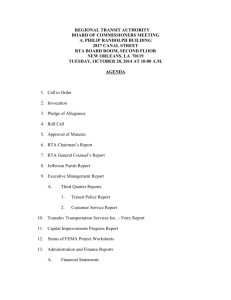
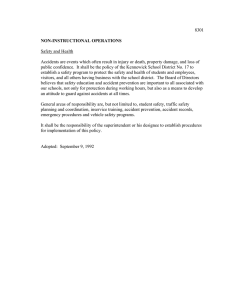
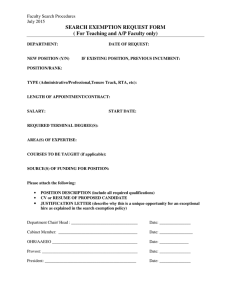
Road Traffic Accidents in Banke District of Nepal Pahadi T.N. Tribhuvan University Bageswory Multiple Public Campus, Kohalpur, Banke, Nepal ABSTRACT Background: Road Traffic Accident is one among the top five causes of morbidity and mortality in South-East Asian countries. In Nepal as per estimates of morbidity and mortality for 1998-1999, injury contributed 9% to total mortality and was the third leading cause, with road accidents occupying the eighth position in the overall ranking. Its socioeconomic repercussions are a matter of great concern. Efficient addressing of the issue requires quality information on its distribution and different causative factors. Methods: The descriptive research design was applied in two hospitals and in one traffic police office for the study of RTA victims recorded from May 2010 to April 2011. Document analysis forms were applied to collect recorded data and semi-structured interview schedules were applied to the key informant hospital personnel and traffic polices. All the recorded 228 victims of RTA were analyzed on percentage basis. Results: It was observed that 59.6 percent of victims were in the age group of 20 to 49 years. The male/female ratio observed in this study was 3.65:1. Employees constituted the largest group (28.95%) involved in RTAs, followed by students (24.12%). Motorcycle accidents were recorded as the highest percentage (38.88). The passengers constituted 42.1 percent of the main road users involved in RTA, followed by driver (25.88%). The highest percentage (14.1%) of RTA victims was recorded in the month of June followed by September (13.0%) and October (13.0%). The highest number of reported accident cases occurred on Fridays (29.3%) and Sundays (21.7%) respectively. High speed (44.6%) was the major cause of accident followed by careless and drunken driving (34.8%). Majority of the victims (58%) had got minor treatment. There was no proper rescue mechanism and victims’ management provision in the district. Conclusion: Most of the factors responsible for RTA and its fatal consequences are preventable. A comprehensive multipronged approach can mitigate most of them. Safer people or safer road users, safer roads, safer vehicles and safety management are the sectors to be addressed to save lives and injuries by reducing road accidents. Keywords: Socio-demographic factors, vulnerable, epidemiological, road and traffic accidents, rescue, Banke district INTRODUCTION The problem of deaths and injury as a result of road accidents is now acknowledged to be a global phenomenon with authorities in virtually all countries of the world concerned about the growth in the number of people killed and seriously injured on their roads. Highly motorised countries with 60 per cent of global vehicles have only 14 percent of global deaths. Conversely Asia/Pacific with only 16 per cent of vehicles has about 44 percent of global deaths. Road fatalities are expected to continue to increase with a fatality toll estimated between 900 thousand and 1.1 million by the year 2010 and between 1.1 and 1.3 million by 2020 (Jacobs & Thomas, 2000). Road accident costs may be US$65 billion in developing and transitional countries, and US$453 billion in highly motorised countries, making a crude estimated total of US$518 billion worldwide (ibid.). Crude estimates suggest that the annual cost of road crashes is about 1% of the Gross National Product (GNP) in developing countries, 1.5 in transitional countries and 2% in highly motorized countries (ibid.). In fact, Road Traffic Accident (RTA) is the number one cause (80 to 90%) for all injuries (Department of Health Services, 2001 & World Health Organization, 2002). In Nepal as per estimates of morbidity and mortality for 1998-1999, injury contributed 9% to total mortality and was the third leading cause, with road accidents occupying the eighth position in the overall ranking. Fifty eight per cent of injuries were in the 15- 44 years age group with a male to female ratio of 3:1 (Jha & Agrawal, 2004). Most commonly affected road users are pedestrians, passengers and cyclists as opposed to