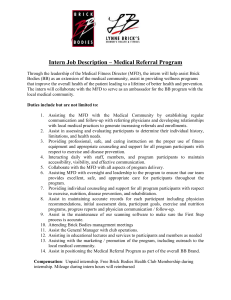
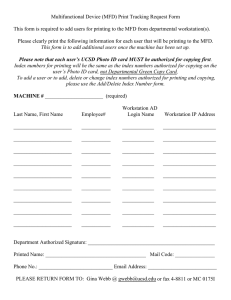
ORIGINAL ARTICLE Perinatal outcome of placental massive perivillous fibrin deposition: a case–control study Louise Devisme1* , Claire Chauvière2, Hélène Franquet-Ansart1, Anastasia Chudzinski2, Morgane Stichelbout1,3, Véronique Houfflin-Debarge2,4 and Damien Subtil2,4 1 Department of Pathology, Lille University Hospital CHRU, Lille Cedex, France Jeanne de Flandre Hospital, Lille University Hospital CHRU, Lille Cedex, France 3 North of France University, Lille, France 4 EA 4489, Lille North of France University, Lille, France *Correspondence to: Louise Devisme. E-mail: louise.devisme@chru-lille.fr 2 ABSTRACT Objective The objectives of the study are to describe the obstetric outcomes associated with massive perivillous fibrin deposition (MFD) compared with a control series and to determine if outcome differs according to the extent of fibrin deposition. Method Retrospective case–control study based on placentas analyzed over a consecutive 12-year period. MFD was considered severe if it extended over more than 50% of the placenta and moderate between 25% and 50%. Results During the study period, MFD was observed on 71 placentas, 39 severe and 32 moderate. Compared with the 142 control women, the 39 women with severe MFD more often had histories of autoimmune disease and intrauterine fetal death. The case women with MFD were associated with elevated levels of maternal alpha-fetoprotein and with a high risk of severe growth restriction and/or intrauterine death. Compared with the infants with moderate MFD, those with severe MFD had also more abnormal umbilical artery Doppler velocimetry findings and more often intrauterine deaths and lower birthweights. Conclusion Regardless of their extent, MFD that covered at least 25% of the placenta was almost always accompanied by severe growth restriction and by a high risk of intrauterine fetal death. Moreover, severe MFD tend to be associated with autoimmune diseases of the mothers, and pregnancies show more often a pathologic Doppler of the umbilical arteries and more often intrauterine fetal death that the moderate form. © 2017 John Wiley & Sons, Ltd. Funding sources: None Conflicts of interest: None declared INTRODUCTION Massive perivillous fibrin deposition (MFD) was first described in the 1960s.1 It is defined by the existence of massive deposits of fibrin extending over at least 25% of the placental volume, whether they are observed to be central, transmural, or basal (along the maternal floor).2 Even though its presence is associated with an increased risk of growth restriction and intrauterine fetal death (IUFD),2–6 this rare lesion remains relatively unstudied, and its cause unknown. Thus, the frequency of growth restriction and the stillbirth rate, associated with this placental lesion, are variable from one study to another. The risk of recurrence is high in the first-trimester abortion, but it seems to be lower when MFD is observed in second-trimester or third-trimester placentas, at around 14%.2–7 The absence of studies comparing these cases with a control population has prevented the formal establishment of a relation between these lesions and the clinical manifestations Prenatal Diagnosis 2017, 37, 323–328 observed. To improve knowledge of the clinical consequences associated with MFD and to determine if outcome differs according to the extent of fibrin deposition, we conducted a retrospective comparative clinicopathologic study. METHODS This single-center continuous retrospective case–control study covers the period from 1 January 2000 to 30 June 2013, in our level 3 university hospital maternity unit. Cases and controls come from a database of all