- Thesis")
SCHOOL 1OF 1BUSINESS 1AND 1MANAGEMENT 1
AN 1ANALYSIS 1OF 1THE 1GOVERNMENT 1AND 1IMPLEMENTING 1PARTNERS
1COST 1IMPLICATION 1ON 1HIV/AIDS 1CASE 1MANAGEMENT 1INFECTIONS
1FROM 12012 1- 12017: 1A 1CASE 1OF 1WESTERN 1PROVINCE, 1ZAMBIA
STUDENT 1NAME: LUCKY 1MUSETA
STUDENT 1NUMBER: 1 1AFIN1421567
Thesis 1submitted 1in 1partial 1fulfillment 1of 1the 1award 1of 1a 1bachelor’s
1degree 1in 1Business 1Economics 1and 1Management 1Studies 1of 1the
1University 1of 1Lusaka
2021
2
DEDICATION
I 1wish 1to 1dedicate 1this 1research 1to 1my 1mother, 1wife, 1children 1and 1my 1friends,
1for 1their 1prayers 1and 1encouragement 1they 1rendered 1to 1me 1and 1all 1my 1family
1members 1for 1their 1financial, 1material 1and 1spiritual 1support 1and 1finally 1to 1my
1friends 1for 1their 1advice 1during 1the 1writing 1of 1this 1research 1report.
i
DECLARATION
I 1LUCKY 1MUSETA, 1hereby 1declaring 1that 1this 1is 1my 1original 1work 1that 1has
1never 1before 1been 1presented 1to 1any 1university 1or 1institution 1for 1any 1award 1of
1a 1degree, 1diploma 1or 1certificate.
Name: 1LUCKY 1MUSETA
Signature: 1_________________Date: 1_________________
ii
APPROVAL
This 1report 1has 1been 1approved 1as 1partial 1fulfilment 1of 1the 1requirement 1for 1the
1award 1of 1the 1Bachelor’s 1Degree. 1
Supervisor’s 1name: 1 1Dr 1Matthews 1C 1Hara
Supervisor’s
1signature…………………………Date……………………………………………..
iii
ACKNOWLEDGEMENTS
I 1would 1like 1to 1use 1this 1opportunity 1and 1medium 1to 1extend 1my 1highest
1gratitude
to 1my 1Academic 1Supervisor 1Dr 1Matthews 1Hara 1who 1has 1been 1very 1supportive
1from
the 1inception 1to 1completion 1of 1this 1Dissertation. 1Dr 1Matthews 1Hara 1has 1been 1a
1motivator,
an 1advisor 1who 1challenged 1me 1to 1never 1settle 1for 1mediocrity. 1His 1guidance,
inspiration 1and 1motivation 1were 1vital 1to 1the 1completion 1of 1this 1Dissertation 1as
this 1was 1the 1single 1greatest 1piece 1of 1work 1that 1I 1have 1done. 1
iv
LIST 1OF 1FIGURES
Figure 2.1: 1Conceptual 1Framework………………………………………………………11
Figure 14.1: 1indicates 1the 1benefits 1from 1the 1programs 1which 1were 1established 1in
12012 1to 1prevent 1and 1reducing
1HIV/AIDS…………………………………………………………16
Figure 4.2 1Shows 1the 1provincial 1HIV 1spending 1in 1Zambia 1(US$m, 1%, 120152017...……18
Figure 14.3: 1shows 1the 1percentage 1of 1each 1provincial 1HIV 1grants 1which 1was
1allocated...…19 1
Figure 14.4: 1shows 1the 1National 1AIDS 1Spending 1Assessment 1towards 1reducing 1the
1HIV/AIDS 1infections 1in 1Zambia 1from 120122017…………………………………………201
Figure 4.5: 1Shows 1Zambia 1HIV 1funding 1sources 120122015……………………………….22
Figure 14.6: 1Agents 1of 1HIV 1funding 1in 1Zambia 1(US$m, 120152017)..……………………...22
Figure 4.7: 1shows 1the 1general 1programs 1which 1were 1done 1by 1the
1government……………25
v
LIST 1OF 1TABLES
Table 4.1: 1indicates 1the 1best 1investment 1to 1be 1undertaken 1towards 1HIV 1high
1impact
1activities…………………………………………………………………………………….22
Table 4.2: 1Goal: 1To 1reduce 1the 1incidence 1and 1prevalence 1of
1HIV……………………23-24
vi
LIST 1OF 1ACRONYMS
ART 1– 1Antiretroviral 1Treatment
ARV- 1Antiretroviral 1drugs
CDC 1– 1Centers 1for 1Disease 1Control 1and 1Prevention
CHAZ 1– 1Churches 1Health 1Association 1of 1Zambia
CIDRZ 1- 1Centre 1for 1Infectious 1Diseases 1Research 1in 1Zambia
CMMB 1– 1catholic 1Medical 1Mission 1Board
CRS 1– 1Catholic 1Relief 1services
DAPP 1– 1Development 1Aid 1from 1people 1to 1People
DHD 1– 1District 1Health 1Director
DHO 1– 1District 1Health 1Office
HIV 1- 1Human 1Immunodeficiency 1Virus
ICAP 1– 1International 1Centre 1for 1AIDS 1Program
MTEF 1- 1Mid-Term 1Expenditure 1Framework
PEPFAR 1– 1Presidents 1Emergency 1Plan 1for 1Aids 1Relief
QI/QA 1– 1Quality 1Improvement 1/Quality 1Assurance
SOPs 1– 1Standard 1Operating 1Procedures
vii
SPSS 1– 1Software 1Package 1for 1Social 1Scientists
STD 1– 1sexually 1Transmitted 1Diseases
TB 1– 1Tuberculosis
UNAIDS 1– 1United 1Nations 1Programme 1on 1HIV/AIDS
WHO 1– 1World 1Health 1Organisation
WPHO 1– 1Western 1Provincial 1Health 1Office
WPHO 1CoAg 1– 1Western 1Provincial 1Health 1Office 1Cooperative 1Agreement
ZAMPHIA 1- 1Zambia 1Population-based 1HIV 1Impact 1Assessment
UHC- 1Universal 1Health 1Coverage
MHBP- 1minimum 1health 1benefits 1package
NASA 1- 1National 1AIDS 1Spending 1Assessment
NASF- 1National 1AIDS 1Strategic 1Framework
viii
TABLE 1OF 1CONTENT
DEDICATION ............................................................................................................................ i
DECLARATION .......................................................................................................................ii
APPROVAL ............................................................................................................................ iii
ix
LIST 1OF 1FIGURES ............................................................................................................... v
LIST 1OF 1TABLES ................................................................................................................ vi
LIST 1OF 1ACRONYMS .......................................................................................................vii
TABLE 1OF 1CONTENT ........................................................................................................ ix
ABSTRACTS ..........................................................................................................................xii
CHAPTER 1ONE: 1INTRODUCTION .................................................................................. 14
1.0 1Introduction .................................................................................................................. 14
1.1 1Background 1of 1the 1study ........................................................................................ 14
1.2 1Statement 1of 1the 1problem ....................................................................................... 16
1.3 1Research 1Objectives ................................................................................................... 17
1.3.1 1General 1Objective .................................................................................................... 17
1.3.2 1Specific 1Objectives .................................................................................................. 17
1.4 1Research 1Questions .................................................................................................... 17
1.5 1Significance 1of 1the 1study ........................................................................................ 17
1.6 1Scope 1of 1the 1study .................................................................................................. 17
1.7 1Definitions 1of 1the 1key 1terms ................................................................................. 17
CHAPTER 1TWO: 1LITERATURE 1REVIEW .................................................................... 18
2.0 1Introduction .................................................................................................................. 19
2.1 1Related 1literature ........................................................................................................ 19
2.2 1Theoretical 1Framework .............................................................................................. 20
2.3
Empirical 1review ..................................................................................................... 21
2.3.1 1The 1best 1investment, 1need 1based 1options 1to 1be 1undertaken 1towards 1HIV
1high 1impact 1activities ..................................................................................................... 21
2.3.2 1The 1preparedness 1of 1the 1government 1in 1taking 1up 1the 1HIV 1program .... 22
2.4 1Conceptual 1framework ............................................................................................... 24
2.5 1Chapter 1summary ....................................................................................................... 25
CHAPTER 1THREE: 1RESEARCH 1METHODOLOGY .................................................... 26
x
3.0 1Introduction .................................................................................................................. 26
3.1 1Study 1Design .............................................................................................................. 26
3.2 1Study 1target 1population ............................................................................................ 26
3.3 1Study 1sample 1size ..................................................................................................... 26
3.4 1Sampling 1method........................................................................................................ 26
3.5 1Data 1collection............................................................................................................ 27
3.6 1Data 1analysis .............................................................................................................. 27
3.7 1Data 1management 1and 1quality ................................................................................ 27
3.8 1Ethical 1consideration .................................................................................................. 28
CHAPTER 1FOUR: 1DATA 1ANALYSIS 1AND 1INTERPRETATION ........................... 29
4.0 1Introduction .................................................................................................................. 29
4.1 1The 1benefits 1derived 1from 1the 1program 1since 1its 1establishment 1in 12012 1in
1Western 1Province 1establish 1how 1much 1investment 1has 1been 1made 1towards
1reducing 1the 1HIV/AIDS 1infections. .............................................................................. 29
4.2 1The 1best 1investment, 1need 1based 1options 1to 1be 1undertaken 1towards 1HIV
1high 1impact 1activities 1in 1Western 1Province .............................................................. 34
4.3 1The 1preparedness 1of 1the 1government 1in 1taking 1up 1the 1HIV 1program 1in
1Western 1Province ............................................................................................................... 2
CHAPTER 1FIVE: 1CONCLUSION 1AND 1RECOMMENDATIONS ................................ 5
5.0 1Introduction .................................................................................................................... 5
5.1 1Conclusion...................................................................................................................... 5
5.2 1Recommendations .......................................................................................................... 6
5.2.1
Zambia 1should 1develop 1a 1health 1and 1HIV/AIDS 1(combined) 1financing
1strategy6
5.2.2
Zambia 1should 1be 1assisted 1in 1finding 1options 1and 1lessons 1from 1other
1countries 1exposed 1to 1similar 1situations......................................................................... 6
5.2.3
Zambia 1should 1consider 1establishing 1trust 1funds, 1besides 1the 1already
1established 1health 1insurance 1programs. .......................................................................... 6
xi
5.2.4
Low 1rates 1of 1insurance 1coverage 1pose 1a 1challenge 1to 1the 1long-run
1sustainability 1and 1equity 1of 1access 1to 1HIV 1and 1health 1services 1in 1the 1face
1of 1declining 1donor 1resources. ......................................................................................... 6
5.3 1Future 1research ............................................................................................................. 6
REFERENCES .......................................................................................................................... 8
Appendix 11: 1 1Questionnaire 1District 1Health 1Office ..................................................... 11
Appendix 12: 1 1Interview 1guide 1for 1District 1Health 1Office ......................................... 14
Appendix 13: 1 1Interview 1guide 1for 1Implementing 1partners 1(NGOs).......................... 16
ABSTRACT
The 1research 1looked 1into 1an 1investigation 1into 1analysis 1the 1government 1and
1implementing 1partners 1cost 1implication 1on 1HIV/AIDS 1case 1management 1from
12012 1- 12017: 1a 1case 1of 1Western 1Province, 1Zambia. 1The 1research 1was
1conducted 1in 1western 1province 1of 1Zambia. 1With 1the 1sample 1size 1of 142
1respondents 110 1respondents 1were 1implementing 1partners 1(NGO’s) 1and 1from 1each
1organisation 1only 12 1respondents 1were 1selected 1for 1this 1study 1and 116
xii
1respondents 1were 1from 1the 1district 1health 1office 1accountant 1directors’ 12
1respondent 1from 1each 1district 1of 1western 1province.
Respectable 1research 1design 1makes 1sure 1the 1information 1gathered 1is 1steady 1with
1the 1study 1objectives 1and 1data 1collected 1by 1accurate 1and 1economical 1procedure.