drivers who are involved in most of the deaths and disabilities. This ever expanding epidemic targeting the young and productive generations is likely to take a heavy burden on the quality of life and socioeconomic growth of the region (Department of Health Services, 2001). The reasons for the high burden of road traffic injuries in developing countries are: growth in the numbers of motor vehicles; higher number of people killed or injured per crash in lowincome countries; poor enforcement of traffic safety regulations; inadequacy of health infrastructure, and poor access to health care (Nantulya & Reich, 2002). At present more than 1015,271 motorized vehicles are registered in the country with highest share of two wheelers (69%). The growth rate for motorized vehicles is ranging from 9 to 17 percent with an average of 13 percent per year in which two wheelers is highest with about 16 percent (Sitaula,2010). The percentage of road accidents is highest in Urban areas (48%) followed by highways (29%) and rural areas (23%) (Sitaula, 2010). Total fatality rate in road accidents is estimated to be 49.42 percent per 10,000 motorized vehicles (Excluding two and three wheelers) (Sitaula,2010). The highest percentage of vulnerable vehicles is to be for motorcycles (38%) and followed by29 percent for light vehicles (car, jeep, van) (Shrestha, 2006). In recent years shares of causality accidents for motorcycles has been found to increase to 50 percent (ibid.). Considering total estimated 1,986 fatality in a year, 993 deaths are in motorcycle accidents, i.e., 33 deaths per 10,000 motorcycles (ibid.). The top ten highest accident clusters are observed in Kathmandu followed by Chitwan, Dhading, Lalitpur, Jhapa, Nawalparasi, Banke, Kailali, Dang, and Rupendehi district (ibid.). Pedestrians are the largest group of victims in road accidents. Young people of age group from 15 to 40 years are high percentage (44%) in road accident causalities (ibid.). In city and urban areas, accidents of two wheelers account high. Trucks and buses have high accident rates on rural roads. Road accident cost calculation for a single year alone showed at least NRs. 764 million (about 9 million £) which is a significant loss to the nation's resources (0.4% of GDP) (ibid.). Loss in road accidents can be reduced and large amount of nation’s loss could be saved by investing an effective road safety measures. Effective research on road safety issues is an essential pre-requisite to better understanding of the problem and provides the framework against which effective policies and counter measures should be developed (Asian Development Bank, 1997). Studies on RTA are far and few in Nepal. Surprisingly, Banke being the transient point for transportation in Mid-western region has no epidemiological study on RTA. The geographical complexity of the region appears to make it a place of special interest. This study, the first of its kind in Banke, was planned to assess the epidemiological distribution of RTA. METHODOLOGY This descriptive epidemiological study was based on the road traffic accidents recorded in Bheri Zonal Hospital Nepalgunj, Nepalgunj Medical College Teaching Hospital Kohalpur and Regional Traffic Police Office Kohalpur of Banke district. All the 228 Road Traffic accidents and its victims during the period: May 2010 to April 2011 were analysed. The cases were cross-checked to avoid duplication. The victims/relatives of the RTA cases were interviewed to obtain information about the circumstances leading to the accident. Five hospital staffs and Five Traffic Polices were selected purposively as key informants for the study purpose. Different sets of pretested document analysis forms were developed to collect the data from hospitals and traffic police record. The medico-legal records and case sheets of the victims were also referred for collecting necessary data. Semi-structured interview schedules were also constructed to collect data from key informant hospital staffs and traffic polices. Ethical consideration during data collection and analysis was strictly followed. Data collection tools were administered after obtaining the informed consent from the concerned institutions and respondents. All the recorded 