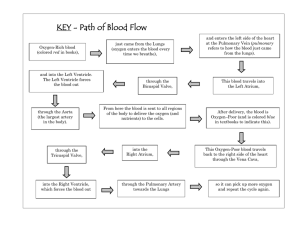
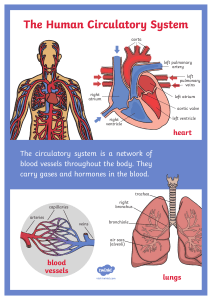
FETAL HEART DEFECTS, CLASSIFICATION, & TYPES *Fetal ductus arteriosus: artery that connects to aorta + pulmonary artery *Heart Shunt: abnormal pattern of blood flow through heart *Left-to-Right Shunt: abnormal pattern of blood flow through heart ; allows the oxygenated (saturated) pulmonary venous blood to return directly to the lungs rather than being pumped to the body; some can go away on its own without treatment *Right-to-Left Shunt: abnormal pattern of blood flow through heart; some blood does NOT get oxygenated; allows the deoxygenated, systemic venous return to bypass the lungs and return to the body without becoming oxygenated; usually require surgery to correct. LEGEND: ASD= Atrial septal defect; CHD= congenital heart disease; HLHS = hypoplastic left heart syndrome; PDA = patent ductus arteriosus; PS = pulmonic stenosis; RVOT = right ventricular outflow tract = TGA, transposition of the great arteries; VSD = ventricular septal defect; BE, = bacterial endocarditis; COA = coarctation of the aorta; LV/LA – left ventricle/left atrium; RV/RA: right ventricle/right atrium; L-to-R = left-to-right shunting; R-to-L = right to left shunting FETAL HEART DEFECTS, CLASSIFICATION, & TYPES DEFECTS RELATED TO AN ↑ IN PULMONARY BLOOD FLOW Characteristics: mixing of blood from the pulmonary + systemic circulations in heart chambers; fully saturated systemic blood mixes w/ desaturated pulmonary blood flow (causes a systemic blood flow that has less O2) Pathophysiology -Abnormal opening between atria - L-to-R shunt (high to low) -blood in L Atrium shunt to R Atrium -↑ flow of oxygenated blood to R side of heart Complications: risk for atrial dysrhythmias, pulmonary vascular obstructive disease, embolism Signs/Symptoms Treatment Asymptomatic (early on) Surgical TX: Surgical patch closure Open repair cardiopulmonary bypass HF (develop after awhile) Systolic/diastolic murmur (w/ fixed split 2nd heart sound) Nonsurgical treatment: Amplatzer Septal Occluder Enlarged RA Most close spontaneously Atrial Septal Defect -Abnormal opening between L & R ventricles -L-to-R shunting occurs -blood in L ventricle shunt to R ventricle -more resistance in systemic than pulmonary -co-occur w/ other defects (pulmonary stenosis, transposition of great vessels, ductus arteriosus, atrial defects, coarct of aorta) (during 1st yr of life) Enlarged RV HF loud holosystolic murmur - ↑ blood volume forced into lungs (↑ resistance) Ventricular Septal Defect Complications: risk for Endocarditis, pulmonary obstructive disease -ductus arteriosus don’t fully close in 1st weeks of life -causes L-to-R shunting -blood continues flow from aorta →pulmonary artery -severity depends on size of ductus & pulmonary resistance Complications: injury to laryngeal nerve/thoracic, left diaphragm paralysis (heard best at L sternal border) Asymotomatic HF Machinery-like murmur R Ventricle hypertrophy Pulmonary Congestion Widened pulse presure Bounding pulses Surgical TX: Pulmonary artery banding Complete Repair Sutures (small defects) Knitted Dacron patch (large defect) Medication TX: Indomethacin (Prostaglandin inhibitor) Surgical TX: Thoracotomy (Division of ductus arteriosus) Non-Surgical TX: Coils to occlude/close ductus FETAL HEART DEFECTS, CLASSIFICATION, & TYPES DEFECTS RELATED TO A ↓ PULMONARY BLOOD FLOW Characteristics: obstruction of pulmonary blood flow + an anatomic defect (ASD or VSD) between the right and left sides of the heart Pathophysiology -includes total of FOUR defects: Ventricular septal defect, pulmonary stenosis, overriding aorta & RV hypertrophy - pressures may be equal in the R & L ventricles - shunt direction depends on difference between pulmonary & systemic resistance -R-to-L shunt occurs if pulmonary resistance is higher Tetralogy of Fallot -L-to-R shunt occurs if systemic resistance is higher -Anoxic spells: occur usually during crying or after feeding. Infant’s