1This 1research 1employed 1qualitative 1and 1quantitative 1research 1design 1the 1study
1specifically, 1was 1more 1of 1a 1descriptive 1design 1and 1little 1mathematical 1in
1nature, 1this 1was 1used 1to 1obtain 1the 1relevant 1information 1from 1respondents. 1
The 1sample 1method 1which 1was 1used 1in 1this 1survey 1is 1purposive 1sampling 1it
1was 1employed 1for 1every 1respondent 1because 1it 1was 1specific 1on 1the 1HIV/AIDS
1cost 1implication 1management 1as 1it 1allowed 1the 1researcher 1to 1interact 1with
1respondents 1who 1are 1familiar 1with 1the 1study 1and 1hence 1assist 1the 1researcher 1to
1collect 1relevant 1information 1required. 1
This 1study 1hired 1triangulation 1methods 1as 1the 1way 1of 1data 1collection.
1Triangulation 1was 1used 1because 1it 1combines 1different 1methods 1of 1data
1collection. 1Skill 1shows, 1that 1no 1solitary 1instrument 1is 1inadequate 1in 1collecting
1valid 1and 1reliable 1data. 1The 1study 1engaged 1a 1series 1of 1data 1collection 1methods
1and 1instruments 1which 1contains; 1documentary 1analysis, 1face-to-face 1interviews,
1structured 1questionnaires, 1semi 1questionnaires 1and 1group 1discussions.
The 1findings 1of 1the 1study 1showed 1that 1ARVs 1were 1the 1highest 1considered
1benefit 1of 1programs 1in 1trying 1to 1weaken 1the 1virus 1and 1boost 1up 1the 1immune
1system 1of 1people 1who 1are 1HIV 1positive. 1Followed 1by 1Voluntary 1counselling
1and 1testing 1(VCT) 1about 190% 1of 1the 1population 1of 1western 1province 1have
1done 1it 1once 1or 1twice 1in 1their 1life 1to 1know 1their 1status. 1Anti-natal 1and
1counselling 1of 1couples 1are 1also 1some 1of 1the 1benefits 1of 1the 1programs 1which
1were 1been 1established 1since 12012. 1Male 1Circumcision 1(CM) 1is 1another 1program
1which 1was 1established 1in 1try 1to 1reduce 1HIV/AIDS 1of 1which 1the 1study 1showed
1that 1most 1males 1have 1under 1gone 1the 1circumcision 1process.
1
xiii
CHAPTER 1ONE: 1INTRODUCTION
1.0 1Introduction 1
The 1research 1study 1analysed 1the 1cost 1implication 1of 1the 1HIV 1infection 1in 1western
1province 1of 1Zambia. 1This 1chapter 1presents 1the 1background 1of 1the 1problem 1under 1study,
1statement 1of 1the 1problem, 1research 1objectives, 1research 1questions, 1hypothesis, 1and 1rationale
1to 1the 1study, 1scope 1and 1operation 1definitions 1for 1the 1key 1terms.
1.1 1Background 1of 1the 1study
According 1to 1World 1Health 1Organisation 1(WHO), 1(2019) 1HIV 1continues 1to 1be 1a 1major
1global 1public 1health 1issue, 1having 1claimed 1more 1than 132 1million 1lives 1so 1far. 1However,
1with 1increasing 1access 1to 1effective 1HIV 1prevention, 1diagnosis, 1treatment 1and 1care,
1including 1for 1opportunistic 1infections, 1HIV 1infection 1has 1become 1a 1manageable 1chronic
1health 1condition, 1enabling 1people 1living 1with 1HIV 1to 1lead 1long 1and 1healthy 1lives.
In 1Zambia, 1around 148,000 1adults 1and 15,400 1children 1became 1newly 1infected 1with 1HIV 1in
12018 1(DHIS 12019). 1New 1infections 1are 1slowly 1decreasing 1- 1in 12010, 147,000 1adults 1and
18,800 1children 1were 1newly 1infected 1with 1HIV (UNAIDS, 2019). 1 1Overall, 1this 1equates 1to
1a 113% 1reduction 1in 1new 1infections 1since 12010. 1
In 1the 1same 1year 1around 11.2 1million 1people 1in 1Zambia 1were 1living 1with 1HIV 1and
117,000 1people 1died 1from 1an 1AIDS-related 1illness (UNAIDS, 2019). 1The 1number 1of 1people
1newly 1diagnosed 1with 1HIV 1and 1with 1active 1tuberculosis 1(TB) 1entering 1care 1has 1fallen
1significantly 1from 166% 1in 12015 1to 110 12017. 1
The 1country 1has 1a 1generalised 1HIV 1epidemic 1driven 1by 1heterosexual 1sex. 1In 12018, 111.3%
1of 1adults 1were 1living 1with 1HIV, 1a 1slight 1reduction 1on 12010 1levels 1when 113% 1of
1adults 1were 1living 1with 1HIV. 1Women, 1particularly 1adolescent 1girls 1and 1young 1women,
1are 1worse 1affected 1than 1men. 1In 12017, 114.3% 1of 1women 1aged 115 1and 1over 1were
1living 1with 1HIV, 1compared 1to 18.8% 1of 1their 1male 1counterparts. 1Marginalised 1groups
1such 1as 1sex 1workers, 1transgender 1people, 1prisoners, 1people 1who 1inject 1drugs, 1gay 1men
1and 1other 1men 1who 1have 1sex 1with 1men 1are 1also 1disproportionately 1affected 1by 1HIV.
In 12018, 178% 1of 1all 1people 1living 1with 1HIV 1were 1on 1treatment. 1As 1of 12019, 187% 1of
1people 1living 1with 1HIV 1were 1aware 1of 1their 1status, 1and 189% 1on 1treatment 1and 175%
1were 1virally 1suppressed. 1
14
In 12016, 1life 1expectancy 1for 1men 1was 160 1years 1and 1for 1women 164 1years. 1This 1is 1a
1considerable 1increase 1from 1the 12012 1average 1life 1expectancy 1of 149.4 1years, 1partly 1due
1to 1improved 1access 1to 1antiretroviral 1treatment 1(ART).
Prevalence 1among 1adults 1in 1Zambia 1has 1changed 1little 1over 1the 1last 1decade 1despite
1decreasing 1infection 1rates. 1Life 1expectancy 1among 1people 1living 1with 1HIV 1has 1improved
1significantly 1as 1a 1result 1of 1scaled-up 1treatment 1programmes 1in 1recent 1years. 1Among
1people 1who 1have 1been 1able 1to 1access 1antiretroviral 1treatment 1(ART), 175% 1are 1now
1virally 1suppressed. 1HIV 1continues 1to 1fuel 1the 1country’s 1tuberculosis 1epidemic. 1Women
1are 1disproportionately 1affected 1by 1HIV, 1with 1prevalence 1among 1young 1women 1more 1than
1double 1that 1of 1young 1men.
According 1to 1Western 1Provincial 1Health 1Office 1Health 1Information 1System 1(2005), 1Western
1province 1started 1offering 1antiretroviral 1drugs 1in 12005 1at 1Lewanika 1General 1Hospital. 1And
1later 1the 1service 1was 1rolled 1out 1to 1other 1district 1hospitals 1till 1the 1implementation 1of 1the
1current 1test 1and 1treat 1in 1all 1the 1facilities 1in 1accordance 1to 1the 12018 1HIV 1Consolidated
1guidelines. 1In 1western 1province, 1about 198, 1000 1people 1are 1on 1antiretroviral 1treatment
1(ART), 1interpreting 1a 19% 1of 1the 1total 1provincial 1population. 1According 1to 1ZAMPHIA
12018, 1the 1viral 1suppression 1was 1at 153.1% 1making 1the 1province 1to 1be 1the 1most
1infectious 1in 1Zambia 1with 1the 1HIV 1prevalence 1at 116% 1the 1highest 1among 1all 1the
1provinces.
According 1to 1the 1Mid-Term 1Expenditure 1Framework 1(MTEF) 12019 1– 12022 1for 1Western
1Provincial 1Health 1Office, 1the 1province 1has 1been 1receiving 1financial, 1human 1resource,
1logistical 1and 1technical 1support 1from 1different 1cooperating 1partners 1in 1the 1management 1of
1HIV 1infection. 1The 1support 1came 1from 1the 1following 1partners; 1Western 1Provincial 1Health
1Office 1Cooperative 1Agreement 1(WPHO 1CoAg) 1with 1Western 1Provincial 1Health 1Office
1since 12006, 1Centre 1for 1Infectious 1Diseases 1Research 1in 1Zambia 1(CIDRZ) 1since 12007,
1Churches 1Association 1of 1Zambia 1(CHAZ) 1since 12007 1in 1Mission 1hospitals, 1MARCH
1Zambia 1since 12012, 1IntraHealth 1Zambia 1since 12012, 1ICAP 1since 12018, 1University 1of
1Maryland 1since 12018, 1Chemonics 1since 12016, 1CRS 1since 12018, 1DAPP 1since 12010,
1Catholic 1Medical 1Mission 1Board 1(CMMB) 1since 12012, 1Discover 1Health 1since 12017.
15
1.2 1Statement 1of 1the 1problem
With 1the 1background 1above, 1Western 1province 1has 1been 1receiving 1a 1lot 1of 1support 1from
1different 1partners 1to 1curb 1the 1HIV 1epidemic, 1which 1in 1turn 1has 1not 1been 1analyzed
1evaluated 1as 1to 1its 1see 1the 1impact 1the 1support 1has 1on 1its 1contribution 1towards 1reducing
1the 1HIV 1infections. 1Of 1which 1considering 1that 1the 1majority 1of 1the 1support 1given 1is
1donor 1based 1which 1is 1dependent 1on 1the 1satisfying 1action 1of 1the 1key 1HIV 1driving
1factors 1for 1example, 1attainment 1of 1the 1HIV 1targets.
The 1study 1aimed 1at 1analyzing 1the 1cost 1implications 1in 1the 1reduction 1of 1the 1HIV
1infections 1and 1preparedness 1of 1the 1government’s 1take 1up 1of 1the 1management 1of 1the
1HIV 1program 1in 1western 1province. 1Though 1the 1program 1is 1beneficial 1to 1the 1province 1it
1being 1donor 1driven 1the 1program 1is 1time 1bound 1and 1government 1is 1expected 1to 1take 1it
1over 1once 1the 1program 1comes 1to 1an 1end. 1However, 1there 1is 1no 1road 1map 1in 1place 1on
1how 1the 1government 1will 1take 1up 1the 1HIV 1program. 1The 1program 1was 1started 1by
1donors 1due 1to 1government’s 1financial 1incapacity 1to 1undertake 1it. 1The 1program 1has 1been
1in 1operation 1since 1and 1in 1all 1that 1time 1the 1government 1has 1only 1provided 1administrative
1support 1but 1not 1financial. 1It 1is 1however, 1not 1clear 1whether 1there 1is 1a 1parallel 1program
1from 1government 1to 1take 1over 1on 1the 1conclusion 1of 1the 1donor 1support. 1
So 1far 1there 1has 1not 1been 1any 1research 1done 1in 1the 1province 1to 1look 1at 1the 1cost 1that
1has 1been 1put 1in 1by 1different 1partners 1in 1the 1fight 1against 1HIV 1as 1well 1as 1whether
1there 1is 1a 1parallel 1program 1from 1government 1to 1take 1over 1the 1program 1on 1the 1ending
1of 1donor 1support. 1As 1this 1will 1ascertain 1how 1much 1the 1program 1has 1received 1in
1comparison 1with 1the 1reduction 1of 1the 1HIV 1infections.
There 1is 1no 1road 1map 1in 1place 1on 1how 1the 1government 1will 1take 1up 1the 1HIV 1program
1and 1so 1the 1study 1will 1also 1aim 1at 1assessing 1the 1capacity 1of 1the 1government 1in 1taking
1up 1the 1program.
16
1.3 1Research 1Objectives
1.3.1 1General 1Objective
To 1analyse 1the 1government 1and 1implementing 1partners 1cost 1implication 1on 1HIV/AIDS 1case
1management 1from 12012 1- 12017: 1a 1case 1of 1Western 1Province, 1Zambia.
1.3.2 1Specific 1Objectives
i.
To 1assess 1benefits 1derived 1from 1the 1program 1since 1its 1establishment 1in 12012 1in
1Western 1Province 1establish 1how 1much 1investment 1has 1been 1made 1towards 1reducing
1the 1HIV/AIDS 1infections
ii.
To 1establish 1the 1best 1investment, 1need 1based 1options 1to 1be 1undertaken 1towards
1HIV 1high 1impact 1activities 1in 1Western 1Province
iii.
To 1determine 1the 1preparedness 1of 1the 1government 1in 1taking 1up 1the 1HIV 1program
1in 1Western 1Province
11.4 1Research 1Questions
i.