228 victims of RTA were analyzed on percentage basis. RESULTS Socio-demographic factors and RTA A total of 228 RTA victims were found to be recorded at both hospitals and District traffic police office during the period: May 2010 to April 2011. There were 179 (76.1%) male and 49 (23.9%) female casualties (Table 1). Table 1. Age and sex distribution of Road Traffic Accident (RTA) victims Age Group 0-9 10-19 20-29 30-39 40-49 50-59 60-69 70 and above Total Males Females Total No. 4 15 16 45 40 30 20 9 % 2.23 8.4 8.9 25.13 22.35 16.76 11.2 5.03 No. 2 5 14 15 6 3 2 2 % 4.1 10.20 28.6 30.6 12.24 6.12 4.1 4.1 No. 6 20 30 60 46 33 22 11 % 2.6 8.7 13.1 26.3 20.2 14.5 9.6 5.0 179 100.0 49 100 228 100 The highest number of victims (26.3%) were from 30-39 years of age followed by 46(20.2%) in the age group 40-49 years. About 70 percent of victims were under 50 years of age. Table 2 describes the educational status and occupation of the RTA victims. Table 2. Educational status and occupations of RTA victims Education Illiterate Primary School High School Intermediate Graduate and above Total Frequency Occupation Frequency No. 75 50 % 32.70 21.94 Employee Student No. 66 55 % 28.95 24.12 46 34 23 20.17 14.91 10.1 Businessman Agriculturist Housewife 50 34 23 21.93 14.91 10.09 228 100.0 228 100.0 About one third percentages (32.7%) of victims were illiterate. Victims with a higher education were fewer in proportion. There were 28.95 percent employees involved in RTA. This was followed by students (24.12%) and businessmen (21.93%). Table 4. Different types of vehicles involved in RTA Type of Vehicle Motorcycle Jeep Bus Truck Cycle Tractor Tempo Others Total No. % 42 29 24 14 12 10 4 1 136 30.88 21.32 17.64 10.29 8.8 7.35 2.94 0.73 100.0 The total numbers of vehicles involved were 136. Of these, 42 (30.88%) were Motorcycle, 29(21.32%) were Jeep and 24(17.64%) were Buses. Table 5. Different categories of victims involved in RTA Category of Victims Passengers(Occupants) Drivers Pedestrians Cyclists Total No. % 96 59 52 21 228 42.1 25.88 22.81 9.21 100.0 The major categories of road users involved in these accidents were occupants of different vehicles (42.1%) followed by drivers (25.88%) and pedestrians (22.81%). Among the drivers of different types of vehicles, 33.87 percent were motorcyclists. Vulnerable Time of RTA Time distribution is an important pattern of RTA from an epidemiological point of view. 16,00% 14,00% 12,00% 10,00% 8,00% 6,00% 4,00% 2,00% 0,00% Figure 1. Vulnerable months by the percentage of accidents The highest numbers of RTA cases were reported in Month: June (14.1%) followed by September (13.0%) and October (13.0%). A greater number of accident cases (37%) were registered in three rainy months of June, September and October, and also in winter months (33.5%). 35,00% 30,00% 25,00% 20,00% 15,00% 10,00% 5,00% 0,00% Sunday Monday Tuesday Wednesday Figure 2. Vulnerable days by the percentage of RTA Thursday Friday Saturday The highest numbers of victims were reported on Fridays (29.30%) followed by Sundays (21.7%). 45,00% 40,00% 35,00% 30,00% 25,00% 20,00% 15,00% 10,00% 5,00% 0,00% AM to 12 AM 12 AM to 6 PM Figure 3. 6Vulnerable time by the percentage of RTA6 PM to 12PM 12PM to 6 AM The highest numbers of accidents were reported in between 12 AM to 6 PM (39.2) followed by 6 AM to 12 AM (31.5%). Consequences of RTA About three fourth of the people (76.7%) were reported either severely injured (38.6%) or Table 6. Distribution of victims by the result of RTA Result of RTA Males Death Severe Injury Moderate Injury Mild Injury Total Females Total No. 34 70 % 19.1 39.3 No. 9 18 % 18.0 36.0 No 43 88 % 19.0 38.6 68 38.2 19 38.0 87 38.1 6 3.4 4 8.0 10 4.3 178 100.0 50 100.0 228 100.0 moderately injured (38.1%). Nearly 20.0% of the victims were died in RTA. About equal percentage of males (19.1%) and females (18%) were died due to these accidents. Table 7. Distribution of deaths by age group in RTA Age group No. of deaths % 1 2 19 14 7 43 2.32 4.65 44.19 32.56 16.28 100.0 Children under 5 yrs Children from 5 to 15 yrs Young people(15 to 40 yrs Elder people(40 to 55 yrs) Elder people above 55 yrs Total Death rate was found to be high (44.19%) among the age group 15 to 40 years followed