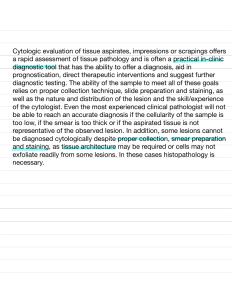
FUNDAMENTALS OF CLINICAL DERMATOLOGY: AND SPECIAL CLINICAL CONSIDERATIONS Fitz 9th ed APPROACH TO THE PATIIENT: PHYSICAL EXAM APPROACH TO THE PATIIENT: PHYSICAL EXAM IDEAL CONDITIONS FOR THE COMPLETE SKIN EXAMINATION: Excellent lighting - bright, natural light - avoids missing out subtle but important details Undress the patient fully and gowned Remove underwear, socks, shoes, makeup, eyeglasses Examining table at a comfortable height - head that reclines - extendable foot rest - gynecologic stirrups Examining room at a comfortable temperature - sink for handwashing Chaperone if a patient and physician are of opposite genders APPROACH TO THE PATIIENT: PHYSICAL EXAM RECOMMENDED TOOLS FOR THE COMPLETE SKIN EXAMINATION : ❖ A magnifying tool such as a loupe, magnifying glass, and/or dermatoscope. ❖ A bright focused light such as a flashlight or penlight. ❖ Glass slides for diascopy and viral direct fluorescent antibody (DFA) testing, fungal scrapings and touch preparations, Tzanck smears, scabies prep. ❖ Alcohol pads to remove scale or surface oil. ❖ Gauze pads or tissues with water for removing makeup APPROACH TO THE PATIIENT: PHYSICAL EXAM RECOMMENDED TOOLS FOR THE COMPLETE SKIN EXAMINATION : ❖ Gloves: when any contagious condition is suspected, when contact with body fluids is possible, when examining mucous membranes and genital areas, and when performing any procedure ❖ A ruler for measuring lesions. ❖ No. 15 and No. 11 scalpel blades for scraping and incising lesions, respectively Diagnostic solutions: potassium hydroxide solution, oil, Tzanck smear, bacterial, viral, and fungal culture media ❖ A camera for photographic documentation ❖ A Wood lamp (365 nm) for highlighting subtle pigmentary changes. APPROACH TO THE PATIIENT: PHYSICAL EXAM TECHNIQUE OF THE DERMATOLOGIC PHYSICAL EXAMINATION: ❖ Observe the patient at a distance for general impressions (eg, asymmetry due to a stroke, cachexia, jaundice) ❖ Examine the patient in a systematic way, usually from head to toe, uncovering one area at a time to preserve patient modesty ❖ Move the patient and the illumination as needed for the best view of each body area ❖ - side lighting best reveals depth and details of skin lesion borders ❖ Palpate lesions to determine whether they are soft, firm, tender, or fluid-filled ❖ - A magnifier worn on the head leaves both hands free for palpation of lesions ❖ - Certain lesions, especially pigmented lesions, are best examined with a dermatoscope to identify characteristic concerning features. APPROACH TO THE PATIIENT: PHYSICAL EXAM TECHNIQUE OF THE DERMATOLOGIC PHYSICAL EXAMINATION: ❖ Mucosal sites should be carefully examined with additional illumination with a penlight or flashlight ❖ During the examination, patients may be reassured by the physician’s reporting of benign lesions as they are encountered ❖ Document the skin findings, including the type of lesions and their locations, either descriptively or on a body map ❖ Photography and triangulation based on anatomic landmarks is particularly important for lesions suspicious for skin malignancy undergoing biopsy, so that the exact location may be found and definitively treated at a later date Fitzpatrick Skin type Fitzpatrick Skin type I II IV V VI III Morphology Introduction to Morphology PRIMARY MORPHOLOGY REACTION PATTERN SECONDARY CHANGE Aids in differential diagnosis Honed further by other lesional characteristics (shape, color,arrangement of lesions in relationship to one another (configuration) and on the body (distribution) Primary Morphology Primary Morphology Patch, Erythema infectiosum FLAT (NONPALPABLE) PRIMARY LESIONS Patch, Nevus of ota Primary Morphology Macule, petechiae FLAT (NONPALPABLE) PRIMARY LESIONS Patch, fixed drug