What 1are 1the 1benefits 1derived 1from 1the 1program 1since 1its 1establishment 1in 12012
1in 1Western 1Province 1establish 1how 1much 1investment 1has 1been 1made 1towards
1reducing 1the 1HIV/AIDS 1infections.
ii.
1What 1is 1the 1best 1investment, 1need 1based 1options 1to 1be 1undertaken 1towards 1HIV
1high 1impact 1activities 1in 1Western 1Province 1
iii.
How 1is 1the 1preparedness 1of 1the 1government 1in 1taking 1up 1the 1HIV 1program 1in
1Western 1Province?
1.5 1Significance 1of 1the 1study 1
The 1findings 1can 1help 1stakeholders 1know 1the 1government 1and 1implementing 1partners 1cost
1implication 1on 1HIV/AIDS 1case 1management 1infections 1from 12012 1- 12017: 1a 1case 1of
1western 1province, 1Zambia
11.6 1Scope 1of 1the 1study
The 1study 1took 1place 1in 1Western 1Province 1covering 1period 12012-2017 1of 1Zambia.
1.7 1Definitions 1of 1the 1key 1terms
- 1Cost 1implications: 1the 1amount 1of 1time, 1money, 1and 1energy 1required 1to 1manage 1the
1HIV 1program
- 1Interventions: 1designed 1strategies 1aimed 1at 1address 1a 1problem
17
- 1Mentorship: 1a 1process 1of 1imparting 1knowledge 1and 1skills 1from 1a 1well-trained 1or
1knowledgeable 1person 1to 1another
18
CHAPTER 1TWO: 1LITERATURE 1REVIEW
2.0 1Introduction
This 1chapter 1deals 1with 1the 1review 1of 1literature 1on 1the 1studies 1that 1have 1been 1done 1on
1the 1area 1under 1study. 1literature 1refers 1to 1all 1sources 1of 1published 1data 1and 1is 1a 1written
1summary 1from 1literature 1research. 1 1literature 1review 1describes 1theoretical 1perspectives 1and
1previous 1research 1findings 1regarding 1the 1problem 1at 1hand. 1The 1purpose 1of 1literature
1review 1is 1described 1by 1Akpo 1(2002) 1as 1that 1of 1providing 1the 1context 1for 1the 1research
1by 1looking 1at 1the 1work 1of 1what 1has 1already 1been 1done 1in 1the 1subject 1area. 1The
1chapter 1shall 1present 1the 1literature 1to 1be 1reviewed 1on 1the 1cost 1implications 1of 1the 1HIV
1infection. 1Some 1of 1the 1cost 1will 1include 1the 1financial, 1technical, 1logistical, 1equipment
1and 1human 1resource 1support. 1The 1purpose 1of 1reviewing 1the 1literature 1shall 1be 1to 1know
1main 1variables 1to 1contribute 1towards 1the 1cost 1implications 1of 1the 1HIV 1infection.
1Furthermore, 1the 1review 1of 1the 1literature 1shall 1also 1identify 1the 1gaps 1from 1previous
1studies 1done 1and 1also 1variables 1that 1were 1used 1to 1formulate 1the 1objectives. 1
2.1 1Related 1literature 1
Peters, 1(2010) 1found 1that 1both 1the 1European 1the 1American 1governments 1had 1shifted 1their
1attention 1from 1treatment 1to 1prevention 1of 1HIV 1in 1their 1support. 1Leibowitz, 1(20111)
1found 1that 1treatment 1expenditures 1on 1HIV 1had 1overshadowed 1the 1prevention 1spending 1on
1HIV. 1Kates, 1(2005) 1said 1that 1Centres 1for 1Disease 1Control 1and 1Prevention 1(CDC) 1uses
1grants 1and 1cooperative 1agreements 1to 1fund 1research 1and 1non-research 1public 1health
1programs 1that 1advance 1the 1Agency’s 1public 1health 1mission. 1CDC’s 1Division 1of
1HIV/AIDS 1Prevention 1maintains 1an 1HIV 1Funding 1page 1with 1information 1on 1current 1CDC
1HIV 1prevention 1funding 1opportunities 1open 1for 1applicants 1as 1well 1as 1active 1grant
1programs 1for 1which 1awards 1have 1already 1been 1made. 1 1In 1addition, 1CDC’s 1National
1Prevention 1Information 1Network 1provides 1a 1database 1of 1HIV-related 1funding 1opportunity
1announcements 1from 1CDC 1and 1many 1other 1federal 1agencies, 1as 1well 1as 1funding
1opportunities 1related 1to 1viral 1hepatitis, 1STDs, 1tuberculosis, 1and 1school 1health. 1More
1information 1on 1CDC 1grants 1is 1available 1from 1CDC’s 1Office 1of 1Grants 1Services. 1The
1researcher 1further 1added 1that 1this 1is 1the 1CDC 1has 1many 1agencies 1that 1support 1human,
1financial, 1logistical 1and 1technical 1support 1services 1to 1different 1countries.
19
Banigbe, 1B, 1(2019) 1described 1that 1transitioning 1the 1responsibility 1for 1all 1or 1parts 1of 1a
1donor 1funded 1program 1to 1host 1government 1or 1local 1stakeholders 1is 1common 1in
1development 1programs, 1and 1is 1usually 1considered 1to 1be 1a 1sustainability 1strategy. 1Board,
1(2003) 1also 1agreed 1that 1indeed, 1development 1programs 1that 1do 1not 1plan 1to 1successfully
1incorporate 1a 1blueprint 1for 1local 1country 1ownership 1may 1be 1criticized 1for 1facilitating
1donor 1dependency. 1 1Odekunle, 1(2016) 1Despite 1the 1importance 1of 1the 1successful 1transition
1of 1PEPFAR 1efforts 1to 1donor 1recipient 1countries, 1the 1nature 1of 1these 1transitions 1is
1complex, 1and, 1has 1been 1met 1with 1challenges. 1Katz, 1(2013, 1also 1indicated 1that 1with
1increasingly 1aggressive 1global 1targets 1such 1as 1the 1UNAIDS 190-90-90 1goals, 1many 1have
1feared 1Presidents 1Emergency 1Plan 1for 1Aids 1Relief 1(PEPFAR) 1supported 1programs 1would
1not 1only 1fall 1short 1of 1these 1targets, 1but 1also 1lose 1the 1tremendous 1gains 1established 1in
1the 1earlier 1PEPFAR 1era. 1UNAIDS, 1(2014) 1said 1that 1their 1analysis 1had 1highlighted 1that
1clinics 1in 1Nigeria’s 1had 1major 1challenges 1in 1the 1provision 1of 1HIV 1services 1in 1the 1wake
1of 1the 1PEPFAR 1funding 1policy 1change. 1Providers 1describe 1reductions 1in 1the 1quality 1of
1care 1administered 1and 1in 1clinic 1attendance, 1along 1with 1human 1resource 1gaps 1as 1the
1greatest 1threats 1to 1delivering 1effective 1HIV 1care.
Atum, 1(2016) 1found 1that 1human 1resource 1shortages 1had 1been 1a 1persistent 1challenge 1during
1the 1rapid 1scale-up 1of 1ART 1in 1Low- 1and 1Middle-Income 1Countries 1(LMICs). 1Cailhol, 1J,
1(2013) 1also 1said 1that 1PEPFAR-supported 1sites 1had 1used 1creative 1strategies 1such 1as 1use
1of 1retired 1staff, 1formal 1and 1informal 1task-shifting, 1and 1development 1of 1new 1cadres 1of
1health 1workers 1to 1meet 1human 1resource 1needs 1for 1HIV 1care 1in 1Nigeria. 1Lawn, 1(2010)
1found 1that 1although 1PEPFAR 1still 1provided 1funds 1for 1CD4 1testing, 1viral 1load 1testing
1was 1no 1longer 1supported 1in 1many 1facilities 1of 1Nigeria. 1Critical 1laboratory 1infrastructure
1was 1undermined 1because 1many 1patients 1did 1not 1pay 1for 1required 1laboratory 1tests 1that
1were 1no 1longer 1supported 1by 1PEPFAR, 1but 1helped 1to 1subsidize 1laboratory 1operations.
2.2 1Theoretical 1Framework
2.2.1 1Theory 1of 1Planned 1Behaviour
Ajzen, 1(1991) 1described 1the 1theory 1of 1planned 1behaviour 1as 1that 1behaviour 1which 1is
1dependent 1on 1one’s 1intention 1to 1perform 1the 1behaviour. 1This 1will 1be 1done 1through;
1attitude, 1subjective 1norms 1and 1perceived 1behaviour. 1 1In 1this 1study 1the 1theory 1of 1planned
1behaviour 1entails 1that 1the 1attitude 1of 1the 1HIV 1implementing 1partners 1are 1clear 1that 1they
1would 1want 1to 1continue 1supporting 1the 1HIV 1program 1and 1on 1the 1other 1hand
20
1subjectively 1the 1government 1has 1no 1clear 1intentions 1to 1take 1up 1the 1full 1support 1of 1the
1program.
2.3 Empirical 1review 1
2.3.1 1The 1best 1investment, 1need 1based 1options 1to 1be 1undertaken 1towards 1HIV 1high
1impact 1activities
The 1adoption 1of 1an 1MHBP, 1however, 1does 1not 1imply 1that 1the 1delivery 1of 1services 1and
1health 1financing 1are 1only 1limited 1to 1those 1priority 1interventions. 1No 1country 1can 1finance
1all 1of 1the 1health 1services 1offered 1by 1modern 1medicine 1to 1all 1of 1its 1citizens.
1Constructing 1a 1MHBP 1that 1contains 1priority 1services 1is 1a 1way 1of 1recognizing 1this
1limitation, 1by 1channelling 1available 1financing 1with 1greater 1priority 1to 1those 1services.
1Other 1services 1of 1lower 1priority, 1such 1as 1referral 1care 1or 1less 1common 1diseases, 1are
1likely 1to 1continue 1to 1be 1delivered 1and 1receive 1some 1public 1financing, 1in 1addition 1to
1financing 1coming 1from 1patients 1and 1their 1families. 1For 1example, 1many 1developing
1countries 1in 1Latin 1America, 1such 1as 1Argentina, 1El 1Salvador, 1Nicaragua, 1and 1Guatemala,
1have 1defined 1MHBPs 1that 1focus 1on 1maternal 1and 1child 1health 1services 1and 1are 168
1targeted 1to 1low-income 1families. 1
Hospital 1services, 1not 1contained 1in 1the 1MHBP, 1continue 1to 1be 1offered 1universally 1to 1all
1citizens, 1or 1to 1the 1poor, 1but 1with 1considerable 1rationing 1through 1queues, 1demand
1deflection, 1and 1low 1quality 1of 1care. 1The 1MHBP 1services 1receive 1the 1funding 1needed 1to
1achieve 1the 1coverage 1targets 1set 1out 1by 1the 1ministry 1of 1health, 1while 1hospital 1and 1other
1services 1excluded 1from 1the 1MHBP 1receive 1residual 1funding. 1Box 15 1illustrates 1the
1approach 1taken 1by 1one 1country 1to 1model 1the 1need 1for 1the 1financing 1of 1health 1services
1within 1and 1outside 1of 1the 1UHC 1health 1benefits 1package. 1A 1tentative 1package 1was
1defined 1comprised 1of 1preventive 1and 1curative 1health 1interventions. 1(Barroy, 1Bitran 1et 1al.,
12015, 1unpublished 1report 1from 1the 1Democratic 1Republic 1of 1Congo). 1
The 1approach 1these 1researchers 1took 1was 1to 1project 1MHBP 1and 1other 1health 1system 1costs
1separately 1using 1different 1criteria. 1For 1MHBP 1services 1they 1used 1normative 1production
1functions 1that 1included 1some 1human 1resources, 1medical 1supplies, 1transportation 1costs, 1and
1medicines, 1cost 1out 1using 1local 1input 1costs, 1as 1well 1as 1expected 1output. 1For 1services
1outside 1of 1the 1MHBP, 1they 1relied 1on 1country-specific 1knowledge 1about 1the 1costs 1of
1hospital 1services, 1public 1health 1services, 1medical 1institutes, 1and 1the 1management 1of 1the
21
1health 1system 1to 1project 1future 1needs 1of 1human 1resources, 1infrastructure, 1and 1other
1operating 1expenditures.