by age group 40 to 55 years (32.56%). Causes of RTA Table 8. Distribution of the RTAs by the causes Causes of RTA High speed Carelessness of drivers including drunken driving Machinery problem Overload Bad weather condition Passenger carelessness Overtake Total No. % 41 32 44.6 34.8 6 5 5 2 1 92 6.5 5.4 5.4 2.2 1.0 100.0 The main cause of RTA was high speed (44.6%) followed by carelessness of the drivers including drunken driving (34.8%). Management of RTA Victims Victims of RTA were found to be poorly managed in the hospitals. Majority of the 12% 15% Minor Treatment Blood Transfusion Operation ICU 15% 58% Figure 4. Distribution of RTA victims by the treatment category victims (58%) had got minor treatment where others had blood transfused (15%), Performed operation (15%) and kept under ICU (12%) respectively. Emergency care facility for RTA Victims There was no separate ward for the treatment of RTA victims in these two hospitals. Medical staffs have to treat the victims in general emergency ward with less available facilities. Rescue by Security Personnel Most of the victims were rescued by their family or friends and some were also rescued by police and admitted to the hospitals for treatment. There was no proper rescue mechanism in the district. DISCUSSION Among 228 RTA cases recorded, the highest percentage (26.3%) of these were cases in the age group of 30to 39 years. It was observed that 59.6 percent of victims were in the age group of 20 to 49 years. This shows that people from the most active and productive age groups are more involved in RTAs. This causes a serious economic loss to the family, society and nation. It was noticed that below and above the age of 20 and 49 years respectively, there is a decrease in accident cases. The reason for this may be that children are taken care of by elders and are less likely to use vehicles. The lower proportion of RTAs in those aged 60 years and above could be due to the generally less mobility of these population groups. The male/female ratio observed in this study was 3.65:1. This may be due to the fact that females lead a less active life and mostly remain indoors. Furthermore, it was observed that more people with lower levels of education were involved in RTAs. However this relationship between education and RTA may not be causal. In this study, employees constituted the largest group (28.95%) involved in RTAs, followed by students (24.12%). The reason for this may be that employees travel in Motorcycles, Jeeps and Buses which are usually loaded in an improper manner and are in high speed in busy roads. Motorcycle accidents were recorded as the highest percentage (38.88) followed by jeep accidents (21.32%) because these are the major means of transportation in this area. In this study the passengers constituted 42.1percent of the main road users involved in RTA, followed by driver (25.88%) and motorcycle drivers (33.8%) among the drivers category. The highest percentage (14.1%) of RTA victims who reported to these hospitals was recorded in the month of June followed by September (13.0%) and October (13.0). A possible reason for this could be the increased number of accidents in these months, due to rains in June and Dashain, Deepawali and Chhath in September and October. In the present study, the highest number of reported accident cases occurred on Fridays (29.3%) and on Sunday (21.7%). In Nepal, Sundays and Fridays are the first and last working days of the week: this could be the possible reason for the large number of accidents on these days. People celebrate Friday as weekend and possibly are in a hurry to go to various places to join their working places on the following Sunday. The number of accidents was the lowest on Saturdays. The possible reason for this could be that Saturdays are a weekly holiday in Nepal. The other reason could be that Nepalese do not like to start their journey on a Saturday because of a religious belief. High speed (44.6%) was the major cause of accident followed by careless and drunken driving (34.8%). Speed reduces the amount of available time needed to avoid a crash, increases the likelihood of crashing and increases the severity of a crash once it occurs. In the present study, 16.9 percent drivers were found to have consumed alcohol 2-3 hours prior to the accident. The probability of having a crash rises dramatically when a driver reaches and exceeds 0.08 percent Blood Alcohol Concentration (BAC) (SmartMotorist.com, 2010). 