the placental examinations performed during this period in the department of pathology at the request of the maternity department. Records of single pregnancies at a gestational age of 22 weeks or more were eligible for the study. The MFD diagnosis was based on the following criteria: existence of massive fibrin deposits encasing villi on microscopic examination of the placenta, regardless of the potentially associated lesions (Figures 1 and 2). In the case © 2017 John Wiley & Sons, Ltd. 10970223, 2017, 4, Downloaded from https://obgyn.onlinelibrary.wiley.com/doi/10.1002/pd.5013 by University Of Chicago - Librar, Wiley Online Library on [17/11/2022]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License DOI: 10.1002/pd.5013 Figure 1 Macroscopic sections of two placentas demonstrating massive grey-white diffuse deposition of fibrin occupying almost all the parenchyma (a), compared with red and homogeneous sections of a normal placenta (b) Figure 2 Low-power micrograph of two placentas showing massive perivillous fibrin eosinophilic fibrin surrounding strangled villi (a), while villi are clearly visible in the free intervillous space of the normal placenta (b) of recurrence in the same patient, only the index case was retained. Two controls were included for each case: the patients who gave birth immediately before and after the case patient, regardless of whether a placental examination was performed. These controls were not matched with gestational or maternal age, neither with race or ethnicity. All placentas were examined after fixation in formalin. Systematic samples were taken from healthy areas and embedded in three paraffin blocks (the cord and membranes, central placenta and peripheral placenta). Samples were also taken of any macroscopic lesions. The blocks were cut to a 3-μm thickness and stained with hematoxylin-eosin-safran. All slides were reread by a single operator (L. D.). This pathologist was aware only of the Apgar score and birth weight. We set up two groups according to the magnitude of fibrin deposition. The first type, considered severe, was defined by fibrin deposition occupying at least 50% of the villi and intervillous spaces.2 The second group comprised the placentas where fibrin deposition occupied at 25% of the villi and intervillous space but did not reach 50%. These deposits were called moderate.2 Prenatal Diagnosis 2017, 37, 323–328 Maternal and neonatal data were extracted and collected from the medical files by a single investigator (C. C.). Data collection was declared to the French Commission Informatique et Liberté (DEC 16–67). Ethical approval was not required for this retrospective study. We studied the following patient characteristics: age, ethnicity, BMI, smoking status during pregnancy, principal medical and obstetric history. When available, these laboratory results were also noted: alpha-fetoprotein and β-HCG in serum screening for trisomy 21 (n < 2.5 MoM), alkaline phosphatases (N < 2.5 N), transaminases (N < 3 N). The clinical data collected during pregnancy concerned prenatal hospitalization, any preeclampsia, defined according to the ISSHP criteria8 and the uterine and umbilical artery Doppler spectra. Data for pregnancy outcome included gestational age, mode of labor onset, and mode of delivery. Data about the newborn included: birthweight, umbilical artery pH, and the occurrence of either neonatal intensive unit care transfer or death before discharge. Fetal growth restriction was defined according to the French curves derived from 2003 National Perinatal Survey.9,10 The birthweights © 2017 John Wiley & Sons, Ltd. 10970223, 2017, 4, Downloaded from https://obgyn.onlinelibrary.wiley.com/doi/10.1002/pd.5013 by University Of Chicago - Librar, Wiley Online Library on [17/11/2022]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License L. Devisme et al. 324 325 observed were related to the median for gestational age, as birthweight ratios.11 The analysis successively compared each of the MFD groups (severe and moderate) with the control group and then compared the two MFD groups with each other. Epidata 3.1 software (EpiData Association, Odense, Denmark) was used to perform the analysis. Comparisons between the qualitative data used the Chi-2 test or Fisher’s exact test, when the number of individuals was low. Comparisons between the quantitative variables used Wilcoxon’s nonparametric test. All the tests were bilateral, and the significance level was set at P < 0.05. The percentages are reported in parentheses, and means are reported with the standard deviation of the distribution. RESULTS During the study period, 64 619 births took place in our hospital, and 6971 placentas were analyzed (10.8%). Among them, 79 placentas had lesions determined to be MFD (1.1% of placental examinations, 0.1% of deliveries). As required by the study protocol, eight placentas were excluded for the following reasons: twin pregnancies (n = 2), gestational age below 22 weeks (n = 1), recurrence of MFD (n = 5). Finally, the study covered 71 placentas, 39 with severe MFD (>50%) and 32 moderate (25% to < 50%). In the group of 142 control patients, three patients were excluded because of twin pregnancies and were replaced. Table 1 summarizes the characteristics of the case and control patients. Compared with the control women, the case patients with severe MFD were more often of African or West Indian origin (15.4% vs 2.1%, P < 0.001)), or had a history of IUFD (7.7% vs 0.0%, P = 0.009) or an autoimmune disease (12.8% vs 2.1, P = 0.012). They were comparable to the control patients for their other characteristics and history. The women with moderate MFD were comparable to the control patients except that more of the former smoked (41.9% vs 15.5%, P = 0.002). Finally, compared with the women with moderate MFD, the women with severe MFD were more often black (African or West Indian, 15.4% vs 3.1%, P = 0.04) and smoked less often (22.2% vs 41.9%, P = 0.05). Pregnancy outcomes are described in Table 2. Severe MFD was associated with an elevated level of alpha-fetoprotein (>2.5 MoM) in one third of the cases (31.3% vs 0.0%, P < 0.001), without any significant elevation of β-HCG, alkaline phosphatases or transaminases. Clinically, more than half the women with severe MFD were hospitalized before labor (56.4% vs 14.1%, P < 0.001), and almost one in five had preeclampsia (18.0% vs 0.7%, P < 0.001). More than half the fetuses with severe MFD also had abnormal umbilical Doppler spectra (60.0% vs 1.4%, P < 0.001), and nearly a quarter of them died in utero (23.1 vs 0.0, P < 0.001), at a mean gestational age of 31 weeks (range: 24–41 weeks). Preterm delivery was very frequent in this severe MFD group, reaching 62.1% of pregnancies (vs 6.4% in the control group, P < 0.001). Almost one third of the women in this group gave birth very preterm (≤32 weeks: 31.0 vs 0.7%, P < 0.001). Induced delivery was more common in women with severe MFD, with a cesarean rate of 44.8% (vs 9.2% in controls, P < 0.001). Of the liveborn infants in the severe MFD group, 93.1% were growth-restricted, with birthweights below the third percentile (vs 3.5% of the controls, P < 0.001). More than half the newborns with severe MFD were transferred to the neonatal intensive care unit (55.2% vs 2.1%, P < 0.001) (Table 2). There was one postnatal death: a child in Table 1 Patient characteristics according to their group 1 Severe MFD >50% n = 39 Age (years) 29.6 ± 4.9 2 Moderate MFD 