eruption Primary Morphology Papule, lichen nitidus RAISED (PALPABLE) PRIMARY LESIONS Plaque, psoriasis Primary Morphology Nodule, lymphoma cutis RAISED (PALPABLE) PRIMARY LESIONS Plaque, Xanthelasma Primary Morphology FLUID-FILLED PRIMARY LESIONS Vesicles and bullae, linear IgA disease Pustule, pustular psoriasis Secondary Change (Epidermal or Surface Change) Ichthyosiform scale, ichthyosis vulgaris Ostraceous scale, psoriasis Secondary Change (Epidermal or Surface Change) Lichenification, lichen simplex chronicus Eschar overlying stellate purpura, calciphylaxis Secondary Change (Epidermal or Surface Change) Other Lesional characteristics: Color BROWN - most often representative of melanin (within melanocytes or outside of melanocytes) - may be caused by deposition of other pigments, cells, or materials in the dermis (hemosiderin, amyloid, or mucin; certain types of inflammation (granulomatous, histiocytic, plasmacytic, or mixed) Melanin in the epidermis - tan to muddy brown - brown-black (when very concentrated - nevi or melanomas or heavily pigmented seborrheic keratoses) Melanin in the dermis - brown, gray, or blue Other Lesional characteristics: Color RED “erythema” Pale red, pink, purple - may result from inflammation leading to hyperemia (subtle vascular dilation) More saturated red to purple can indicate intense hyperemia or vascular congestion (also called rubor, as seen in erysipelas) Even more saturated red to purple hue can result from the either malformed ectopic blood vessels Extravasated erythrocytes (petechiae or purpura) Other Lesional characteristics: Color Other Lesional characteristics: Color Other Lesional characteristics: Color Purple papules, Kaposi sarcoma Violaceous Gottron papules, dermatomyositis Yellow, necrobiosis lipoidica diabeticorum Apple-jelly sign, sarcoidosis Other Lesional characteristics: Shape and configuration SHAPE – describes the primary lesion CONFIGURATION - refers to shapes made from the arrangement of individual primary lesions in relation to one another DEMARCATION - refers to the edge of an individual lesion and whether it is sharply defined from or blends into the surrounding skin Other Lesional characteristics: Shape and configuration ❖ Annular: Ring-shaped; implies that the edge of the lesion has a color and/or texture ❖ change that is more prominent on the leading edge than the center (granuloma annulare, ❖ tinea corporis, erythema annulare centrifugum) ❖ Round/Nummular/Discoid: Coin-shaped; solid circle or oval; usually with uniform morphology from the edges to the center (nummular eczema, plaque-type psoriasis, discoid lupus) ❖ Arcuate: Arc-shaped; often a result of incomplete formation of an annular lesion (urticaria, ❖ subacute cutaneous lupus erythematosus) Other Lesional characteristics: Shape and configuration ❖ Linear: Resembling a straight line; often implies an external contactant or Koebner phenomenon has occurred in response to scratching; may apply to a single lesion (such as a scabies burrow, poison ivy dermatitis, or bleomycin pigmentation) or to the arrangement of multiple lesions (as seen in lichen nitidus or lichen planus) ❖ Geographic: A shape similar to a land mass; edges are reminiscent of a coastline ❖ Reticular or Retiform: Net-like or lacy in appearance, with somewhat regularly spaced rings or crossing lines with sparing of intervening skin (livedo reticularis, cutis marmorata) ❖ Stellate: Having multiple angulated edges, resembling a star Other Lesional characteristics: Shape and configuration ❖ Serpiginous: Serpentine or snake-like (cutaneous larva migrans) ❖ Targetoid: Target-like, with a center darker than the periphery. ❖ Typical targets (eg, erythema multiforme) have 3 zones: a dark red-purple or dusky center, encircled by a paler pink