2.3.2 1The 1preparedness 1of 1the 1government 1in 1taking 1up 1the 1HIV 1program
The 1Government 1of 1Zambia, 1the 1cooperating 1partners, 1the 1private 1and 1business
1communities 1will 1significantly 1meet 1the 1cost 1of 1implementing 1this 1plan. 1Implementation
1of 1this 1programme 1is 1going 1to 1cost 1approximately 1US$ 1348.8 1million. 1With 1the
1continuing 1decline 1in 1the 1price 1of 1ARV 1drugs 1and 1diagnostics 1it 1is 1expected 1that 1the
1unit 1cost 1of 1treatment 1will 1reduce 1over 1the 1period 1of 1time. 1
An 1estimation 1of 1the 1HIV 1resources 1needed 1to 1achieve 1the 1NASF 1goals, 1adjusted 1for
1the 1‘test 1and 1treat’ 1strategy 1that 1these 1needs 1continue 1to 1increase 1and 1if 1Zambia 1is 1to
1attain 1its 1goals, 1a 1potential 1funding 1gap 1could 1be 1experienced. 1 1Importantly, 1in 1the
1longer-term 1projections 1(e.g. 1EQUIP, 12017: 1T&T 1cost 1estimates 1to 12030), 1revealed 1that
1the 1costs 1will 1eventually 1begin 1to 1plateau 1around 12025, 1due 1to 1the 1impact 1of 1both 1the
1prevention 1efforts 1as 1well 1as 1the 1preventative 1effect 1of 1the 1scale-up 1of 1test 1and 1treat
1(NAC, 12017). 1
Zambia 1has 1applied 1the 1System 1of 1Health 1Accounts 1(SHA), 1formerly 1known 1as 1the
1National 1Health 1Accounts 1(NHA), 1which 1provides 1the 1total 1health-related 1spending 1in 1the
1country, 1including 1HIV 1(within 1the 1health 1sector), 1as 1shown 1in 1table 12 1below. 1HIV
1financing 1in 1Zambia 1has 1been 1predominantly 1donor 1supported 1as 1shown 1below, 1and 1the
1Government) 1contributed 112.1% 1of 1the 1health-related 1HIV 1spending 1(MOH, 12018: 1NHA
12016). 1According 1to 1the 1NHA 12016 1findings, 1HIV 1and 1STD 1programs 1and 1interventions
1took 134.78% 1of 1the 1General 1Health 1budget 1which 1translated 1to 17,14% 1of 1the 1national
1budget 1(MOH, 12018)..
Saleh 1et 1al 1(2018) 1comments 1that, 1most 1countries 1in 1the 1Sub-Saharan 1Africa 1region 1rely
1heavily 1on 1external 1assistance 1to 1finance 1their 1HIV/AIDS 1response, 1although 1the 1SubSaharan 1Africa 1region 1as 1a 1whole 1is 1less 1dependent 1on 1external 1financing 1than 1the 1four
1case 1study 1countries. 1The 1Sub-Saharan 1Africa 1average 1share 1of 1spending 1accounted 1for
1by 1external 1assistance 1was 1at 1its 1lowest 1in 12009 1(46 1percent), 1with 1the 1remaining 154
1percent 1financed 1by 1government 1and 1households. 1Among 1the 1case 1study 1countries, 1Côte
1d’Ivoire 1was 1the 1most 1dependent 1on 1external 1financing 1for 1HIV/AIDS 1in 1the 1past 1five
1years 1(2010-2015). 1
22
1Kenya’s 1extensive 1HIV/AIDS 1response 1has 1been 1financed 1mostly 1through 1external
1assistance 1as 1well. 1In 12010, 1it 1achieved 1its 1highest 1share 1of 1domestic 1financing 1for
1HIV/AIDS: 118 1percent 1of 1the 1total. 1However, 1the 1next 1year 1Kenya 1financed 1only 111.8%
1of 1its 1HIV/AIDS 1response 1with 1domestic 1resources 1while 1donors 1picked 1up 1the
1remaining 188.2 1percent. 1Tanzania’s 1dependence 1on 1external 1support 1for 1its 1HIV/AIDS
1interventions 1increased 1from 151.1 1% 1in 12005 1to 169.3 1percent 1in 12010. 1For 1these 1four
1case 1study 1countries, 1external 1funding 1represents 1upwards 1of 1two-thirds 1of 1all 1resources,
1with 1much 1of 1the 1external 1funding 1coming 1from 1bilateral 1donors, 1notably 1the 1U.S.
1President’s 1Emergency 1Plan 1for 1AIDS 1Relief 1(PEPFAR). 1For 1HIV/AIDS 1and 1a 1few
1other 1vertical 1programs, 1however, 1dependency 1on 1external 1funding 1is 1much 1higher 1for 1all
1countries, 1reaching 1between 170 1and 190%. 1This 1means 1that 1if 1international 1development
1assistance 1does 1decrease 1in 1future 1years, 1programs 1such 1as 1HIV/AIDS, 1malaria 1and
1tuberculosis 1are 1likely 1to 1suffer 1most 1(Saleh 1et 1al, 12018).
The 1Government 1of 1the 1Republic 1of 1Zambia 1(GRZ) 1through 1the 1National 1AIDS 1Council
1(NAC) 1has 1the 1overall 1responsibilities 1for 1coordinating 1all 1national 1HIV/AIDS/TB/STI
1activities 1as 1stipulated 1in 1the 1NAC 1act. 1NAC 1will 1undertake 1resource 1mobilisation 1as
1well 1as 1monitoring 1and 1evaluation 1of 1the 1programme. 1The 1MOH 1will 1be 1responsible 1for
1providing 1national 1leadership, 1implementation 1of 1policies, 1forging 1partnerships 1with 1key
1players, 1and 1coordination 1at 1national 1level. 1The 1MOH 1will 1also 1work 1closely 1with 1the
1National 1AIDS 1Council, 1Churches 1Health 1Association, 1Faculty 1of 1General 1Practitioners
1and 1Private 1Sector, 1Network 1of 1Zambian 1People 1Living 1with 1HIV/AIDS, 1Zambia
1National 1AIDS 1Network 1(ZNAN) 1and 1the 1different 1Cooperating 1Partners. 1The 1success 1of
1the 1implementation 1plan 1rests 1on 1these 1stakeholders 1recognising 1their 1role 1and 1embracing
1collaborative 1approaches. 1The 1Directorate 1of 1Clinical 1Care 1and 1Diagnostic 1Services 1of
1MOH 1through 1the 1National 1ART 1Programme 1Coordinator 1will 1provide 1the 1leadership
1through 1the 1implementation 1of 1effective 1systems 1and 1cooperation 1amongst 1stakeholders.
1The 1Coordination 1at 1provincial 1level 1will 1be 1provided 1by 1the 1Provincial 1Health 1Office
1(PHO) 1whereas 1the 1District 1Health 1Management 1Team 1(DHMT) 1will 1coordinate 1activities
1at 1district 1level. 1The 1district 1level 1institutions 1include 1the 1hospitals, 1health 1centres, 1Faith
1Based 1Organisations 1(FBO), 1NGOs, 1and 1the 1private 1sector. 1
23
2.4 1Conceptual 1framework
Conceptual 1framework 1is 1a 1set 1of 1coherent 1ideas 1or 1concepts 1organized 1in 1a 1manner 1that
1makes 1them 1easy 1to 1communicate 1to 1others 1or 1an 1organized 1way 1of 1thinking 1about
1how 1and 1why 1a 1study 1takes 1place 1and 1about 1how 1we 1understand 1its 1activities
1(Wimmer 1and 1Dominick 12003). 1In 1this 1study, 1a 1conceptual 1framework 1is 1an 1assessment
1of 1items 1and 1activities 1needed 1to 1be 1in 1action 1for 1cost 1implications 1of 1HIV 1infection
1management.
Figure 2.1 :Conceptual 1framework 1 1
Equipment
11111111111111111111111111
Laboratory 1Equipment
1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1Drugs
1 1 11supply
11111111111111111111111111111
Gloves 1
Financial 1Support
Mentorship
Funded 1Interventions
Boats
Meetings
Strategy 1Formulation
Salary 1and 1Incentive
Technical 1Support
Cost 1Implications 1of
1HIV 1Infection
1management
SOP 1Adherence
Strategy 1Formulation
QI/QA
Logistical 1Support
Human 1Resource
Motor 1vehicles
Trainings
Motor 1bikes
Hire 1of 1Professional
1Staff
Travel 1(VL 1Courier,
1Domestic 1Travel)
Orientations
Service 1Provision
Cost 1implication 1of 1HIV 1infection 1these 1are 1the 1estimated 1funds 1put 1in 1the 1programs 1for
1HIV/ 1AIDS 1to 1be 1undertaken. 1 1 1
Financial 1Support 1these 1are 1funds 1needed 1to 1be 1in 1actions 1as 1the 1programs 1for
1HIV/AIDS 1are 1been 1carried 1out 1in 1the 1health 1centers. 1When 1meetings 1are 1been 1held
1for 1such 1programs 1personnel’s 1attending 1the 1meeting 1need 1lunch, 1water 1and 1incentives
1for 1work 1motivation 1among 1others. 1 1
24
Human 1Resource 1Support 1involves 1the 1availability 1of 1people’s 1work 1force 1or 1efforts
1needed 1to 1do 1the 1work 1efficiently 1and 1render 1services 1for 1the 1implementation 1of
1HIV/AIDS 1programs 1to 1the 1general 1public. 1These 1persons 1must 1be 1well 1trained, 1orientate
1because 1they 1deal 1with 1the 1public. 1
Equipment 1Support 1focuses 1on 1availability 1of 1resources 1needed 1to 1carry 1out 1the 1programs.
1Therefore, 1such 1equipment 1include 1laboratories 1and 1drug 1supply 1amongst 1other 1resources
1needed 1in 1dealing 1with 1HIV/AIDS 1
Technical 1Support 1these 1are 1the 1health 1experts 1and 1monitors 1assigned 1to 1check 1on 1how
1the 1programs 1on 1HIV/AIDS 1are 1been 1carried 1out 1and 1evaluate 1the 1challenges 1the
1programs 1is 1facing 1as 1it 1is 1been 1executed. 1 1 1 1
Logistical 1Support 1this 1variable 1which 1looks 1at 1the 1transportation 1of 1equipment 1and 1health
1personnel’s 1in 1order 1to 1carry 1out 1the 1program 1effectively. 1
2.5 1Chapter 1summary 1 1
Based 1on 1literature 1review, 1there 1exists 1a 1gap 1on 1the 1assessment 1of 1cost 1implication 1on
1HIV/AIDS 1management. 1Some 1studies 1have 1shown 1the 1efforts 1and 1investments 1the
1government 1and 1other 1partners 1are 1investing 1in 1order 1to 1fight 1the 1HIV/AIDS. 1Therefore,
1this 1research 1study 1aimed 1at 1filling 1up 1the 1gap 1on 1HIV/AIDS 1programs 1and 1cost
1implication 1management 1because 1there 1has 1been 1an 1argument 1to 1whether 1the 1money
1invested 1is 1benefiting 1the 1people 1affected 1with 1HIV/AIDS 1or 1maybe 1it’s 1been
1mismanaged 1by 1the 1people 1in 1authorities, 1after 1the 1money 1is 1been 1invested 1by 1the
1government 1and 1other 1partner 1to 1reduce 1HIV/AIDS 1or 1maybe 1the 1funding 1is 1not 1enough
1to 1carry 1out 1the 1HIV/AIDS 1programs 1to 1the 1general 1public. 1However, 1this 1gap 1triggered
1the 1researcher 1to 1undertake 1the 1study 1to 1 1 1 1 1analyze 1the 1government 1and
1implementing 1partners 1cost 1implication 1on 1HIV/AIDS 1case 1management 1
25
CHAPTER 1THREE: 1RESEARCH 1METHODOLOGY
3.0 1Introduction
This 1chapter 1will 1looked 1at 1methodological 1procedures 1to 1be 1followed 1when 1collecting
1and 1analysing 1data. 1The 1methodological 1procedure 1includes: 1study 1design; 1study 1area;
1study 1population; 1study 1sample; 1sample 1size; 1sampling 1method; 1data 1collection; 1data
1analysis; 1data 1management 1and 1quality 1and 1ethical 1considerations.