25–50% n = 32 31.4 ± 7.1 3 Controls n = 142 30.1 ± 5.7 1 versus 3 2 versus 3 1 versus 2 0.62 0.27 0.21 <0.001 0.69 0.04 0.16 0.50 0.66 0.47 0.002 0.05 Ethnicity White 23 (59.0) 23 (71.8) 111 (78.2) North Africa 8 (20.5) 8 (25.0) 26 (18.3) Sub-Saharan Africa, West Indies 6 (15.4) 1 (3.1) 3 (2.1) 0 2 (1.4) Other BMI (kg/m2) Smokers 2 (5.1) 25.5 ± 6.1 24.8 ± 7.2 24.0 ± 5.8 8 (22.2) 13 (41.9) 22 (15.5) Nulliparas 20 (51.3) 13 (40.6) 59 (41.5) 0.28 >0.99 0.37 History spont. abortion < 12 weeks 11 (28.2) 8 (25.0) 38 (26.8) 0.84 >0.99 0.76 History late miscarriage 12–21 weeks 2 (5.1) 0 (0.0) 1 (0.7) 0.12 >0.99 0.50 History IUFD 3 (7.7) 0 (0.0) 0 (0) 0.009 >0.99 0.24 History preeclampsia/HELLP 1 (2.6) 0 (0.0) 2 (1.4) 0.52 >0.99 >0.99 History deep vein thrombosis 1 (2.6) 0 (0.0) 3 (2.1) >0.99 >0.99 >0.99 0 (0.0) 0 (0.0) 4 (2.8) 0.58 >0.99 5 (12.8) 0 (0.0) 3 (2.1) 0.012 >0.99 History known thrombophilia Autoimmune diseasea 0.06 BMI, body mass index; IUFD, intrauterine fetal death. a Including one Antiphospholipid syndrome, one systemic scleroderma, one dermatopolymyositis, one mixed connective tissue disease and one Goujerot–Sjögren syndrome. Prenatal Diagnosis 2017, 37, 323–328 © 2017 John Wiley & Sons, Ltd. 10970223, 2017, 4, Downloaded from https://obgyn.onlinelibrary.wiley.com/doi/10.1002/pd.5013 by University Of Chicago - Librar, Wiley Online Library on [17/11/2022]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License Perinatal outcome of placental massive perivillous fibrin deposition Table 2 Pregnancy outcomes according to their group 1 Severe MFD >50% n = 39 2 Moderate MFD 25–50% n = 32 3 Controls n = 142 Alpha-fetoprotein > 2.5 MoM 5/16 (31.3) β-HCG > 2.5 MoM 0/17 (0.0) Alkaline phosphatases > 2.5 N 6/19 (31.6) 0/10 (0.0) 6/23 (26.1) SGOT and /or TGP > 3 N 1/29 (3.5) 1/17 (5.9) 2/35 (5.7) Prenatal hospitalization Preeclampsia 22 (56.4) 7 (18.0) 2/78 (2.6) >0.99 0.28 0.35 0.74 0.15 0.07 >0.99 13 (40.6) 3 (9.4) 18/30 (60.0) 6/24 (25.0) 9 (23.1) 35.1 ± 4.6 >0.99 1/9 (11.1) Abnormal umbilical Doppler Gestational age at birtha <0.001 <0.001 11/20 (55.0) In utero death 1 versus 2 0/67 (0.0) 15/32 (46.9) 1 (2.6) 2 versus 3 3/12 (25.0) Abnormal uterine Doppler Medically-indicated TOP 1 versus 3 1 (3.1) 2 (6.2) 36.8 ± 2.4 >0.99 >0.99 20 (14.1) <0.001 <0.001 0.19 1 (0.7) <0.001 0.02 0.49 0.15 0.06 0.57 5/21 (23.8) <0.001 <0.001 1 (0.7) 0.39 0.34 >0.99 0 (0.0) <0.001 0.03 0.10 <0.001 <0.001 0.06 1/70 (1.4) 39.1 ± 3.1 0.01 Preterm birth ≤ 32 weeks 9/29 (31.0) 3/29 (10.3) 1/141 (0.7) <0.001 <0.001 0.05 Preterm birth ≤ 37 weeks 18/29 (62.1) 11/29 (37.9) 9/141 (6.4) <0.001 <0.001 0.07 6/29 (20.7) 14/29 (48.3) <0.001 <0.001 0.09 Mode of labor onseta Spontaneous 112/141 (79.4) Induction of labor 10/29 (34.5) 6/29 (20.7) 16/141 (11.3) Cesarean before labor 13/29 (44.8) 9/29 (31.0) 13/141 (9.2) 18/29 (62.1) 18/29 (62.1) 1730 ± 770 2050 ± 690 27/29 (93.1) Cesareana Birthweight (g)a <3d percentile Umbilical artery pH < 7.15 Transferred to NICU Inhospital neonatal death 4/28 (14.3) 16/29 (55.2) 1/29 (3.5) <0.001 <0.001 >0.99 3390 ± 630 <0.001 <0.001 0.07 24/29 (82.8) 5/141 (3.5) <0.001 <0.001 0.42 2/29 (6.9) 7/132 (5.3) 0.10 0.67 0.42 10/29(34.5) 3/141 (2.1) <0.001 <0.001 0/29 (0) 20/141 (14.2) 0/141 (0) >0.99 0.17 0.11 >0.99 MFD, massive perivillous fibrin deposition; NICU, neonatal intensive care unit; TOP, termination of pregnancy; SGOT, aspartate transaminase. a Excluding medical terminations of pregnancy and in utero deaths. the severe MFD group, born at 32 weeks, weighing 810 g at birth, below the first percentile. In the moderate case group, findings were similar for pregnancies and neonates, with lower proportions but always in the same direction and statistically significant. Finally, the