O2 needs exceed the blood supply available. Increases risk for emboli, seizures, loss of consciousness or sudden death after an anoxic spell - tricuspid valve fails to develop -no communication between R atrium to R ventricle -Blood flows through ASD or foramen ovale to the left side of the heart and through a VSD to the right ventricle and out to the lungs - often co-occur w/ PS + TGA - deoxy + oxyg blood of left side of heart mixes Tricuspid Atresia Postoperative complications: dysrhythmias, HTN, pleural/pericardial effusions, ventricular dysfunction, protein-losing enteropathy, atrial dysrhythmias, late ventricular dysfunction, developmental delays Signs/Symptoms Treatment Cyanotic at birth Surgical tx: Mild cyanosis that worsens Blalock-Taussig shunt operation Complete repair systolic murmur (moderate) Blue spells/tet (acute episodes of cyanosis & hypoxia) Anoxia Cyanosis Tachycardia Dyspnea Hypoxemia (acute or chronic) Medication IV infusion prostaglandin E1 at 0.1 mcg/kg/min Surgical Shunt placement atrial septostomy (if ASD is small) pulmonary artery banding (if clubbing blood to lung increases) FETAL HEART DEFECTS, CLASSIFICATION, & TYPES OBSTRUCTIVE DEFECTS Pathophysiology Signs/Symptoms Treatment - narrowing near insertion of ductus arteriosus - Cause increased pressure in upper extremity/head -decreases pressure in lower extremities - defect is outside the heart and pericardium - best to get elective surgery for in 1st 2 years of life ↑BP w/ bounding pulses in upper extremities Non-surgical Balloon angioplasty (for older kids/adults) **15% - 30% risk for recurrence in patients who got surgery as infants underwent surgical repair as infants *** Coarctation of Aorta Complications: HTN, ruptured aorta, aortic aneurysm, stroke, recoarctation of aorta - Narrowing of aortic valve -causes resistance to blood flow in LV -resists the LV trying to pump blood out of heart -causes HTN in pulmonary system ***2 Types*** 1. Valvular aortic stenosis: most common type; caused by malformed bicuspid valve ; (1) obstruction is progressive; (2) sudden MI/ischemia occurs (or low cardiac output) can result in sudden death; (3) surgical repair rarely end w/ normal valve *NO strenuous physical activity* Aortic Stenosis 2. Subvalvular aortic stenosis: stricture caused by a fibrous ring Complications: ↓ cardiac output, MI, pulmonary HTN, scarred LV muscles (causes mitral insufficiency) ↓ BP w/ weak pulses in lower extremities Infants: signs of HF Sever acidosis Surgical 1st line for infants under 6mo Percutaneous balloon angioplasty dizziness, headaches, fainting, nose bleeds (epistaxis) ↓ cardiac output left ventricular hypertrophy (end-diastolic pressure) pulmonary vascular congestion Pulmonary HTN Infant S/S: hypotension, faint pulses, tachycardia, poor feeding Children: exercise intolerance, chest pain, dizziness w/ prolonged standing; systolic ejection murmur VALVULAR STENOSIS Surgical Repair: catheterization balloon dilation (1st Line treatment), Aortic valvotomy (Rarely used), Aortic valve replacement (if they’ve had a valve before) Non-Surgical Repair: balloon angioplasty dilation SUBVALVULAR STENOSIS Surgical Repair: cut the fibromuscular ring, patch the LV, valve replacement FETAL HEART DEFECTS, CLASSIFICATION, & TYPES MIXED DEFECTS Characteristics: Defects impede blood flow out of the ventricles ; blood exiting the heart meets a narrowed area (stenosis) that cause obstruction to blood flow Pathophysiology Signs/Symptoms Medication IV prostaglandin E1 - The pulmonary artery switches place with Aorta Severely cyanosis NORMAL Heart Circulation Aorta: carries blood from LV → rest of body Pulmonary Artery: carries blood from RV → lungs ABNORMAL Transposition of Great Artery Aorta: carries blood from RV → lungs Pulmonary Artery: carries blood from LV → rest of body Transposition of Great Arteries/Vessels Treatment Depressed function at birth (to keep ductus arteriosus open, keep oxygen saturation 75% or higher & maintain