3.1 1Study 1Design
Research 1Design 1is 1the 1framework 1that 1specifies 1the 1types 1of 1information 1to 1be 1collected,
1source 1of 1data 1and 1data 1collection 1procedures 1(Shuttle 1worth, 12008). 1Good 1design 1makes
1sure 1that 1the 1information 1gathered 1is 1consistent 1with 1the 1study 1objectives 1and 1data 1are
1collected 1by 1accurate 1and 1economical 1procedure. 1This 1research 1is 1qualitative 1and
1quantitative 1in 1nature. 1The 1study 1specifically, 1is 1more 1of 1a 1descriptive 1design 1and 1little
1mathematical 1in 1nature, 1this 1was 1used 1to 1obtain 1the 1relevant 1information 1from
1respondents. 1
3.2 1Study 1target 1population
Creswell 1(2008) 1defined 1target 1population 1as 1a 1group 1of 1individuals 1who 1have 1one 1or
1more 1characteristics 1in 1common 1which 1is 1of 1interest 1to 1the 1researcher. 1This 1study
1comprised 1of 1various 1western 1province 1implementing 1partners 1such 1as 1the 1NonGovernmental 1Organisation 1and 1the 1district 1health 1office 1accountant 1directors. 1
3.3 1Study 1sample 1size
A 1sample 1is 1a 1small 1group 1of 1respondents 1drawn 1from 1a 1population 1which 1the
1researcher 1is 1interested, 1in 1gaining 1information 1and 1drawing 1conclusions 1(Creswell, 12008).
1The 1study 1was 1comprised 1of 142 1respondents 110 1respondents 1were 1implementing 1partners
1(NGO’s) 1and 1from 1each 1organisation 1only 12 1respondents 1were 1selected 1for 1this 1study
1and 116 1respondents 1were 1from 1the 1district 1health 1office 1accountant 1directors’ 12
1respondent 1from 1each 1district 1of 1western 1province.
3.4 1Sampling 1method
Sampling 1method 1refers 1to 1the 1process 1of 1selecting 1the 1participants 1of 1the 1sample 1study
1from 1the 1population. 1Purposive 1sampling 1was 1used 1in 1this 1study 1to 1the 1district 1health
1accountant 1directors 1and 1Implementing 1Partners 1(NGO’s) 1were 1interviewed. 1The 1purposive
1sampling 1was 1employed 1for 1every 1respondent 1because 1it 1was 1specific 1on 1the 1HIV/AIDS
26
1cost 1implication 1management 1as 1it 1allowed 1the 1researcher 1to 1interact 1with 1respondents
1who 1are 1familiar 1with 1the 1study 1and 1hence 1assist 1the 1researcher 1to 1collect 1relevant
1information 1required. 1
3.5 1Data 1collection
This 1study 1employed 1triangulation 1methods. 1Denzin 1and 1Lincolin 1(2000) 1stated 1that
1triangulation 1involves 1the 1use 1of 1a 1combination 1of 1different 1methods 1of 1data 1collection.
1Experience 1shows, 1that 1no 1single 1instrument 1is 1adequate 1in 1and 1of 1itself 1in 1collecting
1valid 1and 1reliable 1data. 1The 1study 1employed 1a 1range 1of 1data 1collection 1methods 1and
1instruments, 1including 1documentary 1analysis, 1face-to-face 1interviews, 1structured
1questionnaires, 1semi 1questionnaires 1and 1group 1discussions. 1Structured 1questionnaires 1was
1used 1for 1quantitative 1data 1and 1semi 1structured 1questionnaire 1was 1used 1in 1collecting
1qualitative 1data. 1The 1questionnaires 1consisted 1of 1the 1following 1sections 1in 1accordance 1to
1the 1support 1provided 1towards 1the 1HIV 1program; 1Financial, 1Human 1Resource, 1Technical
1Support, 1Logistical 1Support 1and 1Equipment. 1These 1questions 1were 1guided 1by 1the
1researcher 1and 1assistants 1to 1the 1researcher. 1The 1collection 1of 1data 1on 1each 1Implementing
1Partner 1and 1the 1DHDs 1were 1taken 1only 120 1minutes. 1Face-to-face 1interviews 1and 1group
1discussions 1were 1also 1done 1to 1both 1target 1populations. 1
3.6 1Data 1analysis
Data 1was 1categorized 1according 1to 1the 1variables 1after 1coding 1which 1was 1entered 1into
1SPSS 1(Scientific 1Package 1for 1Social 1Scientists) 121.0 1database 1for 1analysis 1after 1it 1was
1been 1checked 1for 1internal 1completeness 1and 1accuracy. 1Quantitative 1data 1was 1analyzed
1using 1chi 1square 1test 1to 1establish 1the 1relationships 1between 1independent 1variables 1and
1dependent 1variables.
3.7 1Data 1management 1and 1quality
The 1questionnaire 1was 1pretested 1to 1a 1particular 1number 1of 1HIV 1Implementing 1Partners 1in
1order 1to 1see 1if 1the 1required 1data 1has 1come 1out. 1Then 1data 1was 1collected 1by 1data
1collectors 1from 1the 1districts 1or 1field, 1which 1was 1entered 1into 1SPSS 121.0 1version 1for
1analysis 1after 1thorough 1cleaning. 1Data 1was 1processed 1and 1stored 1on 1the 1computer, 1hard
1drive 1and 1google 1drive 1to 1avoid 1loss 1of 1the 1data. 1The 1questions 1did 1not 1bear 1any
1name 1of 1the 1interviewee 1from 1any 1district.
27
3.8 1Ethical 1consideration
The 1ethical 1considerations 1that 1were 1considered 1when 1conducting 1the 1study 1are 1as
1follows:
Ethical 1clearance 1to 1conduct 1the 1study 1came 1from 1the 1University 1of 1Lusaka 1Research
1Committee.
Permission 1to 1conduct 1study 1among 1HIV 1Implementing 1Partners 1in 1Western 1Province
1was 1obtained 1from 1Western 1Provincial 1Health 1Office. 1
The 1research 1participants 1were 1notified 1of 1their 1participation 1as 1voluntary 1and 1may
1decide 1to 1withdraw 1anytime 1during 1the 1course 1of 1the 1study 1when 1they 1feel
1uncomfortable. 1
The 1research 1participants 1were 1also 1notified 1of 1withdrawing 1from 1the 1study 1shall 1not
1affect 1them 1in 1anyway 1as 1it 1is 1only 1for 1academic 1purpose. 1
28
CHAPTER 1FOUR: 1DATA 1ANALYSIS 1AND 1INTERPRETATION
4.0 1Introduction 1 1
In 1the 1following 1chapter 1the 1main 1content 1is 1to 1present 1the 1findings 1which 1were
1obtained 1from 1the 1survey, 1interpret 1and 1discuss 1the 1findings. 1Therefore, 1this 1chapter
1present 1and 1discuss 1the 1findings 1according 1to 1the 1research 1objectives 1and 1the 1proposed
1research 1methodology. 1
4.1 1The 1benefits 1derived 1from 1the 1program 1since 1its 1establishment 1in 12012 1in
1Western 1Province 1establish 1how 1much 1investment 1has 1been 1made 1towards 1reducing
1the 1HIV/AIDS 1infections.
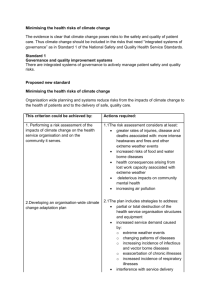
Figure 4.11: 1indicates 1the 1benefits 1from 1the 1programs 1which 1were 1established 1in 12012
1to 1prevent 1and 1reducing 1HIV/AIDS.
(Source: 1Author, 1(2021) 1
The 1data 1which 1was 1collected 1above 1shows 1the 1percentage 1of 1different 1programs 1been
established 1in 1reducing 1the 1HIV/AIDS 1infections. 1The 1bar 1graph 1indicates 1that 1CM
Circumcision 1of 1Male, 140% 1of 1the 1population 1did 1CM 1in 1the 1period 12012-2017, 1ARVs
95% 1of 1population 1in 1the 1province 1affected 1with 1HIV/AIDS 1do 1accept 1to 1be 1taking 1the
1drugs, 1anti-natal 180% 1mothers 1who 1were 1pregnant 1attend 1the 1program, 1VCT 190% 1of
1population 1did 1the 1voluntary 1counselling 1test 1and 180% 1of 1the 1population 1went 1for
1counselling 1and 1attended 1public 1meetings 1on 1HIV/AIDS 1which 1were 1conducted 1randomly.
11
29
From 1the 1first 1objective 1on 1the 1benefit 1derived 1from 1the 1programme 1since 1its
1establishment 1in 12012 1towards 1reducing 1the 1HIV/AIDS 1as 1presented 1in 1figure 12. 1The
1ARVs 1were 1the 1highest 1considered 1benefit 1of 1programs 1in 1trying 1to 1reduce 1and 1boost
1up 1the 1immune 1system 1of 1people 1who 1are 1HIV 1positive. 1Followed 1by 1Voluntary
1counselling 1and 1testing 1(VCT) 1about 190% 1of 1the 1population 1of 1western 1province 1have
1done 1it 1once 1or 1twice 1in 1their 1life 1to 1know 1their 1status. 1Anti-natal 1and 1counselling 1of
1couples 1are 1also 1some 1of 1the 1benefits 1of 1the 1programs 1which 1were 1been 1established
1since 12012. 1Male 1Circumcision 1(CM) 1is 1another 1program 1which 1was 1established 1in 1try
1to 1reduce 1HIV/AIDS. 1
Therefore, 1following 1the 1interviews 1with 1one 1of 1the 1respondent 1who 1explained 1that, 1these
1programs 1which 1were 1established 1from 12012 1and 1years 1back 1had 1benefited 1the
1government 1in 1knowing 1how 1much 1funds 1were 1needed 1in 1order 1to 1reduce 1the 1epidemic
1of 1HIV/AIDS 1and 1suggest 1the 1way 1forward 1to 1combat 1the 1epidemic. 1The 1ARV’s 1and
1VCT 1programs 1were 1the 1most 1activities 1and 1programs 1which 1were 1exercised. 1The
1programs 1for 1VCT 1are 1done 1randomly 1throughout 1the 1province 1along 1with 1distribution 1of
1condoms 1to 1the 1public 1for 1prevention 1during 1these 1VCT 1programs. 1Male 1circumcision
1(CM) 1are 1also 1done 1and 1encouraged 1in 1order 1to 1prevent 1cervical 1cancer 1and 1HIV/AIDS
1spread. 1However, 1on 1the 1other 1hand 1there 1has 1been 1job 1creation 1to 1the 1people 1of
1western 1province 1and 1Zambia 1at 1large 1because 1for 1these 1projects 1to 1be 1implemented
1and 1work 1effective 1there 1is 1need 1of 1human 1resource 1for 1example, 1personnel 1who
1operate 1on 1male 1circumcision, 1who 1do 1HIV/AIDS 1education 1teachings 1to 1the 1general
1public 1and 1personnel 1who 1work 1on 1anti-natal 1programs. 1
The 1research 1findings 1are 1similar 1to 1the 1findings 1of 1Peters, 1(2010) 1found 1that 1both 1the
1European 1the 1American 1governments 1had 1shifted 1their 1attention 1from 1treatment 1to
1prevention 1of 1HIV 1in 1their 1support. 1Leibowitz, 1(20111) 1found 1that 1treatment 1expenditures
1on 1HIV 1had 1overshadowed 1the 1prevention 1spending 1on 1HIV. 1Kates, 1(2005) 1said 1that
1Centres 1for 1Disease 1Control 1and 1Prevention 1(CDC) 1uses 1grants 1and 1cooperative
1agreements 1to 1fund 1research 1and 1non-research 1public 1health 1programs 1that 1advance 1the
1Agency’s 1public 1health 1mission. 1CDC’s 1Division 1of 1HIV/AIDS 1Prevention 1maintains 1an
1HIV 1Funding 1page 1with 1information 1on 1current 1CDC 1HIV 1prevention 1funding
1opportunities 1open 1for 1applicants 1as 1well 1as 1active 1grant 1programs 1for 1which 1awards
1have 1already 1been 1made. 1 1In 1addition, 1CDC’s 1National 1Prevention 1Information 1Network
1provides 1a 1database 1of 1HIV-related 1funding 1opportunity 1announcements 1from 1CDC 1and
30
1many 1other 1federal 1agencies, 1as 1well 1as 1funding 1opportunities 1related 1to 1viral 1hepatitis,
1STDs, 1tuberculosis, 1and 1school 1health.