comparison between the severe and moderate MFD groups found no statistically significant differences for laboratory, clinical or obstetric findings between the two groups, except that abnormal umbilical Doppler spectra were more frequent in the severe MPD group (60.0% vs 25.0%, P = 0.01). Nonetheless, we also noted a trend toward more IUFDs in the severe compared with the moderate MFD groups (23.1 vs 6.2, P = 0.10) and toward a lower mean birthweight (1730 ± 770 vs 2050 ± 690, P = 0.07). DISCUSSION Our work represents the first case–control study about MFD. It shows that MFD is almost always associated with very severe growth restriction, regardless of its extent once it reaches the threshold of 25%. It is also associated with an increased risk of IUFD, which reached 23% for the severe Prenatal Diagnosis 2017, 37, 323–328 MFD cases. Moreover, we showed a significant association between elevated alpha-fetoprotein in the second trimester and MFD. Massive perivillous fibrin deposition was found in 0.7% of the placentas examined in our university pathology department, which is consistent with the frequency of 0.5% reported by others.2–4 Related to the number of deliveries, this frequency was estimated at 0.07% in our study, double the estimate of 0.03% by Bane et al.6 These variations may be associated with the women’s ethnic origin and with the indications for placental pathology examinations, which vary between hospitals. In any article, these lesions are rare. In our series, the increased risk of IUFD in the case group was in accordance with the stillbirth rate estimated at 17% to 50% in the literature.3,4,12 The frequency of severe IUGR reached 93%, which is much higher than for other placental diseases. In comparison, the frequency of severe growth restriction (below the third percentile) at our hospital is 30% among the placentas of women with preeclampsia13 and 61% among the placentas with chronic histiocytic intervillositis.14 Accordingly, severe growth restriction is the essential clinical characteristic of MFD. This strong association has already been © 2017 John Wiley & Sons, Ltd. 10970223, 2017, 4, Downloaded from https://obgyn.onlinelibrary.wiley.com/doi/10.1002/pd.5013 by University Of Chicago - Librar, Wiley Online Library on [17/11/2022]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License L. Devisme et al. 326 stressed, with growth restriction rates ranging from 31% to 100%, depending on the author.2–6,12 Some portion of these variations may be explained by the different curves and cut off points used. The cases of growth restriction observed in our series were mainly vascular placental, because 60% of them had abnormal umbilical artery Doppler spectra, including more than 15% with reverse flow or absent diastole. On the other hand, the uterine Doppler spectra did not differ significantly from those of the control group, a finding that does not support the existence of maternal vascular damage. The preeclampsia rate observed in our study was 18%: seven cases, only two severe. This rate is moderate and close to the 20% found in women with isolated growth restriction and abnormal umbilical Doppler findings or among compromised fetuses between 24 and 36 weeks for whom the advantage of immediate delivery was uncertain.15,16 This observation thus points in the same direction as a impairment in the intraplacental blood flow in the intervillous space and not a primary reduction in the uteroplacental circulation. Several authors have mentioned the association between MFD and some autoimmune diseases, especially the antiphospholipid syndrome.17,18 The association with these diseases was significant in our series, although it concerned only 13% (n = 5) of the women. Because