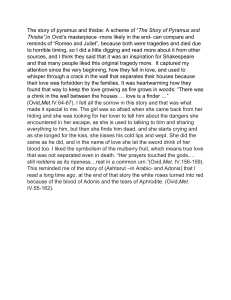
10/22/2020 Part IV: Sustainable Recovery (Print pagebreak 433) CHAPTER 15 Making the Shift From Treating Dysfunction to Treating Sensitivity in Rehabilitation Greg Lehman LEARNING OBJECTIVES After reading this chapter, you should be able to: Understand potential pain science key messages. Consider a different approach to viewing pain from the kinesiopathologic model of dysfunction. “It's partly true, too, but it isn't all true. People always think something's all true. JD SALINGER (Print pagebreak 434) Introduction Treating individuals with pain is difficult. The emergence of pain from an individual is influenced by multiple factors, making pain a multidimensional problem. Pain can be viewed as the person's response to perceived threat and its purpose is to motivate an action. 1 This definition is profound because it disconnects pain from merely being a response to tissue damage. Pain now becomes more about the sensitivity of the individual and how a multitude of factors interrelate to influence pain. When we recognize that numerous factors influence this sensitivity and the production of pain we can also acknowledge how numerous treatment approaches can be helpful. Consistent with viewing pain as something that emerges from the individual and is meant to prompt a response, we can also view many physical dysfunctions in the same light. The assessment process of traditional musculoskeletal rehabilitation (with many approaches detailed in this textbook) attempts to identify physical impairments or presumed movement dysfunctions relative to a proposed ideal in our patients presenting with pain, those with recurrent injuries, and even those individuals who are pain free. The assumption is that impairments or assumed movement dysfunctions in the biomechanical realm either predispose one to pain/injury or perpetuate a painful problem. This is the cornerstone of the kinesiopathologic model of treating pain and injuries. One limitation of the kinesiopathologic model is determining when an impairment is relevant or whether a proposed movement dysfunction is truly dysfunctional or merely is a manifestation of normal or even optimal variation. In order to identify movement dysfunctions, we must know what is ideal or normal. Assumed deviations from the ideal are presumed to be related to pain. It is a difficult task to conduct research in this area, and the research through the years has naturally been mixed. Even when we have research that might relate a specific movement pattern to pain or injury, we are left with clinically important questions: https://oce.ovid.com/book/ovid 1/17 10/22/2020 Part IV: Sustainable Recovery Is this assumed movement dysfunction relevant under all conditions (e.g., high speed, high loads, different sexes, different contexts)? Is the assumed movement dysfunction a cause or consequence of pain? Is the assumed dysfunction merely a product of the normal variability of the motor system? Must the movement dysfunction be changed to influence pain and injury? The purpose of this chapter is to provide an alternative or complementary approach to the kinesiopathologic model. It is recognized that biomechanical movement patterns (simply biomechanics for short) are involved in many pain cases while at the same time recognizing that biomechanics is often completely irrelevant. Alternatively, we can change our view of assumed faulty movement patterns to movements that have merely become sensitized and pain-related rather than inherently dysfunctional. When movements or activities are viewed as sensitized or pain-coupled, 2 we have a number of different interventions to address these sensitivities. Therapeutic neuroscience education (i.e., pain science) and an exercise- and movement-based intervention can be used together with some changes in how the traditional approach is applied. This chapter will have two related sections: The point of pain science: the key messages of therapeutic neuroscience education When biomechanics matters: highlighting the role of biomechanics within the biopsychosocial framework of pain and injury rehabilitation Clinical vignettes will be used to illustrate examples throughout the text. Part I: The Point of Pain Science Therapeutic neuroscience education (i.e., pain science) can be viewed as a separate and distinct component of an overall rehabilitation approach or can be woven into different aspects of a multidimensional treatment approach. Examples of the former being those researched and taught by the Neuro Orthopaedic Institute (Explain Pain, NOI Group), Therapeutic Neuroscience Education researched heavily by Adrian Louw 3 and Jo Nijs. 4 The educational content of pain science education can be delivered separately or in conjunction with other treatment. Moseley and Butler 5 state, “It presents the biological information that justifies a biopsychosocial approach to rehabilitation.” A slightly different approach will use the key messages of pain science education within a multidimensional treatment approach. This approach may see less emphasis on structured education into the (Print pagebreak 435) neurophysiology of pain but will use the concepts of pain science throughout the clinical encounter. Two examples being the Cognitive Functional Therapy approach to rehabilitation 6 and the Progressive Goal Attainment Program. 