty. Clin Plast Surg 4111, 1977 7. Dzubow LM. Flap dynamics. J Dermatol Surg Oncol 17116,1991 8. Elliot RA Jr: Rotation flaps of the nose. Plast Reconstr Surg 44:147,1969 9. Emery BE, Stucker FJ: The use of grafts in nasal reconstruction. Facial Plast Surg 10:358, 1994 10. Field LM: Nasal alar rim reconstruction utilizing the crus of the helix with several alternatives for donor site closure. J Dermatol Surg Oncol 12253, 1986 11. Field LM: The glabellar transposition "banner" flap. J Dermatol Surg Oncol 14376, 1988 12. Hollier HJ, Stucker FJ: Local flaps for nasal reconstruction. Facial Plastic Surgery 10:337, 1994 13. Jackson I T Nose reconstruction. In Local Flaps in Head and Neck Reconstruction. St. Louis, CV Mosby, 1985, p 87 14. Johnson TM, Ratner D, Nelson B R Soft tissue reconstruction with skin grafting. J Am Acad Dermatol 27151, 1992 15. Kurato S, Hashimoto H, Terashi H, et al: Frontonasal flap for reconstruction of complete alar defects. J Dermatol Surg Oncol 22850, 1996 16. Maves MD, Yessenow RS The use of composite auricular grafts in nasal reconstruction. J Dermatol Surg Oncol 14:994, 1988 17. Meirson D, Goldberg LH. The influence of age and patient positioning on skin tension lines. J Dermatol Surg Oncol 19:39, 1993 18. Redman RD, Olshansky K: Anatomic alar reconstruction with staged nasolabial flap. Ann Plast Surg 20:285, 1988 19. Reiger RA: A local flap for repair of the nasal tip. Plast Reconstr Surg 49:147, 1967 20. Salasche SJ, Grabski WJ: Complications of flaps. J Dermatol Surg Oncol 17:132, 1991 21. Salasche SJ, Bemstein G, Senkarik M Nose. In Surgical Anatomy of the Skin. Norwalk, Appleton and Lange, 1988 22. Salasche SJ: The Nose. In Roenigk RK, Roenigk HH (eds): Dermatologic Surgery: Principles and Practice. New York, Marcel Dekker, 1989 23. Symonds FC, Crikelair GF: Auricular composite 108 MEIRSON grafts in nasal reconstruction: A report of 36 cases. Plast Reconstr Surg 37433, 1966 24. Tromovitch TA, Stegman SJ, Glogau RG: Nasal defects. In Flaps and Grafts in Dermatologic Surgery. Chicago, Year Book, 1989 25. Woodburne RT: Essentials of Human Anatomy. New York, Oxford University Press, 1978 26. Zitelli JA: The bilobed flap for nasal reconstruction. Arch Dermatol 125:957, 1989 27. Zitelli JA: Reconstruction of the nose with local flaps. J Dermatol Surg Oncol 17184, 1991 28. Zitelli JA: Wound healing be secondary intention: A cosmetic appraisal. J Am Acad Dermatol 9:407, 1983 Address reprint requests to Dan H. Meirson, MD 1 West Sample Road Suite 201 Pompano Beach, FL 33064