each had a different autoimmune disease, it is impossible to associate MFD onset with any particular one. Massive perivillous fibrin deposition can be definitively diagnosed only by pathology examination, retrospectively. Although some hyperechogenic placental features have been described, potentially associated with oligohydramnios,12 there is no marker or antenatal sign specific for this disease. Elevated maternal serum alpha-fetoprotein equal to or greater than 2.5 MoM was found in almost one third of the cases in our series. These high levels have long been known to be associated with an excess of placental diseases, growth restriction and IUFD,19 probably because of early and severe thrombo-occlusive placental lesions. Although elevated alpha-fetoprotein is not specific, it can be used as an early marker of recurrence.20–22 Nonetheless, no data have been published about the sensitivity of this examination. In our study, a diagnosis of MFD was never mentioned during the 327 prenatal period. In practice, because of the risk of recurrence in following pregnancies, the clinical management is important but difficult and not well established so far. Dosage of second trimester maternal serum alpha-fetoprotein, ultrasound monitoring of fetal growth and ultrasounds targeted to the placenta may be helpful to detecting a recurrence and to provide an appropriated neonatal care. Like all case–control studies, our analysis has several limitations. In view of the absence of any obstetric pathology in most of these control patients, some laboratory data, velocimetric (Doppler) findings and most of the placental examinations were unavailable for this group. Nonetheless, the comparison with a control group is a strong point of our study and makes it possible to demonstrate the highly abnormal nature of these placental lesions once they reach 25% of the placental surface. CONCLUSION In our series, 88% of the neonates had severe growth restriction, and half were born preterm. The rate of intrauterine death was high at 15%, still higher than the 10% risk of IUFD in cases of FGR with abnormal umbilical Doppler or uncertain need for immediately delivery.15 To our knowledge, no other placental pathology is associated with so high a rate of growth restriction and of IUFD. Although rare – less than 1% of the placental examinations in our series – this pathology must be considered in cases of severe apparently vascular growth restriction and normal maternal uterine Doppler, especially if serum alpha-fetoprotein was measured and found high during the second trimester of pregnancy. WHAT’S ALREADY KNOWN ABOUT THE TOPIC? • Massive perivillous fibrin deposition is a rare idiopathic disorder associated with a high risk of intrauterine growth restriction and pregnancy loss. WHAT DOES THIS STUDY ADD? • Our study quantifies the risk of severe growth restriction and intrauterine death regardless of the extent of the lesion. REFERENCES 1. Benirschke K, Driscoll S. Maternal floor infarction. Pathology of the Human Placenta. Springer-Verlag: New York; 1967. 2. Katzman PJ, Genest DR. Maternal floor infarction and massive perivillous fibrin deposition: histological definitions, association with intrauterine fetal growth restriction, and risk of recurrence. Pediatr Dev Pathol 2002;5:159–64. 3. Naeye RL. Maternal floor infarction. Hum Pathol 1985;16:823–828. 4. Andres RL, Kuyper W, Resnik R, et al. The association of maternal floor infarction of the placenta with adverse perinatal outcome. Am J Obstet Gynecol 1990;163:935–8. 5. Fuke Y, Aono T, Imai S, et al. Clinical significance and treatment of massive intervillous fibrin deposition associated with recurrent fetal growth retardation. Gynecol Obstet Invest 1994;38:5–9. 