7 , 8 Both programs recognize that multiple factors contribute to pain; therefore, addressing the biopsychosocial interplay is helpful to influence pain and disability. These management strategies use pain science explanations to reconceptualize both pain and injury to ultimately change how patients view their condition to motivate and support change in their behavior. Pain science education could be used to encourage physical activity, address fears of reinjury, change catastrophizing, and explain the mechanisms behind and the factors influencing a patient's pain. These approaches may differ in how they structure and teach pain science, but they have many similarities that can be seen in the key messages delivered to patients and perhaps in their most basic therapeutic goals. Consistent across these approaches is the change in the meaning of pain to patients. Key messages of pain science will be explored later. The key message will be described and examples of how this influences therapy and function will be discussed. https://oce.ovid.com/book/ovid 2/17 10/22/2020 Part IV: Sustainable Recovery Key Message: Pain Is an Alarm That Is Meant to Motivate an Action Pain is an emergent property of the brain of the person in pain. 9 Hodges and Smeets 10 state, “When pain is acute the nervous system takes action to remove real or anticipated threat to the tissues and this can be achieved by motor output … When pain is chronic the motor system changes and its relevance for ‘protection’ of tissues is less clear.” Moseley and Butler 5 eloquently and simple state, “EP (Explain Pain) emphasizes that any credible evidence of danger to body tissue can increase pain and any credible evidence of safety to body tissue can decrease pain.” This statement captures the multidimensional nature of the persistence of pain and illustrates how multiple interventions can be of benefit. What This Permits Viewing pain as an alarm meant to motivate an action permits multiple lines of discussion that can influence behavior change and change how the patient perceives their condition. An alarm is not an indication of damage but is merely a response to a potential threat. The sensitivity of alarms is also not related to the degree of the problem that an alarm is meant to alert us to. This key message allows the therapist to introduce the idea that sensitivity is influenced by multiple factors in a patient's life and therefore the amount of the alarm (i.e., pain) is also influenced by these factors. Sensitivity can also be changed. Recognizing this bioplasticity and adaptability gives hope but also sets timelines on prognosis for recovery. Common discussion threads to introduce this to your patient are rhetorical questions about fire alarms. What causes a fire alarm to go off? Does the location of the smoke alarm correlate with the location of a fire? Does the alarm mean there is a fire? If a sprinkler goes off in one part of the building, does that mean that there is a fire there? Sprinklers going off at a distant are analogous to changes in muscle activity, muscle strength, weakness, etc., at a distance from the pain. All of these physical changes/impairments can be viewed as similar outputs from the brain/person in as much as pain is an emergent property. This helps reconceptualize impairments as possibly occurring because of the same need for protection or perceived threat as pain itself rather than some inherent flaw in the person. Key Message: Multiple Factors Influence the Sensitivity of the Alarm Related to the first key message is that pain is multifactorial. All aspects of a person's life can influence their sensitivity and pain. For example, catastrophizing, fear of movement, expectations, psychological distress, and stress can influence pain and injury (see Fig. 15.1). https://oce.ovid.com/book/ovid 3/17 10/22/2020 Part IV: Sustainable Recovery Figure 15.1 Pain is multidimensional. It is ultimately created by the person in response to a number of factors. (Print pagebreak 436) What This Permits It is not easy being a musculoskeletal therapist and asking questions that have psychosocial expectations. Many patients do not expect this of therapists and may not understand why the questions are being asked. When pain is explained as something that is influenced by many factors and is more than just tissue damage, then questions like these can begin to be justified. This can build a therapeutic alliance and can also influence recovery. Key Message: Hurt Does Not Equal Harm The belief that pain equals tissue damage is pervasive. The belief that structural and degenerative changes found on imaging may impact the pain severity of many patients. Yet, it is well established that there is an inconsistent and often poor relationship between many imaging findings and pain. Degenerative changes, 11 shoulder labral tears, 12 and disk herniations 13 are consistently seen in asymptomatic populations. Further, even when tissue injury or inflammation appears to be linked with pain, there is no strong relationship between the amount of pain someone feels and the amount of tissue damage. 14 This disconnect can be best illustrated to patients with simple questions about their past experiences with pain. Asking about the pain they felt during a paper cut and how that correlated with damage is useful. Asking queshttps://oce.ovid.com/book/ovid 4/17 10/22/2020 Part IV: Sustainable Recovery tions about the variability in their pain throughout a day or over the course of the week helps illustrate how pain changes faster than we would expect tissue damage to change. A simple example is asking whether they think a fractured bone that is set in a cast for more than a week is painful. The patient will usually reply that they believe it is not painful, yet they will also realize that the bone is still fractured. Highlighting the discrepancy between pain and damage helps facilitate this change in viewpoint. What This Permits This is a start to reconceptualizing pain and changing how the person perceives their condition. This in and of itself can influence the perception of threat or danger and may even influence physical function. 3 Further, it can allow patients to perform activities or exercise that are painful. If pain is viewed as something that is not causing further damage, this allows for the addition of more meaningful activities. This is not to say that pain is ignored. Rather it is accepted and the patient can start to tolerate more activity either with less pain or the same amount. The caveat being that there is an attempt to avoid an exacerbation of symptoms or large flare-ups in pain the next day. 5 Key Message: The Person Adapts to Applied Stress Fundamentally, treatment can be viewed as the application of stressors to the person in pain. Exercise, activities of daily living, resuming work activities, and even cognitive stressors like pain science education can catalyze reactions or adaptation in the person. With acute injuries applying load to an injured tissue or a reactive tendon facilitates healing and repair. In the patient with persistent pain the exposure to feared or painful activities in a slow graded manner can increase the tolerance to those activities. Ideally, the exposure to those activities is preceded by pain science education which prepares the patient to perform activities they might view as threatening. 