zone, followed by a rim of darker erythema. ❖ Atypical targets have just 2 zones, a dark or dusky center with a paler pink rim. Note that both have a center darker in comparison to the outer zone; if the center is paler than the outer zone, it should be termed “annular” Other Lesional characteristics: Shape and configuration ❖ Whorled: Like marble cake, with 2 distinct colors interspersed in a wavy pattern; usually seen in mosaic disorders in which cells of differing genotypes are interspersed (as seen in incontinentia pigmenti, hypomelanosis of Ito, linear and whorled nevoid hypermelanosis) ❖ Grouped/Herpetiform: Lesions clustered simplex virus reactivation; arthropod bites) together (Herpes ❖ Scattered: Sparse lesions that are irregularly distributed ❖ Polycyclic: Formed from coalescing circles, rings, or incomplete rings (as seen in urticaria, subacute cutaneous lupus erythematosus) Other Lesional characteristics: Shape and configuration Annular lesion, granuloma annulare Reticular eruption, livedo racemosa Nummular lesion, nummular dermatitis Other Lesional characteristics: Shape and configuration Serpiginous erythema, jellyfish sting Atypical targetoid lesions, Stevens-Johnson syndrome due to medication Polycyclic eruption, pityriasis rosea Other Lesional characteristics: Distribution of multiple lesions Dermatomal/Zosterif orm Blaschkoid - Unilateral and lies in the distribution of a single spinal afferent nerve root - Follows the lines of skin cell migration during embryogenesis - longitudinally oriented on the limbs - circumferential on the trunk Herpes zoster Incontinentia pigmenti, inflammatory linear verrucous epidermal nevus Lymphangitic and Sporotrichoid Sun Exposed/Photodistri buted Sun Protected Lying along the distribution of a lymph vessel implies an infectious agent that is spreading centrally from an acral site - Occurs in areas usually not covered by clothing (face, dorsal hands, and a triangular area corresponding to the opening of a Vneck shirt on the upper chest - Occurs in areas usually covered by one or more layers of clothing - Usually a dermatosis that is improved by sun exposure Photodermatitis, subacute cutaneous lupus erythematosus, polymorphous light eruption, squamous cell carcinoma parapsoriasis, mycosis fungoides “sporotrichoid” - when individual papules or nodules lie along the distribution of a lymphatic network Other Lesional characteristics: Distribution of multiple lesions Acral - Occurring in distal locations, such as on the hands, feet, wrists, ankles, ears, or penis Truncal - Occurring on the trunk or central body Extensor Occurring over the dorsal extremities, overlying the extensor muscles, knees, or elbows (psoriasis is a classic example Psoriasis Flexor Intertriginous - Overlying the flexor muscles of the extremities, the antecubital and popliteal fossae - Occurring in the skin folds, where 2 skin surfaces are in contact (axillae, inguinal folds, inner thighs, inframammary skin, and under an abdominal pannus Childhood atopic dermatitis Often related to moisture and heat generated in these areas Other Lesional characteristics: Distribution of multiple lesions Seborrheic - Favoring the hair-bearing locations of the skin (scalp, eyebrows, beard, central chest, axillae, genitals) - Also often favors the nasolabial and postauricular creases Follicular - Papules centered around hair follicles Localized Confined to a single body location Generalized - Widespread Exanthem (rash) - generalized eruption consisting of inflammatory (red) lesions Bilateral Symmetric Universal - Occurring with mirror- image symmetry on both sides of the body - Involving the entire cutaneous surface Erythroderma, alopecia universalis Other Lesional characteristics: Distribution of multiple lesions END. THANK YOU!