6. Bane AL, Gillan JE. Massive perivillous fibrinoid causing recurrent placental failure. BJOG Int J Obstet Gynaecol 2003;110:292–5. Prenatal Diagnosis 2017, 37, 323–328 7. Lee J, Romero R, Xu Y, et al. Detection of anti-HLA antibodies in maternal blood in the second trimester to identify patients at risk of antibody-mediated maternal anti-fetal rejection and spontaneous preterm delivery. Am J Reprod Immunol N Y N 2013;70:162–75. 8. Brown MA, Lindheimer MD, de Swiet M, et al. The classification and diagnosis of the hypertensive disorders of pregnancy: statement from the International Society for the Study of Hypertension in Pregnancy (ISSHP). Hypertens Pregnancy 2001;20:IX–XIV. 9. Blondel B, Supernant K, Du Mazaubrun C, et al. [Trends in perinatal health in metropolitan France between 1995 and 2003: results from the National Perinatal Surveys]. J Gynecol Obstet Biol Reprod 2006;35:373–87. 10. Gardosi J, Mongelli M, Wilcox M, et al. An adjustable fetal weight standard. Ultrasound Obstet Gynecol 1995;6:168–74. 11. Basso O, Frydenberg M, Olsen SF, et al. Two definitions of ‘small size at birth’ as predictors of motor development at six months. Epidemiol Camb Mass 2005;16:657–663. © 2017 John Wiley & Sons, Ltd. 10970223, 2017, 4, Downloaded from https://obgyn.onlinelibrary.wiley.com/doi/10.1002/pd.5013 by University Of Chicago - Librar, Wiley Online Library on [17/11/2022]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License Perinatal outcome of placental massive perivillous fibrin deposition 12. Mandsager NT, Bendon R, Mostello D, et al. Maternal floor infarction of the placenta: prenatal diagnosis and clinical significance. Obstet Gynecol 1994;83:750–4. 13. Devisme L, Merlot B, Ego A, et al. A case–control study of placental lesions associated with pre-eclampsia. Int J Gynaecol Obstet 2013;120:165–8. 14. Marchaudon V, Devisme L, Petit S, et al. Chronic histiocytic intervillositis of unknown etiology: clinical features in a consecutive series of 69 cases. Placenta 2011;32:140–5. 15. GRIT Study Group. A randomised trial of timed delivery for the compromised preterm fetus: short term outcomes and Bayesian interpretation. BJOG 2003;110:27–32. 16. Thornton JG, Hornbuckle J, Vail A, et al. Infant wellbeing at 2 years of age in the Growth Restriction Intervention Trial (GRIT): multicentred randomised controlled trial. Lancet 2004;364:513–20. 17. Bendon RW, Hommel AB. Maternal floor infarction in autoimmune disease: two cases. Pediatr Pathol Lab Med 1996;16:293–7. Prenatal Diagnosis 2017, 37, 323–328 L. Devisme et al. 18. Sebire NJ, Backos M, Goldin RD, et al. Placental massive perivillous fibrin deposition associated with antiphospholipid antibody syndrome. BJOG 2002;109:570–3(2002). 19. Waller DK, Lustig LS, Cunningham GC, et al. The association between maternal serum alpha-fetoprotein and preterm birth, small for gestational age infants, preeclampsia, and placental complications. Obstet Gynecol 1996;88:816–22. 20. Görbe E, Rigo J, Marton T, et al. [‘Maternal floor infarct’, simultaneous manifestation of intrauterine fetal retardation and high maternal AFP level]. Z Geburtshilfe Neonatol 1999;203:218–20. 21. Al-Sahan N, Grynspan D, von Dadelszen P, et al. Maternal floor infarction: management of an underrecognized pathology. J Obstet Gynaecol Res 2014;40:293–6. 22. Katz VL, Bowes WA, Sierkh AE. Maternal floor infarction of the placenta associated with elevated second trimester serum alpha-fetoprotein. Am J Perinatol 1987;4:225–8. © 2017 John Wiley & Sons, Ltd. 10970223, 2017, 4, Downloaded from https://obgyn.onlinelibrary.wiley.com/doi/10.1002/pd.5013 by University Of Chicago - Librar, Wiley Online Library on [17/11/2022]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License 328