15 Pain science education mitigates this threat and can change patients' views about the danger associated with resuming meaningful activities or exercise. What This Permits Very simply, recognizing that people have the ability to adapt allows or gives “permission” to start doing the things that they have been missing in their life. Exercise can function as an analgesic 10 and preparing a patient with pain science education can help permit the resumption of exercise. Recognizing that the body adapts can also shift expectations and beliefs about structural influences on pain. It is possible that patients might worry about normal variations in structure (e.g., scoliosis, uneven shoulders, leg length inequality) and feel that these normal variations are driving their pain and must be corrected to be pain free. However, if there is a shift in thinking that the person can adapt, then a change in how a patient views the structural variants can occur. Further key messages can be seen in Figures 15.2 and 15.3. Part II: When Biomechanics Matter Simply, biomechanics might always matter to some extent in the prevention and treatment of pain and injury. It is just a question of what mechanical aspects need to be addressed and how much they contribute to the patient's presentation. For this chapter, biomechanics refers to the BIO aspect of biopsychosocial model of pain and injury. Biomechanics is the study of the forces which act on, and are produced by, the body. Relevant topics to pain and injury are the kinematics or “quality” of movement/technique, forces and loads on the body, the strength or resiliency of tissue, and/or the physical impairments/functional abilities of individuals. (Print pagebreak 437) https://oce.ovid.com/book/ovid 5/17 10/22/2020 Part IV: Sustainable Recovery Figure 15.2 Key message overview part I. The following sections propose potential areas where the biomechanics component of the biopsychosocial model can be viewed as a relevant area to address. This approach recognizes that biomechanics is just one part of multidimensional treatment, but for the sake of brevity, the focus is on the mechanical aspects of rehabilitation. It should also be noted that the presented approach is an alternative and/or overlaps with other mechanical approaches to treating pain and injury. This does not mean that those other approaches are not valuable or effective. It is merely a different route and means of interpreting how common physical findings relate to the patient in pain. Five areas will be presented where biomechanics contribute to pain and injury and where modifying biomechanics may be of benefit in the prevention and treatment of pain and injury. Case vignettes will be used to illustrate the concepts for each category. It is recognized that these categories are fluid and even overlapping. Other categories or means of classifying may also exist. For the purpose of this chapter, mechanics are viewed as relevant in the following areas: Temporary changes to desensitize a painful condition Joint kinematic relevance during high load activities Mechanical changes for the interruption of habits associated with pain Matching individual function with the demands of sports and tasks Respect for the adaptation to imposed stressors Temporary Changes to Desensitize and Painful Condition https://oce.ovid.com/book/ovid 6/17 10/22/2020 Part IV: Sustainable Recovery This is a very straightforward example and borders on common sense. Patients will present with acute injuries or painful episodes that are consistently aggravated (Print pagebreak 438) by a consistent mechanical stimulus. Although it is not possible to parse how much of the pain comes from nociception and how much comes from the processing or one's response to that nociception, it isn't necessary to do this calculation. Simply avoiding aggravating movements and activities for a short period of time is often prudent clinical decision making. Figure 15.3 Key message overview part II. An acute ankle sprain involves nociception that most likely has a chemical and mechanical basis. Minimizing and modifying use for 2 to 3 days after a sprain is appropriate as the neuroimmune responses decrease. The same process applies for an acute lower back strain. The source of the nociception can't be determined quite often, but clinically we often see large amounts of pain that quickly dissipate within 2 to 5 days. Ankle sprain can be viewed as analogous to acute low back pain. Both might involve a neuroimmune response that chemically sensitizes many movements. Respecting that this sensitivity is a normal response and educating the patient that their pain is most likely chemically driven and can be expected to subside quickly is helpful and appropriate. Both of these conditions would warrant short-term relative rest, appropriate loading to catalyze adaptation, and the gradual resumption of normal activities. No fear of movement is created, but the process of sensitivity is explained to reassure that high levels of pain are typically poor indicators of high levels of damage. An Example: Modifying Movements for Temporary Desensitization A 30-year-old female runner presents with a 2-day history of mid to lower portion Achilles pain. The Achilles appears swollen and tender to the touch. There is mild pain with calf raises and pain during running at 15 minutes into each run. Walking is mostly nonpainful. Pain is reported to increase when walking downstairs and running up hills. The patient reports that prior to the pain her (Print pagebreak 439) running mileage increased 20 km (a 40% increase from https://oce.ovid.com/book/ovid 7/17 10/22/2020 Part IV: Sustainable Recovery the previous week) in the past week and she had begun trail running at her tempo pace (a pace much faster than an easy jog). The clinical presentation above is consistent with an Achilles reactive tendinopathy. 