Figure 4.2: 1Shows 1the 1provincial 1HIV 1spending 1in 1Zambia 1(US$m, 1%, 12015-2017)
(Source: 1 1Field, 1(2021) 1
The 1above 1figure 1indicates 1the 1provincial 1HIV 1funding 1from 12015-2017, 1of 1which 1the
1percentages 1and 1graph 1they 1are 1varying 1depending 1on 1the 1years. 1
Figure 4.3: 1shows 1the 1percentage 1of 1each 1provincial 1HIV 1grants 1which 1was 1allocated 1 1
31
(Source: 1Author, 12021) 1
From 1the 1above 1figure 1a 1lot 1of 1grants 1was 1given 1to 1Lusaka 116% 1followed 1by 1Southern
110 1%, 1Copperbelt 19 1%, 1Central 16%, 1Eastern 15%, 1Western 13 1%, 1Luapula 12%, 1North
1western 12 1%, 1Northern1.5 1% 1 1and 1Muchinga 1provinces 11 1%. 1
According 1to 1figure 13 1the 1provincial 1HIV 1spending 1in 1Zambia 1(US$ 1m, 1%, 12015-2017).
1From 1the 1data 1which 1was 1obtained 1in 1the 1field 1it 1can 1be 1analysed 1that, 1in 12015 1the
1money 1which 1was 1invested 1towards 1HIV 1reduction 1is 1approximate 1US$ 1M 135- 1US$ 1M
140 1(K880, 1000 1000) 1of 1which 1Western 1province 1had 1a 1share 1in 1order 1to 1work 1on 1the
1programs 1been 1implemented 1towards 1reducing 1of 1HIV. 1Similar 1to 1figure 14 1which 1shows
1percentages 1of 1grants 1which 1were 1allocated 1to 1each 1province, 1were 1Western 1province
1had 13% 1of 1the 1total 1money 1which 1was 1allocated 1in 1the 1years 12015-2017. 1Therefore,
1through 1the 1interviews 1with 1the 1Districts 1Accountant 1Offices 1of 1Western 1province, 1the
1accountant 1explained 1that, 1the 1grants 1which 1were 1released 1by 1the 1government 1to 1our
1province 1was 1shared 1according 1to 1the 1population 1of 1our 1district, 1therefore, 1the 1districts
1with 1large 1population 1where 1given 1good 1enough 1grants 1in 1order 1for 1the 1programs 1to 1be
1a 1success. 1
However, 1the 1majority 1of 1the 1respondents 170% 1said 1that, 1the 1money 1which 1was 1allocated
1to 1our 1district 1hospitals, 1clinics 1and 1post 1heath 1centres 1was 1used 1in 1carrying 1out 1the
1programs 1like 1HIV/AIDS 1sensation 1in 1public 1place, 1transport 1grants 1and 1allowances 1for
1the 1staffs 1involved 1and 1other 1vital 1things 1like 1hiring 1dancing 1groups 1and 1drama 1also
1hiring 1of 1sound 1systems. 1
32
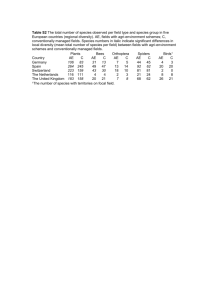
Figure 4.4: 1shows 1the 1National 1AIDS 1Spending 1Assessment 1towards 1reducing 1the
1HIV/AIDS 1infections 1in 1Zambia 1from 12012-2017. 1 1
(Source: 1 1Author, 1(2021) 1
The 1figure 14.5 1shows 1the 1National 1AIDS 1Spending 1Assessment 1towards 1reducing
1HIV/AIDS 1infections 1in 1Zambia 1from 12012-2017. 1The 1bar 1graph 1shows 1that 1in 12012
1the 1money 1which 1was 1invested 1was 1about 1US$ 1M 137, 1then 1by 12013 1the 1graph 1shows
1approximate 1US$ 1M 150(K1,100, 1000 1000) 1was 1invested, 1in 1the 1year 12014 1approximate
1US$ 1M 135 1(K770, 1000 1000) 1was 1invested 1in 1trying 1to 1reduce 1HIV/AIDS. 1While 1in
1the 1year 12015 1approximate 1US$ 1M 140, 1US$ 1M 130 1( 1K660,000 1000) 1was 1invested 1in
1the 12016 1and 1in 12017 1approximate 1US$ 1M 140. 1Therefore, 1from 1the 1investment 1towards
1HIV/AIDS 12013 1was 1the 1highest 1and 12012 1was 1the 1lowest. 1 1
The 1finding 1from 1this 1research 1is 1similar 1to 1the 1findings 1of 1 1Saleh 1et 1al 1(2018) 1who
1analysed 1that, 1the 1MHBP 1cost 1estimates 1produced 1by 1this 1study 1varied 1by 1country, 1but
1on 1average 1the 1cost 1was 1similar 1to 1what 1the 1literature 1has 1estimated 1(for 1example,
1McIntyre, 1et.al. 1(2017). 1The 1cost 1of 1the 1MHBP 1was 1on 171 1% 1persons, 1average 1$87
1per 1person 1covered 1(or 1$38 1per 1capita24) 1per 1year 1at 1baseline 1for 1the 1three 1main
1countries 1(Cote 1d´Ivoire, 1Kenya 1and 1Tanzania) 1for 12015. 1However, 1variations 1were
1observed 1across 1countries. 1The 1MHBP 1costs 1more 1in 1Cote 1d’Ivoire 1($106) 1and 1Kenya
1($98) 1than 1in 1Tanzania 1($68) 1per 1population 1covered. 1
33
4.2 1The 1best 1investment, 1need 1based 1options 1to 1be 1undertaken 1towards 1HIV 1high
1impact 1activities 1in 1Western 1Province
Figure 4.5: 1Shows 1Zambia 1HIV 1funding 1sources 12012-201-2015 1of 1which 1in 12012 1US$
1532 1million 1was 1funded, 12013 1US$ 1488 1million 1was 1invested, 12014 1US$ 1608 1m 1was
1invested 1and 1in 12015 1US$ 1533 1million 1was 1funded. 1The 1data 1presented 1in 1figure 16
1shows 1that 1the 1PEPFAR 1is 1the 1major 1investor 1in 1all 1the 1four 1years 1of 1HIV/AIDS 1cost
1management, 1followed 1by 1public 1sources. 1Global 1funding 1is 1the 1third, 1other 1bilateral
1donors 1are 1the 1four 1while 1private 1sector 1is 1fifth 1and 1other 1multilateral 1donors 1are 1the
1least. 1From 1the 1data 1above 1the 1PEPFAR 1and 1public 1sources 1are 1the 1most 1contributors
1to 1the 1programs 1of 1preventing 1and 1treating 1the 1HIV/AIDS 1epidemic. 1 1
Figure 4.6: 1Agents 1of 1HIV 1funding 1in 1Zambia 1(US$m, 12015-2017)
(Source: 1 1Author, 1(2021) 1
From 1the 1interviews 1with 1one 1of 1the 1respondents 1explained 1that, 1financial 1agents 1are 1the
1entities 1that 1manage 1and 1distribute 1funds, 1purchasing 1services 1and 1determining 1the
1interventions 1to 1be 1provided. 1The 1largest 1majority 1of 1funds 1were 1external 1and 1this 1was
1mostly 1driven 1by 1the 1USG 1funds, 1since 1the 1USG 1was 1labelled 1as 1the 1agent 1for 1its
1own 1funding. 1Much 1of 1the 1GF 1monies 1went 1through 1the 1government 1or 1NGOs, 1which
1were 1labelled 1as 1the 1agent. 1Importantly, 1the 1public 1agent 1share 1increased 1from 19% 1in
12015 1to 115% 1in 12017, 1showing 1more 1direction 1from 1government 1and, 1assumingly,
1alignment 1with 1national 1priorities.
34
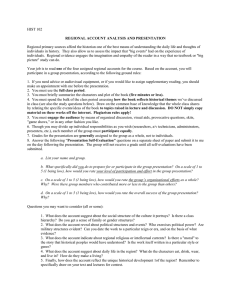
The estimates of the HIV prevalence rate in adults aged 15-49 years suggest that the Zambian HIV
epidemic has been fairly stable over the past 15 years, with a very modest decline after the initial peak
prevalence3. According to Spectrum estimates, adult HIV prevalence peaked in the early 1990s at about
15.2% and has slowly declined to just above 12.6% in 20134. Likewise, HIV incidence has declined
from 1.81% in 2000 to 0.7% in 2013. For children aged 0-14 years, HIV prevalence reached peak levels
in early 2000 and has remained fairly stable over the last ten years with a very modest decline. This
inference is drawn from the Spectrum model estimates which indicate that HIV prevalence in children
aged 0-14 years declined from 2.9% in early 2000 to around 2.32% in 20135.
Figure 5: Spectrum projection of HIV prevalence by age
Source: Spectrum Policy Modelling System: Zambia Model, March 2014
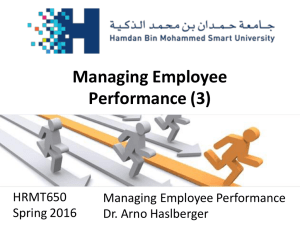
Figure 6: Projected HIV incidence trends 1990 – 2013
35
Source: Spectrum Policy Modelling System, Version 5.03_500 (2014); Zambia Model March
2014
HIV Mortality Trends
The Vital Registration System in Zambia is not optimally functional. While it is up-to-date with
registering of births, the registration of deaths is a serious challenge and gap. In the absence of
reliable mortality data from the Vital Registration System, estimates from Spectrum are used to plot
HIV-related mortality trends. The estimated mortality rate from AIDS in adults aged 15 years and
older has decreased from a peak of 8% in 2002 to 2.1% in 2013. As the ART programme is scaled
up, HIV-related mortality is expected to decline. Currently, survival and retention of people on ART
at 12 months has increased from 65% in 2010 to 81% in 2013. Similarly, mortality attributable to
AIDS in infants reduced from a peak of 10.19% in 2003 to 4.74% in 2013.
Statistical models
This study used the SAE technique to model and estimate HIV prevalence in Zambia, adapting methods
from a similar study in South Africa [6]. Note that the outcome variable entered the modeling
framework as a logit transformation of the direct district HIV prevalence from the ZAMPHIA survey.
The ANC HIV prevalence rate was also modeled as a logit transformation. The HIV prevalence rates are
the direct domain estimates of the Zambian district-level HIV prevalence proportions from the
ZAMPHIA survey, while the ANC HIV prevalence rates are the prevalence proportions among pregnant
women who obtained antenatal care services from clinics dotted across the various districts in Zambia.
The logit transformation was necessary for converting prevalence proportions to the real line which
36
helps in ascertaining the normality assumption test. Similarly, sampling error variance was estimated as
Delta-method approximation using the variances of the domain estimates as reported and elaborated
elsewhere [5]. The model estimated the true HIV prevalence by combining the direct estimate (i.e.,
direct methods estimation) from the ZAMPHIA survey and the indirect model-based estimates, based on
auxiliary predictors and the spatial correlation effects meant to improve the model prediction by
borrowing strength from across the districts [6]. The direct estimate of HIV
prevalence, \(\overline{y}_{i}\) for district i, was obtained as a weighted mean district-specific HIV
prevalence from the ZAMPHIA survey. This estimate can be viewed to be as follows:
$$\overline{y}_{i} = \Theta_{i} + \varepsilon_{i}$$
(1)
where \(\overline{y}_{i}\) is the HIV prevalence estimate for district i estimated from the survey
data; \(\Theta_{i}\) is the district’s true HIV prevalence being estimated; and εi is the random error with
mean 0 and variance \(\sigma_{i}^{2}\) and is assumed to be normally distributed.