cardiac output) Symptoms of HF Surgical Repair Arterial Switch Cardiomegaly (best 1st few weeks of life) Rastelli procedure -There is no communication between systemic & pulmonary circulations (For infants w/ TGA, VSD, severe PS) - failure of pulmonary veins to join L atrium - pulmonary veins instead connect to systemic circulation via the R atrium OR other veins (like superior vena cava) Cyanosis in early life - more pulmonary blood = less cyanosis Total Anomalous Pulmonary Venous Connection End Result: -mixed blood returns to R atrium - R-to-L shunting from R atrium to L atrium -O2 saturation of both heart chambers is equal - R atrium receives all the blood that normally flow into the L atrium -Causes R side of heart to hypertrophy while left side remain small Asymptomatic if no obstruction present HF symptoms Surgical Repair Corrective Repair (Links pulmonary vein back to L atrium, closes ASD) FETAL HEART DEFECTS, CLASSIFICATION, & TYPES MIXED DEFECTS (cont.) Characteristics (cont.): Pressure in the ventricles & great artery before the obstruction is increased, and the pressure in the area beyond the obstruction is decreased ; location of the narrowing is usually near the valve ; obstruction on L side of heart causes HF symptoms; Severe obstruction on R side = cyanosis Pathophysiology Signs/Symptoms Treatment -The two major arteries (aorta + pulmonary artery) fail to separate, leaving one large artery space (AKA the truncus arteriosus) moderate to severe HF Surgical Repair Corrective Repair & Homograph: occurs 1st month of life; closes the VSD so truncus arteriosus gets blood flow from the L ventricle ; remove pulmonary arteries from aorta and attach them to R ventricle via of homograft -Blood from both L + R ventricles empty into the truncus arteriosus variable cyanosis poor growth activity intolerance -This causes systemic & pulmonary blood to mix = overall blood becomes desaturated = hypoxemia -pulmonary blood flow ↑; systemic blood flow ↓ Truncus Arteriosus -Pulmonary vascular disease develops at an early age in patients with truncus arteriosus. - Underdevelopment of the left side of the heart, resulting in a hypoplastic (small size than normal) left ventricle and aortic atresia. -blood from L atrium flows across the patent foramen ovale to the R atrium & R ventricle, and out the pulmonary artery. The descending aorta receives blood from the PDA supplying systemic blood flow HYPOPLASTIC BLOOD FLOW: Hypoplastic Left Heart Syndrome L atrium blood (saturated) mixes w/ R atrium blood (desaturated) →R ventricle → pulmonary artery→ lungs → ductus arteriosus → aorta → to rest of the body **Hypoplastic = smaller size than normal** - coronary + cerebral vessels receive blood by retrograde flow through the hypoplastic ascending aorta diastolic /holosystolic/L sternal murmur 35% of patients have 22q11 gene deletion mild cyanosis -Will need to replace as child grows Surgical Repair Multi stage repair (Norwood & Glenn shunt procedure signs of HF decreased cardiac output fatal in the first months of life without intervention Long-term problems w/ repair: worsening ventricular function, tricuspid regurg, recurrent aortic arch narrowing, dysrhythmias, developmental delays Heart Transplantation Mechanical ventilation Medication IV prostaglandin E1 (to maintain ductal patency & adequate systemic blood flow) FETAL HEART DEFECTS, CLASSIFICATION, & TYPES GENERAL BACKGROUND INFO Increased Pulmonary Blood Flow: -Blood flow from higher-pressure L side of heart to lower-pressure R side (left-to-right shunt); Can cause HF symptoms ; Increased blood volume on the right side of the heart increases pulmonary blood flow at the expense of systemic blood flow. Decreased Pulmonary Blood Flow: Result in cyanosis Obstructive Defects: Mixed Defects: Can lead to hypoxemia (with or w/out cyanosis) & HF; Hypoxemia & HF usually co-occur with these defects PRENATAL CIRCULATION POSTNATAL CIRCULATION FETAL HEART DEFECTS, CLASSIFICATION, & TYPES