16 It is essentially a condition of too much load applied too soon. It has been argued that tendons respond better to tensile loading rather than compressive loading 17 and the Achilles tendon undergoes greater compressive loading in a dorsiflexed position. Consistent with this biomechanical trivia is that the pain appears to increase and has been precipitated by running with increased ankle dorsiflexion. Considering these mechanical variables it is reasonable to avoid/minimize ankle dorsiflexion while the Achilles desensitizes. Modifications should be made to minimize this aggravating activity temporarily. The athlete should be advised to avoid hills, avoid speed work, avoid stretching the calf complex, and avoid foam rolling or other work that actively compresses the tendon. Secondary modifications to influence the strain and compression on the Achilles would be addition of a heel lift to the shoe, a change in shoes to ones with a large heel-toe drop, or even gait modifications to change the stress at the heel. Two examples are to increase stride rate or adopt a more rearfoot strike pattern if the athlete is a forefoot or midfoot strike runner. However, with all changes, these should be done slowly and may not be necessary if running is kept to a volume that avoids flare-ups. At the same time, loading exercises for the tendon can be instituted to further stimulate tendon adaptation and pain relief. 18 Those exercises could be simple isometric calf holds or small range isotonic exercises that avoid dorsiflexion. The caveat here is that dorsiflexion is only avoided for a short period. Initially, 2 weeks can be a sufficient monitoring period as symptoms begin to decrease. Dorsiflexion under load can be reinstituted and using increases in pain the next day as a guide to progression is advised. Lack of flare-ups in pain after 24 hours suggests that the pain is stable and that adding this new positional stressor is acceptable. Dorsiflexion is required for running and many tasks, so exposure to that movement should occur slowly to build tolerance. Joint Kinematic Relevance During High Load Activities Kinematics during functional tasks is often considered important in the prevention and treatment of injuries. We have a preponderance of movement screens to identify proposed dysfunctional kinematics (i.e., quality of movement). It is assumed that these dysfunctions in how someone moves will predispose them to injury. Inherent in this kinesiopathologic model of movement is that there is an ideal way to move and that deviations from those ideals increase injury risk or perpetuate pain. Very crudely, the purpose of movement screens or merely observing individuals move is to identify movement “flaws.” Commonly (not a comprehensive list) proposed movement flaws are: Decreased dorsiflexion Increased pronation Dynamic knee valgus Excessive anterior pelvic tilt Excessive lateral pelvic tilt Loss of the ability to maintain a neutral spine in the sagittal plane Scapular dyskinesis It is assumed that individuals with movement patterns with the above proposed flaws increase their risk of injury. A different viewpoint suggests that these kinematics are not flaws but represent normal variability in huhttps://oce.ovid.com/book/ovid 8/17 10/22/2020 Part IV: Sustainable Recovery man function. And those “flaws” can either be tolerated because of the ability to adapt or they do not need tolerating because they might be optimal for that individual. The research in this area is extensive and extremely mixed and a thorough review is outside the scope of this chapter. What this chapter will explore is the argument that movement quality or specific joint kinematics is more relevant to injury under certain conditions—that is, to discount movement quality or technique under all conditions is just as flawed as arguing that movement quality is important under all conditions. Put succinctly, the argument is that as load increases the number of movement options decreases and that the structural capacity of tissue is challenged. For example, under low loads, it is argued that dynamic knee valgus is poorly linked with an increased injury risk, but under higher loads, the injury risk associated with these movements may increase. Inherent in this argument is the duelling ideas of movement preparation versus movement quality. Movement preparation suggests that all movements can be trained and that an individual's tissues/nervous system can adapt to these movements to become resilient. Although this is potentially attractive, it may have some limitations. Primarily, adaptation is tissue specific and is finite—that is, the loads on some tissues during sport or life might exceed the ability of a tissue to adapt to and hence injury will result. Thus a (Print pagebreak 440) movement quality approach would argue that all positions cannot be prepared for and therefore avoiding those positions under certain conditions is necessary to prevent injury. To illustrate this concept, the next section will explore the proposed movement dysfunction of dynamic knee valgus and knee abduction moment (KAM). Dynamic Knee Valgus and KAM Dynamic knee valgus is composed of hip adduction, hip internal rotation, and knee abduction. The kinetic correlate is an external KAM which sees the ground reaction force creating a KAM during functional tasks like running or jump landing. Dynamic knee valgus is often proposed to be the result of both proximal factors (i.e., weak hip abductors or motor control deficits) and distal kinematics (e.g., increased pronation). Observations during physical tests like a squat, single leg squat, drop jump, running, and cutting occur in an attempt to identify dynamic knee valgus during these tasks and this may lead to clinicians applying various movement corrections/modifications to mitigate the assumed injury risk. This chapter proposes that dynamic knee valgus and the associated external