However, since the number of respondents sampled at district level, during the ZAMPHIA, is not
sufficient to provide reliable district HIV prevalence estimates, the second part of the model, referred to
as indirect method, was estimated to improve the reliability of the estimates. Therefore, in addition to
the direct prevalence estimates obtained from ZAMPHIA, the indirect method used auxiliary
information from within the district and neighboring districts, and other data sources to borrow strength
and improve the precision of the HIV prevalence estimates [16]. Since the outcome variable was a logit
transformation of HIV prevalence, we assumed that HIV prevalence is a linear function of covariates or
HIV risk factors obtained from auxiliary data [6]. The true HIV prevalence (\(\Theta_{i}\) in Eq. 1) can
therefore be thought of as:
$$\Theta_{i} = x_{i} \beta + v_{i}$$
(2)
β is a set of regression coefficients obtained by regressing \(\overline{y}_{i}\) on HIV risk factors (xs)
and vi are normally distributed random errors with mean 0 and variance \(\sigma_{v}^{2}\). Note
that \(\sigma_{v}^{2}\) and \(\sigma_{i}^{2}\) are independent of each other. Combining
Eqs. 1 and 2 gives the following mixed-effects linear regression model;
$$\overline{y}_{i} = x_{i} \beta + v_{i} + \varepsilon_{i}$$
37
(3)
To improve precision of the HIV prevalence estimates from Eq. 3, there is need for a model that
combines direct and indirect estimates into a single estimate, such as the Fay–Herriot (FH) small-area
estimator. The FH estimator is a linear combination of a direct and synthetic estimator which reduces
estimation variance in the underrepresented small areas and in the whole model [17]. The FH estimator
is given by:
$$\overline{y}_{i} = \gamma_{i} \overline{y}_{i} + \left( {1 - \gamma_{i} } \right)x_{i} \hat{\beta
}$$
(4)
where γi and 1 − γi are weights for the direct estimate \(\overline{y}_{i}\) and the synthetic
estimate, \(x_{i} \hat{\beta }\), respectively, which constitute the FH estimator. Note that γ is simply the
ratio of the model error variance to the total error, i.e., \(\frac{{\sigma_{v}^{2} }}{{\sigma_{v}^{2} +
\sigma_{i}^{2} }}\). This means that if the survey-based estimates are precise, more weight is given to
the direct estimate. Similarly, low precision of the survey-based estimates results in more weight being
given to the synthetic or indirect estimate.
Spatial correlation
There is evidence that areas close to each other tend to have similar population dynamics, such as
disease risk factors and disease burden [18]. This highlights the importance of location and geographical
clustering in determining the spread of, and burden of disease—especially infectious diseases, for areas
that are in close proximity [19, 20]. A study in Ethiopia documented the importance of geographical
clustering in determining the prevalence of HIV and Tuberculosis (TB) [21].
To account for this spatial correlation, we built a spatial Fay–Herriot (SFH) model and tested it against a
non-spatial model to ascertain the best fitting model for this study. A spatial adjacency matrix (W) was
built in Excel, as follows:
Spatial adjacency matrix (W) is an n × n matrix where n is the number of district in Zambia.
The diagonal entries are Wii = 0, indicating no correlation for district i to itself.
38
The off-diagonal row entries add up to 1, i.e., Wij = 1. This can be thought of as follows, as presented by
Yakoi and Ando [22];
$$w_{1ij} = \left\{ {\begin{array}{*{20}c} {1/d_{ij, }^{\alpha } } \\ 0 \\ \end{array} } \right.$$
(5)
$${\mathrm{If}}\,i \ne j\,{\mathrm{otherwise}}$$
$$w_{oij} = w_{ij} /\mathop \sum \limits_{k = 1}^{N} w_{1ik}$$
(6)
where dij, in Eq. (5), is the distance between districts i and j; α is a parameter of the distance decay (α = 0
if ij do not share a border, otherwise 0 < α < 1). According to Eq. (6), the total amount of influence that
one area receives from other areas is fixed [22].
The data analysis was conducted in R [23] utilizing the SAE package built in the software [24]. Figures
were produced with the ggplot2 package [25].
Model selection
We fitted a variation of basic area-level models which differed in the inclusion of auxiliary predictors
and assumptions about the random effects. Model 1 included only the logit of ANC prevalence
proportion as an auxiliary predictor. Models 2–9 augmented model 1 with inclusion of the district-level
percentages of dependency ratio (DR), formal dwelling (Formal), high education (HE), land considered
to be urban (Urban), district population (Pop), population aged between 15 and 35 years (15–35 years),
population density (PD) and female population (Female), respectively.
Model 10 augmented model 2 with inclusion of formal dwelling. Model 11 augmented model 10 with
inclusion of higher education. Model 12 augmented model 11 with inclusion of urban prop. Model 13
augmented model 12 with inclusion of pop2010. This continued until model 15, which augmented
model 14 with the inclusion of pop density. Model 16 augmented model 15 with female population.
Model 17 was reduced from model 16 by deletion of the logit of ANC prevalence and provides the
contrast needed to assess the value of ANC prevalence. Models 18–35 relaxed the assumption of
independent model errors in models 1, 2 through to 17, respectively, with inclusion of a simultaneously
autoregressive (SAR) spatial covariance structure. Model 35 only contained the SAR covariance
39
structure without any covariates. The spatial adjacency matrix, described earlier, accounted for the SAR
covariance structure. Relative model performance was assessed using the Akaike Information Criterion
(AIC). The AIC balances model fit against model complexity; smaller values of AIC indicate relatively
better predictive ability. AIC is a dimensionless relative measure, and according to Gutreuter and
others [6], differences of 5 between models are customarily considered to be important.
District-level estimates of the burden of HIV infection were estimated from the best fitting model
(Model 19) which included the logit of ANC prevalence proportion and dependence ratio with the SAR
spatial covariance structure. This model was thereafter used, in combination with the survey-based HIV
prevalence estimates, to model the prevalence of HIV in all the 74 districts of Zambia. A table
containing information on the fitted models has been included as an appendix (See Additional file 1).
Note that there are other models that can be used to account for autocorrelation effect, such as the
conditional autoregressive (CAR) model, and its intrinsic version (intrinsic autoregressive [IAR] model),
and the decision to use SAR is because these models are equivalent and in practice produce similar
results.
Note that there are differences in the modeling approaches between our study and the comparable study
by Dwyer-Lindgren and others. Our study was based on small-area estimation process, while the DwyerLindgren study focuses on estimating the sub-national variation of HIV prevalence using within-country
variation at a 5 × 5-km resolution. Further, the paper reported use of a cross-walking model to link
disparate data sources that leveraged existing microdata and linear regression estimates. Use of k-means
clustering to generate a reduced set of locations based on the centroid of each k-means cluster helped to
generate pseudo-points which were assigned to HIV prevalence observed for the polygon as a whole.
This is different from our paper, where district-level data were obtained and not estimated or assumed.
All the estimates in our study were linked to available survey data which helped to provide associated
survey parameters.
Further, Dwyer-Lindgren et al. fitted three sub-models to the HIV survey data using generalized additive
models, boosted regression trees and lasso regression. They implemented geostatistical modeling
framework which allowed them to model HIV prevalence using a spatially and temporally explicit
generalized linear mixed effects model. Unlike in our model, their logit-transformed HIV prevalence
was modeled as a linear combination of a regional intercept, covariate effects, country random effects,
spatially and temporally correlated random effects. In our modeling framework, temporality seasonal
effect was not included even though the effect of the spatial term was done. Note also that the
40
frequentist approach was the main inference strategy for our study, while Dwyer-Lindgren et al. used
Bayesian framework with a deterministic approach. Their model used the stochastic partial differential
equation approach to approximate the continuous spatial and spatiotemporal Gaussian random fields.
We note that this was appropriate given the complexity of their dataset which would have suffered from
serious computation cost if the frequentist or the sampling-based approach was implemented.
Results
Table 1 shows the population demographics of the auxiliary predictors used to predict district HIV
prevalence. For instance, it can be seen that the population aged 15–35 years represented about 35% of
the population, although it ranged from the lowest rate of about 32% in some districts to highest of
almost 45% in other district. The median population with higher education was 3.3% (ranged from 1.2
to 16%), while the median population of HIV positive pregnant women was approximately 26%. The
females made up of 50.8% of the population.
Model diagnosis and validation
The results obtained using the SAE estimates model were consistently more precise than those obtained
from the direct estimate methodology. For instance, the relative mean standard errors (RMSE) in
Fig. 1 and the relative standard errors for the SAE are continuously lower than those from the direct
estimate model. In addition, the reduction in relative standard errors, due to SAE, was greatest in
districts which produced the least precise direct estimates. For instance, districts like Chadiza, Milenge,
Gwembe and Chavuma have relative standard errors reducing from 99.7 to 30.7%, 70.2 to 30%, 70.9 to
29.5% and 70.4 to 33.1%, respectively. Assuming, for example, that “useful” estimates are those for
which RSE ≤ 20%, then our SAE model produced useful estimates in 52 of the 74 districts for which
direct estimation failed to produce useful estimates.
Relative mean standard errors (RMSE) for the FH HIV prevalence estimates and survey-based
prevalence estimates: The RMSE show lower mean standard errors for the Fay–Herriot small-area
estimations over the survey-based estimation for all the 74 Zambian districts.
It is worth noting that the estimates from the Fay–Herriot estimator had narrower 95% confidence
intervals than the direct estimates. Conversely, some point estimates for some districts such as Chadiza
and Gwembe differed rather substantially between the design-based and model-based estimates. The
41
design-based survey domain estimate of HIV prevalence in Gwembe and Chadiza was of little value for
lack of precision, and at most misleading. Smaller relative standard errors from the FH small-area
estimates are more likely to be true, compared to those from the direct estimates, and are much more
likely to be similar to surrounding districts.
HIV prevalence estimates and confidence intervals for the FH and direct estimates in Zambia’s districts:
The confidence intervals of the FH estimates are narrower than those of the direct estimates for most of
the districts
The conclusion from this model diagnostics and validation is that the FH estimator produces smaller
standard errors compared to the survey-based estimates, across all the 74 districts of Zambia. This
means that SAE prevalence estimates are more reliable than those obtained from the direct estimates.
District HIV prevalence estimates
The district HIV prevalence in Zambia ranges from as low as 4.3% (CI 2.6–6.9) in Lundazi to as high as
23.3% (CI 19.3–27.8) in Namwala. Other notable districts with high HIV prevalence, in order of
magnitude, include Mongu (22.8%; CI 19.2–26.8), Mazabuka (18.7%; 15.4–22.5), Kalulushi (17.5%; CI
13.2–22.7), Choma (17.2%; CI 14.4–20.5), Itezhi-tezhi (17.1%; CI 11.8–24.1), Kafue (17.1%; CI 14.4–
20.1) and Lusaka (16.5%; CI 15.3–17.8). On the other hand, the five districts with the lowest HIV
prevalence, in descending order, were: Chama (5%; 3.3–7.6), Zambezi (4.9%; CI 3–8.1), Kabompo
(4.8%; CI 2.9–7.5), Mafinga (4.6%; CI 2.7–7.5) and Lundazi (4.3%; CI 2.6–6.9). The results of the SAE
reveal that 37 of the 74 districts had relatively low HIV prevalence (≤ 10%), 25 districts had relatively
moderate HIV prevalence (between 10 and 15%), 10 districts had relatively high HIV prevalence
(between 15 and 20%), while 2 districts had relatively very high HIV prevalence (between 18.1% and
23.5%). Table 2 (See Additional file 3) provides both direct and modeled HIV estimates for all the 74
districts, with confidence intervals.
11111
Table 4.11: 1indicates 1the 1best 1investment 1to 1be 1undertaken 1towards 1HIV 1high 1impact
1activities 1
42
S/N PROGRAMS 1TO 1BE 1INVESTED 1IN
PERCENTAGE
1
1
Building 1of 1more 1health 1centres
90%
2
Adequate 1medicine
78%
3
Adequate 1testing 1equipment
89%
4
Adequate 1human 1resource 1
67%
5
Others 1vital 1programs
20%
(Source: 1 1Author, 1(2021) 1
Table 4.1 1indicates 1the 1best 1investment 1to 1be 1undertaken 1towards 1HIV 1high 1impact
1activities. 1From 1the 1majority 1of 1the 1respondents 190% 1said 1that 1building 1of 1more 1health
1centres 1and 1upgrading 1of 1health 1centres 1was 1one 1of 1the 1most 1investments 1which 1are
1needed 1towards 1HIV 1high 1impact 1activities. 1Only 1a 1proportion 1of 178% 1respondents 1also
1pointed 1out 1that, 1there 1is 1need 1of 1adequate 1medicine 1in 1health 1centres 1so 1that 1most
1people 1they 1should 1be 1reduce 1transport 1and 1distance 1to 1access 1the 1medicine 1ARVs. 1
Through 1my 1dealing 1with 1the 1respondents 189% 1also 1explained 1that, 1there 1is 1need 1of
1adequate 1testing 1equipment 1and 1laboratory 1equipment 1to 1be 1used 1in 1treating 1and 1testing
1of 1HIV/AIDS 1and 1operation 1of 1male 1circumcision 1in 1health 1centres 1which 1like 1the
1equipment. 1Only 167% 1of 1the 1respondents 1said 1that, 1the 1is 1need 1to 1invest 1in 1having
1adequate 1human 1resource, 1because 1some 1of 1the 1health 1centres 1are 1lacking 1man 1power 1in
1order 1to 1carry 1out 1the 1programs 1on 1HIV/AIDS 1treatment, 1testing 1and 1campaign.