0.08 percent BAC is a level at which all drivers, even experienced ones, are impaired with respect to critical driving skills (National Highway Traffic Safety Administration, 1997). The impairment of driving ability increases as the blood alcohol level rises. The relative risk of being killed in a single-vehicle crash is 11 times greater at BACs between 0.05 and 0.09 percent than at a BAC of 0.0 percent (no alcohol) (Zador, 1991). Major causes of road accidents in Nepal are found to be driver’s negligence, over speed, overtaking at critical places, road user’s negligence, drink and driving, overloading, poor vehicle condition, poor road condition, neglecting safety practices and stray animals on street and footpath shops. Majority of the victims (58%) had got minor treatment and others (48%) had got blood transfusion, operation and intensive care under ICU in the hospitals. It was found that emergency facilities and rescue mechanisms for the RTA victims were poor in the district. There was no rapid response mechanism to such accidents and people managed to rescue the victim/s themselves. It takes long time and the victim/s admitted in hospital with critical situation leads to high fatality. CONCLUSION Nepal has comprehensive safety plans for tackling traffic problems, but they are underfunded and poorly coordinated. Worldwide experience has shown that tough but fair and targeted enforcement of measures against unsafe behaviours, along with mass behaviour modification and education are crucial to the rapid improvement of road safety. But the more pressing reality is that current allocations for road safety are inadequate and allocations for educational programmes are even more deficient. There is lack of coordination between different ministries, departments and various agencies working in the field of injury including road traffic injury. Therefore, there is a need for the Ministry of Health to take the lead and coordinate the efforts of all agencies working for the prevention and control of road traffic injuries, and also in road safety. Most of the factors responsible for RTA and its fatal consequences are preventable. A comprehensive multipronged approach can mitigate most of them. Safer people or safer road users, safer roads, safer vehicles and safety management are the sectors to be addressed to save lives and injuries by reducing road accidents. REFERENCES 1. Asian Development Bank. (1997). Road Safety Guidelines for the Asia and Pacific Region. Manila: Asian Development Bank. 2. Department of Health Services. (2001). Annual Report. Nepal: Ministry of Health and Population, Department of Health Services. 3. Jacobs, G.D., & Thomas, A.A. (2000). A review of global road accident fatalities. London: Transport Research Laboratory. 4. Jha, N., & Agrawal, C.S. (2004). Epidemiological study of road traffic accident cases: A study from Eastern Nepal. Regional Health Forum, Vol. 8. 5. Nantulya, M.V., Reich, M.R. (2002). The neglected epidemic: Road traffic injuries in developing countries. British Medical Journal, 324:1139- 1141. 6. National Highway Traffic Safety Administration. (1997). Traffic safety facts for 1997. US Department of Transportation, National Highway Traffic Safety Administration. 7. Shrestha, D.M.S. (2006). Road safety experiences in Nepal. Nepal: Ministry of Physical Planning and Work. 8. Sitaula, T.P. (2010). Status of road safety in Nepal. Nepal: Ministry of Physical Planning and Works. 9. SmartMotorist.com. (2010). Motorist News and driving guidelines. Retrived on February 2010, From http://www.smartmotorist.com/traffic-and-safety-guidelineisan-important-cause-of-road-crashes.html. 10. World Health Organization. (2002). Strategic plan for injury prevention and control in South-East Asia. New Delhi: World Health Organization, Regional Office for South-East Asia. 11.Zador, P.L. (1991). Alcohol- related relative risk of fatal drinker injuries in relation to driver age and sex. Journal on Studies on Alcohol, 52: 302-310.