KAM is relevant for injury primarily during heavy load activities under certain conditions and less so during low to moderate load activities of a repetitive nature. A thorough and exhaustive review of the literature is not possible, but contrasting results from various biomechanical studies can help illustrate this proposal. The sensitivity model of rehabilitation also recognizes that a great deal of research will correlate the presence of increased hip adduction during functional tasks with knee pain. However, correlational studies cannot help determine whether the movement pattern is inherently faulty, is a consequence of the pain, or perhaps has just become sensitized and coupled with pain. More on this sensitizing coupling will be explored in the upcoming sections. To avoid this difficulty, prospective research that addresses the role of dynamic knee valgus and knee pain will be discussed. Prospective studies are difficult and there are few which look at this specific question. However, from those that have, we see mixed results related to commonly espoused movement dysfunctions as being predictive or associated with future injuries. https://oce.ovid.com/book/ovid 9/17 10/22/2020 Part IV: Sustainable Recovery Figure 15.4 The adaptability of the person to external loading may provide insight into how individuals response either positively or negatively to repeated loading of assumed faulty positions. The Error of Making Generalized Rules for Injury Mechanisms Quatman et al 19 have documented the biomechanical mechanism of injury to the anterior cruciate ligament (ACL) as consisting of KAM, tibial internal rotation moment, and tibial anterior shear. Video analysis of noncontact ACL injuries lends some support to these movement patterns as being associated with acute ACL tears. 20 Waldén et al 20 reported “we frequently observed knee valgus, but we rarely saw an overt dynamic valgus collapse.” Of note was the low amount of knee flexion (˜20 degrees) associated with observed injuries. We have evidence of specific movement pattern being associated with high load on a specific structure (ACL) which exceeds that structure's failure threshold. However, this is a faulty movement pattern under all conditions and for all knee structures. Knee valgus is an important component of many sports and can also be seen as normal movement pattern in many athletes. Where the pattern may be completely safe is in low load but highly repetitive activities. It is under these other conditions where knee valgus may be tolerated and perhaps advantageous. An example of knee valgus at high level sport would be in the repeated motions of an ice hockey goal tender. Other examples are commonly seen in female distance runners. Knee valgus is an inherently faulty pattern that predisposes to lower limb injury or pain. It is possible that the slow exposure to the knee valgus permits slow adaptation to positions (Fig. 15.4). (Print pagebreak 441) Instead of viewing the pattern as faulty, it could be viewed similar to all stressors placed on the person—we must adapt to them. The stressor is the catalyst for healthy adaptation. Prospectively, there is some evidence that females who demonstrate increased KAM during a drop landing task are at an increased risk for future ACL injuries. 21 Those authors showed that girls with a KAM greater than 25.3 N·m had an injury risk of 6.8% versus 0.4% if below that threshold (see Fig. 15.5). Of note, those with a KAM greater than 15.3 N·m had a patellofemoral pain injury risk of 6.8%, but if below that threshold, they still had an injury risk of 2.9%. This prospective study illustrates the concept of how high load activities might have a relevant mechanical variable that is less relevant in low load activities. For example, other prospective studies looking at patellofemoral pain syndrome (PFPS) will inconsistently link components of dynamic knee valgus with future pain. For example, Noehren et al 22 linked increased hip adduction (˜4 degrees) in a group that went on to develop PFPS. However, other components of knee valgus (hip internal rotation and calcaneal eversion) were not linked with future pain. One issue with Noehren et al 22 was that the injured group had only 12 degrees of hip adduction versus a control group that had 8 degrees of hip adduction. This 8-degree average of the control group and the 12-degree average of the injured group are lower than the majority of control groups' (pain free) average hip adduction seen in systematic reviews. 23 Thus, it is difficult to look at a runner and conclude that they have a degree of hip adduction that predisposes them to injury. One can't suggest that it is 12 degrees (the amount seen in the prospectively injured group) as this is typically less than every https://oce.ovid.com/book/ovid 10/17 10/22/2020 Part IV: Sustainable Recovery control running group. In a 2-year prospective study looking at the relationship between joint kinematics and drop jump landing, Boling et al 24 (Print pagebreak 442) showed that hip adduction and calcaneal eversion were not linked with future pain, but when comparing groups at the extremes, there was a difference in hip internal rotation between those who experienced future PFPS and those who didn't. We have few prospective studies and the ones existing do not provide a strong basis to conclude that hip adduction under low and repetitive loads is an exceedingly strong risk factor for knee pain. Figure 15.5 Increased knee abduction moment (KAM) may better predispose to tissue failure injuries (e.g., anterior cruciate ligament [ACL]) than nontissue failure injuries (e.g., anterior knee pain). This opinion does recognize, aided by correlational data, increased group hip adduction (a component of knee valgus) in groups with patellofemoral pain during either running 23 or functional tasks. 25 The sex of the athlete in pain also appears to influence the significance of the proposed faulty kinematic with pain. 26 Willy et al 27 showed that males with PFPS demonstrate decreased hip adduction but increased knee abduction and KAM. Conversely, hip adduction is inconsistently linked with pain with a number of studies showing no differences between groups. 28 , 29 These inconsistencies may reflect normal variability, the adaptability of the human system, and the natural complexity of the human movement. These inconsistencies suggest that it is very difficult to look at specific human movement patterns and label them as faulty or normal. Rather, it may be more accurate and certainly simpler to describe them as sensitive or not sensitive. With this framework, we recognize that intervening to change a sensitive movement pattern can be sufficient to decrease pain but may not be necessary—that is, kinematic interventions can help but are not necessarily the only way to treat the pain. Nor do those movement patterns need to be changed forever. When we view pain as a multidimensional phenomenon, we can be optimistic about our chances to change pain because there may be a number of options to desensitize the person— kinematic changes being just one. Perhaps, those patterns are changed as a temporary reprieve and then the inhttps://oce.ovid.com/book/ovid 11/17 10/22/2020 Part IV: Sustainable Recovery dividual can slowly resume those patterns, learn to tolerate them, and function pain free. This concept leads to the other category of when biomechanics matters in relation to pain. Mechanical Changes for the Interruption of Habits Associated With Pain The previous category naturally transitions to this category. If a movement pattern is not inherently faulty, how can it be categorized? An alternative approach is to view it merely as sensitized. This viewpoint leads to a greater number of treatment options. Those options might be: Avoid the activities that lead to the sensitive movement. Address all of the multidimensional components in a patient's life that lead to pain and sensitivity. Change the movement pattern during the offending activities. To put it bluntly, we can avoid the pattern or learn to desensitize the pattern to tolerate it. These options are well illustrated in the case studies and in clinical experience. In the running injury literature individuals with patellofemoral pain will undergo a rehabilitation program that involves hip and knee resistance training. Traditionally, the intention was to either change lower extremity kinematics or perhaps change muscle timing patterns. However, we see that exercise programs designed to make these changes often fail 30 , 31 but pain relief occurs nonetheless. 32 However, kinematic changes can be made and those too can be helpful in changing pain during rehabilitation. This is well illustrated in running retraining trials, which attempt to change joint kinematics to influence function. 27 , 33 Where one might view this research as conflicting a more clinically optimistic view is to consider that we have multiple options in helping patients in pain—that is, specific movement corrections are not necessary but can certainly be viewed as helpful. We can see the role of changing movement patterns to alter sensitivity when it comes to treating low back pain. A highly debatable area is the role of spinal flexion in low back pain. It is often argued that spinal flexion should be minimized during lifting or activities of daily living to prevent the degeneration of the spine and the potential for low back pain. It may be easier to come to a consensus when individuals are already in pain. If individuals with low back pain are sensitized to flexion, it may be an appropriate option to avoid it temporarily. Patients who consistently aggravate their pain with flexion-related activities could benefit from training in neutral avoiding the aggravating motion provided the suggestion does not create a fear of the movement or contribute to disability through avoidance. Further, patients involved in sports that require high degrees of repeated flexion and then “sparing” the spine during their training could be helpful. Much like the recommendations from the first category of when biomechanics matters, we may not need to avoid this movement forever. We can teach that avoiding flexion is a temporary measure to allow them to desensitize. And part of treatment is to slowly reintroduce some flexion over time. Thus our clinical decision making can be guided by symptom modification and sensitivity. We do not need to vilify spinal flexion; rather minimizing it initially is an option to (Print pagebreak 443) allow our patients to control their pain and continue the activities they enjoy. It recognizes that adaptation is often finite. Some individuals may be able to desensitize their nervous system via changing their beliefs, addressing catastrophizing, improving self-efficacy, changing fear, and this allows them to tolerate and to habituate to painful flexion but others may not be able to habituate and desensitize. Thus avoiding flexion is reasonable and justifiable. In other words, if spinal flexion is sensitive and attempts to tolerate this spinal flexion prove unsuccessful in influencing low back pain, then avoiding spinal flexion via spinal sparing strategies is an appropriate choice. This is an example of where a movement “flaw” is not an absolute movement “flaw.” Rather it is merely faulty because it is sensitized. It can become desensitized and that movement can occur pain free in the future. Matching Individual Function With the Demands of Sports and Tasks At its simplest, biomechanics matters when loads are highest. We can't make a general recommendation that being stronger will decrease pain or injury risk in every individual. Although strength training itself appears protective for injury, 34 its role may be more relevant under certain conditions. This is best exemplified in https://oce.ovid.com/book/ovid 12/17 10/22/2020 Part IV: Sustainable Recovery sports injuries associated with high loads. For example, sprinting during football/soccer/rugby is associated with high hamstring tears. In these sports elevated levels of strength are considered moderately protective for future injuries. 35 , 36 With respect to joint mobility, a similar trend might be seen. Increased ankle dorsiflexion may be an increased risk for injury in military recruits during basic training, 37 whereas decreased ankle dorsiflexion may be an injury risk for patellar tendinopathy in basketball and volleyball players. 38 , 39 Military training versus basketball/volleyball may have equivalent physiologic stressors but the specific demands on the lower extremity are different. Making blanket statements about optimal joint function is difficult if optimal joint function depends on the needs of the individual determined by the specific activity. Respect for the Adaptation to Imposed Stressors It could be argued that movement patterns are less important than sensitivity. A component of this argument recognizes that the human system is adaptable. Thus, we adapt to the imposed stresses and that injury and pain can be prevented with this slow adaptation process. However, adaptability is finite and is different across tissue types. This may be best seen in the spine. Repeated, heavy flexion loading that is progressive will no doubt increase the strength of the myofascial and connective tissue system. However, components of that system may adapt faster or better than others. We have no warning mechanism to alert us when an adaptability threshold is reached. We make clinical decisions in a very gray area. In the area of sport this respect for adaptability is best illustrated in the work looking at the ratio of chronic to acute workloads. What this research suggests is that acute changes in physical and perceived stressors that are much greater than the applied stress for the past few weeks increase the risk of injury. 40 Summary The causes and perpetuators of pain and injury are multidimensional. It is difficult, if not impossible, to determine the contributing factors. Viewing pain as a manifestation of sensitivity of the entire person allows the clinician to implement multiple therapies in an attempt to address all possible drivers of the patient's sensitivity. Working in the biopsychosocial model of pain and injury does not mean the biomechanics is ignored. Rather, biomechanics can be reconceptualized and considered from a different viewpoint. This chapter has highlighted a number of ways to reconcile the kinesiopathologic model of pain within the biopsychosocial framework besides distilling simple therapeutic neuroscience messages for a patient population. Audit Process Self-check of the chapter's learning objectives Can you provide simple key messages about pain that are relevant to the patient's presentation and story? Are there other simple key messages about pain that might be relevant to the typical patient you might see? Can you integrate key messages about pain with an optimistic view of biomechanical treatment approaches? Can you consider how some of your current mechanical treatment approaches might fall under a specific category of when biomechanics matters? https://oce.ovid.com/book/ovid 13/17 10/22/2020 Part IV: Sustainable Recovery (Print pagebreak 444) References 1. Moseley G, Butler D. The Explain Pain Handbook: Protectometer. Adelaide, Australia: Noigroup Publications; 2015;58. 2. Zusman M. Associative memory for movement-evoked chronic back pain and its extinction with musculoskeletal physiotherapy. Phys Ther Rev. 2008;13(1):57-68. 3. Louw A, Puentedura EJ, Zimney K, Schmidt S. Know Pain, Know Gain? A perspective on pain neuroscience education in physical therapy. J Orthop Sports Phys Ther. 2016;46(3):131-134. doi:10.2519/jospt.2016.0602. 4. Nijs J, Meeus M, Cagnie B, et al. A modern neuroscience approach to chronic spinal pain: combining pain neuroscience education with cognition-targeted motor control training. Phys Ther. 2014;94(5):730-738. doi:10.2522/ptj.20130258. 5. Moseley GL, Butler DS. Fifteen years of explaining pain: the past, present, and future. J Pain. 2015;16(9):807-813. doi:10.1016/j.jpain.2015.05.005. 6. Vibe Fersum K, O'Sullivan P, Skouen JS, Smith A, Kvåle A. Efficacy of classification-based cognitive functional therapy in patients with non-specific chronic low back pain: a randomized controlled trial. Eur J Pain. 2013;17(6):916-928. doi:10.1002/j.1532-2149.2012.00252.x. 7. Raftery MN, Murphy AW, O'Shea E, Newell J, McGuire BE. Effectiveness of a cognitive behavioural therapy-based rehabilitation programme (Progressive Goal Attainment Program) for patients who are workdisabled due to back pain: study protocol for a multicentre randomised controlled trial. Trials. 2013;14:290. doi:10.1186/1745-6215-14-290. 8. Sullivan MJ, Adams H, Rhodenizer T, Stanish WD. A psychosocial risk factor—targeted intervention for the prevention of chronic pain and disability following whiplash injury. Phys Ther. 2006;86(1):8-18. 9. Rio E, Moseley L, Purdam C, et al. The pain of tendinopathy: physiological or pathophysiological? Sports Med. 2014;44(1):9-23. doi:10.1007/s40279-013-0096-z. 10. Hodges PW, Smeets RJ. Interaction between pain, movement, and physical activity: short-term benefits, long-term consequences, and targets for treatment. Clin J Pain. 2015;31(2):97-107. 11. Brinjikji W, Luetmer PH, Comstock B, et al. Systematic literature review of imaging features of spinal degeneration in asymptomatic populations. AJNR Am J Neuroradiol. 2015;36(4):811-816. doi:10.3174/ajnr.A4173. 12. Schwartzberg R, Reuss BL, Burkhart BG, Butterfield M, Wu JY, McLean KW. High prevalence of superior labral tears diagnosed by MRI in middle-aged patients with asymptomatic shoulders. Orthop J Sports Med. 2016;4(1). doi:10.1177/2325967115623212. https://oce.ovid.com/book/ovid 14/17 10/22/2020 Part IV: Sustainable Recovery 13. Jensen OK, Nielsen CV, Sørensen JS, Stengaard-Pedersen K. Back pain was less explained than leg pain: a cross-sectional study using magnetic resonance imaging in low back pain patients with and without radiculopathy. BMC Musculoskelet Disord. 2015;16(374). doi: 10.1186/s12891-015-0827-4. 14. Lluch E, Torres R, Nijs J, Van Oosterwijck J. Evidence for central sensitization in patients with osteoarthritis pain: a systematic literature review. Eur J Pain. 2014;18(10):1367-1375. doi:10.1002/j.15322149.2014.499.x. 15. Nijs J, Torres-Cueco R, van Wilgen CP, et al. Applying modern pain neuroscience in clinical practice: criteria for the classification of central sensitization pain. Pain Physician. 2014;17(5):447-457. 16. Cook JL, Purdam CR. Is tendon pathology a continuum? A pathology model to explain the clinical presentation of load-induced tendinopathy. Br J Sports Med. 2009;43(6):409-416. doi:10.1136/bjsm.2008.051193. 17. Docking S, Samiric T, Scase E, Purdam C, Cook J. Relationship between compressive loading and ECM changes in tendons. Muscles Ligaments Tendons J. 2013;3(1):7-11. doi:10.11138/mltj/2013.3.1.007. 18. Rio E, Kidgell D, Purdam C, et al. Isometric exercise induces analgesia and reduces inhibition in patellar tendinopathy. Br J Sports Med. 2015;49(19):1277-1283. doi:10.1136/bjsports-2014-094386. 19. Quatman CE, Kiapour AM, Demetropoulos CK, et al. Preferential loading of the ACL compared with the MCL during landing: a novel in sim approach yields the multiplanar mechanism of dynamic valgus during ACL injuries. Am J Sports Med. 2014;42(1):177-186. doi:10.1177/0363546513506558. 20. Waldén M, Krosshaug T, Bjørneboe J, Andersen TE, Faul O, Hägglund M. Three distinct mechanisms predominate in non-contact anterior cruciate ligament injuries in male professional football players: a systematic video analysis of 39 cases. Br J Sports Med. 2015;49(22):1452-1460. doi:10.1136/bjsports-2014094573. 21. Myer GD, Ford KR, Di Stasi SL, Foss KD, Micheli LJ, Hewett TE. High knee abduction moments are common risk factors for patellofemoral pain (PFP) and anterior cruciate ligament (ACL) injury in girls: is PFP itself a predictor for subsequent ACL injury? Br J Sports Med. 2015;49(2):118-122. doi:10.1136/bjsports-2013-092536. 22. Noehren B, Hamill J, Davis I. Prospective evidence for a hip etiology in patellofemoral pain. Med Sci Sports Exerc. 2013;45(6):1120-1124. doi:10.1249/MSS.0b013e31828249d2. 23. Neal BS, Barton CJ, Gallie R, O'Halloran P, Morrissey D. Runners with patellofemoral pain have altered biomechanics which targeted interventions can modify: a systematic review and meta-analysis. Gait Posture. 2016;45:69-82. doi:10.1016/j.gaitpost.2015.11.018. 24. Boling MC, Padua DA, Marshall SW, Guskiewicz K, Pyne S, Beutler A. A prospective investigation of biomechanical risk factors for patellofemoral pain syndrome: the joint undertaking to monitor and prevent ACL injury (JUMP-ACL) cohort. Am J Sports Med. 2009;37(11):2108-2116. doi:10.1177/0363546509337934. https://oce.ovid.com/book/ovid 15/17 10/22/2020 Part IV: Sustainable Recovery 25. Nakagawa TH, Moriya ÉT, Maciel CD, Serrão AF. Frontal plane biomechanics in males and females with and without patellofemoral pain. Med Sci Sports Exerc. 2012;44(9):1747-1755. doi:10.1249/MSS.0b013e318256903a. 26. Phinyomark A, Osis S, Hettinga BA, Leigh R, Ferber R. Gender differences in gait kinematics in runners with iliotibial band syndrome. Scand J Med Sci Sports. 2015;25(6):744-753. doi:10.1111/sms.12394. 27. Willy RW, Manal KT, Witvrouw EE, Davis IS. Are mechanics different between male and female runners with patellofemoral pain? Med Sci Sports Exerc. 2012;44(11):2165-2171. doi:10.1249/MSS.0b013e3182629215. (Print pagebreak 445) 28. Foch E, Reinbolt JA, Zhang S, Fitzhugh EC, Milner CE. Associations between iliotibial band injury status and running biomechanics in women. Gait Posture. 2015;41(2):706-710. doi:10.1016/j.gaitpost.2015.01.031. 29. Grau S, Krauss I, Maiwald C, Axmann D, Horstmann T, Best R. Kinematic classification of iliotibial band syndrome in runners. Scand J Med Sci Sports. 2011;21(2):184-189. doi:10.1111/j.1600-0838.2009.01045.x. 30. Snyder KR, Earl JE, O'Connor KM, Ebersole KT. Resistance training is accompanied by increases in hip strength and changes in lower extremity biomechanics during running. Clin Biomech (Bristol, Avon). 2009;24(1):26-34. doi:10.1016/j.clinbiomech.2008.09.009. 31. Willy RW, Davis IS. The effect of a hip-strengthening program on mechanics during running and during a single-leg squat. J Orthop Sports Phys Ther. 2011;41(9):625-632. doi:10.2519/jospt.2011.3470. 32. Esculier JF, Bouyer LJ, Roy JS. The effects of a multimodal rehabilitation program on symptoms and ground-reaction forces in runners with patellofemoral pain syndrome. J Sport Rehabil. 2016;25(1):23-30. doi:10-1123/jsr.2014-0245. 33. Noehren B, Scholz J, Davis I. The effect of real-time gait retraining on hip kinematics, pain and function in subjects with patellofemoral pain syndrome. Br J Sports Med. 2011;45(9):691-696. doi:10.1136/bjsm.2009.069112. 34. Lauersen JB, Bertelsen DM, Andersen LB. The effectiveness of exercise interventions to prevent sports injuries: a systematic review and meta-analysis of randomised controlled trials. Br J Sports Med. 2014;48(11):871-877. doi:10.1136/bjsports-2013-092538. 35. Opar DA, Williams MD, Timmins RG, Hickey J, Duhig SJ, Shield AJ. Eccentric hamstring strength and hamstring injury risk in Australian footballers. Med Sci Sports Exerc. 2015;47(4):857-865. doi:10.1249/MSS.0000000000000465. 36. Timmins RG, Bourne MN, Shield AJ, Williams MD, Lorenzen C, Opar DA. Short biceps femoris fascicles and eccentric knee flexor weakness increase the risk of hamstring injury in elite football (soccer): a prospective cohort study. Br J Sports Med. 2016; 50(24):1524-1535. doi:10.1136/bjsports-2015-095362. 37. Mahieu NN, Witvrouw E, Stevens V, Van Tiggelen D, Roget P. Intrinsic risk factors for the development of Achilles tendon overuse injury: a prospective study. Am J Sports Med. 2006;34(2):226-235. https://oce.ovid.com/book/ovid 16/17 10/22/2020 Part IV: Sustainable Recovery 38. Backman LJ, Danielson P. Low range of ankle dorsiflexion predisposes for patellar tendinopathy in junior elite basketball players: a 1-year prospective study. Am J Sports Med. 2011;39(12):2626-2633. doi:10.1177/0363546511420552. 39. Malliaras P, Cook JL, Kent P. Reduced ankle dorsiflexion range may increase the risk of patellar tendon injury among volleyball players. J Sci Med Sport. 2006;9(4):304-309. 40. Gabbett TJ. The training-injury prevention paradox: should athletes be training smarter and harder? Br J Sports Med. 2016;50(5):273-280. doi:10.1136/bjsports-2015-095788. https://oce.ovid.com/book/ovid 17/17