1Including 1the 1good 1infrastructural 1of 1both 1clients 1and 1staff 1houses. 1 1
The 1findings 1are 1in 1line 1with 1the 1findings 1of 1Saleh 1et 1al 1(2018) 1who 1found 1out 1that,
1the 1project 1MHBP 1and 1other 1health 1system 1costs 1separately 1using 1different 1criteria. 1For
1MHBP 1services 1they 1used 1normative 1production 1functions 1that 1included 1some 1human
1resources, 1medical 1supplies, 1transportation 1costs, 1and 1medicines, 1cost 1out 1using 1local
1input 1costs, 1as 1well 1as 1expected 1output. 1For 1services 1outside 1of 1the 1MHBP, 1they 1relied
1on 1country-specific 1knowledge 1about 1the 1costs 1of 1hospital 1services, 1public 1health 1services,
1medical 1institutes, 1and 1the 1management 1of 1the 1health 1system 1to 1project 1future 1needs 1of
1human 1resources, 1infrastructure, 1and 1other 1operating 1expenditures.
The Investment Framework
43
The investment framework takes as its starting point a human rights approach to the HIV response,
to ensure that it is universal, equitable, inclusive and fosters participation, informed consent and
accountability. The framework makes a distinction between basic programme activities that have a
direct effect on HIV risk, transmission, morbidity and mortality; the critical enablers that are crucial
to the success of HIV programmes; and, synergies with development sectors.
The implementation of the interventions and strategies outlined under this Framework are expected
to contribute to the achievement of the outcome and impact targets and have been arrived at by
considering the state of the epidemic in the country and the results of implementation efforts to the
response thus far. The selection of the interventions and strategies is prem ised on the need to
focus on high impact interventions, with special attention being paid to key populations.
Figure 11: Prioritised Interventions - Modified from the UNAIDS Investment Framework
44
3.1
High Impact Strategic Interventions
The following section presents the prioritised interventions, strategies and results for the
national response.
Treatment Care and Support
The goal of treatment, care and support is to reduce morbidity and mortality through universal
access to comprehensive HIV/TB/STI treatment, care and support services and improve the quality
of life for people living with and affected by HIV and AIDS. Treatment, care and support in the
context of HIV and AIDS encompasses a continuum of actions and interventions at various stages
including Pre-ART and ART as well as special attention to TB/HIV co-infection and nutrition and
psychosocial support. The continuum includes activities that are conducted primarily in static health
facilities combined with outreach to sites that bring services closer to people as well as home and
community based activities that support the individual patient and facilitate the work of health
workers based in health facilities. The actions act synergistically to contribute to delaying the onset
of illness following infection with HIV, slowing the progression of disease, preventing re-infection
or transmission of HIV to others
Programme Priority: The programme priority is to enrol and retain all people eligible for
ART in the treatment programme. Eligibility for ART is defined in the revised guidelines of
2013. Increased demand for ART services is anticipated as the HTC services get strengthened
with the Provider Initiated Counselling and Testing (PITC). The shift from CD4 350 to
CD4 500 as per the latest WHO guidelines will increase the demand for ART. Further
demand will come from the PMTCT and PEP programmes.
Programme indicators and targets: Effective implementation of the programme priorities
is expected to contribute to the achievement of the following outcome results:
Table 6: ART Targets
45
Indicator 1: % of HIV-positive adults who are eligible for treatment
currently receiving
antiretroviral therapy
2013:
2014
2015
2016
626, 775
631, 291
632, 472
629, 574
% Targeted
64%
70%
80%
95%
Population Target
545,222
599, 461
685,138
808, 569
Baseline
Estimated population in
need
Indicator 2: % of HIV-positive children currently receiving antiretroviral
2013:
2014
2015
2016
151, 468
146, 726
140, 142
134, 794
% Targeted
50%
64%
77%
90%
Population Target
76, 294
93, 288
107, 615
121, 315
Baseline
Estimated population in
need
46
Priority Strategies:
i.
Scale up and sustain adherence to treatment among PLHIV;
ii.
Ensure adequate skilled heath providers at all levels;
iii.
Increase the number of health facilities offering ART;
iv.
Expand ART/eMTCT services through integration;
v.
Accelerate ART access for children and adolescents;
vi.
Enhance the use of new technologies that facilitate diagnosis and clinical
monitoring of treatment;
vii.
Scale up and strengthen community-based HIV testing, community level
diagnostics and community level service delivery models;
viii.
Strengthen mobile ART services in rural areas and hard to reach areas or with
key populations such as prisoners, migrants and the disabled;
ix.
Strengthen the food and nutrition component of the ART programme;
x.
Advocate a clear policy to fully sanction ARV prescription authority for nurses;
xi.
Scale up early infant diagnosis of HIV services to all PMTCT sites and
expand routine opt-out testing in all facilities;
xii.
Strengthen monitoring systems to track linkages; and,
xiii.
Increase paediatric-focused site supportive mentorship and develop a paediatric
HIV hotline for clinical support.
47
3.3.2 TB/HIV Co-infection
Programme Priority: For TB and HIV co-infection, the programme priority is to reduce the
death rate among TB and HIV co-infected persons by providing them with treatment for
both HIV and TB.
Programme indicators and targets: Effective implementation of the programme priorities
is expected to contribute to the achievement of the following results:
Table 7: TB/HIV Co-infection Targets
Indicator 3: % of co-infected patients who were screened for TB in HIV care or
treatment setting
2013:
2014
2015
2016
778, 243
778, 017
772, 614
764, 368
% Targeted
65%
70%
80%
90%
Population Target
505, 857
544, 611
618, 091
687, 931
Baseline
Estimated population in
need
Priority Strategies:
i.
Strengthen mechanisms for coordination of collaborative TB/HIV interventions;
ii.
Strengthen interventions to reduce the burden of TB in HIV-infected persons;
iii.
Strengthen interventions to reduce the burden of HIV in TB patients;
iv.
Scale up TB/HIV control in special settings and populations; and,
v.
Strengthen TB/HIV infection prevention and control measures in health care and
community settings.
3.3.3
HIV Testing and Counselling (HTC)
48
HTC is a critical entry point to both HIV prevention and treatment. It ensures a person knows
their sero-status and is able to adapt their behaviour accordingly, by improving their
prevention behaviour and accessing appropriate treatment if needed. In the long term, Zambia
is recommending universal access to testing for HIV for adults, guided by the National HTC
Operational Plan 2014-2016.
To achieve prevention and treatment results, it is essential that HTC reaches all higher risk
and key populations, including patients attending health services and especially STI clients
and un-well children and teens. HTC services need to achieve outreach into epidemic hot
spots such as informal settlements, with services particularly strengthened in regions where
HIV prevalence is highest and where most new infections are occurring, particularly among
young people. Creating linkages between HTC and comprehensive youth friendly prevention
and treatment services for young people is needed, with appropriate messaging and
counselling tools and regional testing days including a youth focus. Reaching men and
reaching couples are both challenging and important concerns. Key populations will need
targeted interventions with appropriate messaging and prevention and treatment linkages.
49
Programme Priority: The programme priority is to address existing gaps in coverage,
uptake and quality of HTC services and linkages to care, treatment and prevention services.
TB screening will be included in the package of services offered in HTC settings.
Programme indicators and targets: Effective implementation of the programme priorities is
expected to contribute to the achievement of the following results:
Table 8: HTC Targets
Indicator 5: % of women and men aged 15-49 who received an HIV test and know
their results
2013:
2014
2015
2016
Estimated population in need 6, 811, 568
7, 036, 252
7, 261, 377
7, 484, 872
% Targeted
41%
47%
50%
55%
Population Target
2, 792, 743
3, 307, 038
3, 630, 688
4, 116, 679
Baseline
Priority Strategies:
i.
Scale up HTC and couple counselling services with all target audiences;
ii.
Strengthen the development of communication activities and materials relevant to
specific key populations and geographically hard-to-reach populations;
iii.
Strengthen and integrate HTC and other related Health services for ease access to
comprehensive service;
iv.
Strengthen the supply chain management system for HTC consumables; and,
v.
Encourage and strengthen collaboration of key players with key line Ministries
on HTC service provision.
3.3.4 Elimination of Mother to Child Transmission (eMTCT)
The MOH and MCDMCH have launched new guidelines on the diagnosis of HIV, the care of
People Living with HIV and the use of Anti-retroviral medicines for treating and preventing
HIV infections. These include new guidelines for women, their partners and children with the
objective ‘of simplifying access and the delivery of this life saving service. The emphasis on
initiating HIV treatment early as well as simplifying and harmonising treatment regimens
50
among various populations and implementing new eligibility criteria will increase coverage
of HIV positive women and also increase the number of children receiving HIV treatment,
consequently this will reduce new transmissions of HIV, improve mothers health and reduce
maternal and child health.
The national strategy is responding to findings in areas that require strengthening. In
particular, support for addressing prongs 1 and 2 and also for Option B+ roll out is required.
This places all HIV positive mothers on ART for life, safeguarding their health, present and
future pregnancies and breastfeeding babies. It acts as long-term “treatment as prevention”
with pregnancy as the entry point and will contribute significantly to keeping mothers and
children alive.
Program Priority: The programme priority is to eliminate new paediatric HIV infections
and improve the survival of children and their mothers within the context of HIV infection.
TB screening also will be introduced as part of an integrated approach for TB and HIV
control efforts in Zambia.
51
Program indicators and targets: Effective implementation of the programme priorities is
expected to contribute to the achievement of the following results:
Table 9: eMTCT Targets
Indicator 6: % of HIV-positive pregnant women who receive antiretroviral to
reduce the risk of mother-to-child transmission
2013:
2014
2015
2016
78, 095
76, 984
75, 576
73, 855
% Targeted
81%
86%
90%
95%
Population Target
63, 257
65, 950
68, 270
70, 162
Baseline
Estimated population in
need
Indicator 7: % of children born with HIV from mothers living with HIV
2013:
2014
2015
2016
11, 717
9, 820
7, 414
8, 430
% Targeted
8%
5%
2%
2%
Population Target
937
491
148
169
Baseline
Estimated population in
need
Priority Strategies:
i.
Reduction of new paediatric infections by 90%;
ii.
Reduction of HIV related maternal deaths by 50%;
iii.
Reduction of MTCT to less than 5% by 18 months;
iv.
Roll out lifelong ART (Option B+) to reach all eMTCT sites in the country;
v.
Scale up and strengthen male involvement in eMTCT programmes;
vi.
Scale up HIV treatment and prevention into ANC, intrapartum and postnatal
care;
vii.
Strengthen HIV treatment and prevention services;
viii.
Improve and promote the use of ANC infrastructure and facilities; and,
ix.
Expand and strengthen SRHS for adolescents and women.
52
3.3.5 Voluntary Medical Male Circumcision (VMMC)
The NASF promotes VMMC for all Zambian males targeting men aged 15 - 49 years as part
of its strategy to reduce new incidence of HIV. This strategy offers, and will continue to
offer, facility-based and community-based VMMC services as part of a comprehensive HIV
prevention package which includes: HIV Testing and Counselling (HTC); condom
programming; screening and treatment of STIs; and, referrals for HIV positive clients.
Programme Priority: The programme priority is to scale up VMMC of males across all
provinces and districts. HTC and TB screening will be offered using the VMMC settings
as entry points in alignment with the integrated approach for TB and HIV control in
Zambia.
53
Programme indicators and targets: Effective implementation of the programme priorities is
expected to contribute to the achievement of the following results:
Table 10: VMMC Targets
Indicator 8: Achieve 80% VMMC coverage among HIV negative men aged 15-49
years by
2017
2013:
2015
2016
526, 818
868, 538
126, 463
21%
29%
55%
57%
116, 265
152, 777
447, 696
72, 084
Baseline
2014
553, 643
% Targeted
Population Target
Estimated population
in
need
Source: VMMC Strategic Plan
After an initial catch-up period to 2015, annual targets will drop to anticipate normal levels.
Priority Strategies:
i)
Standardise the provision of VMMC in both public and private facilities to reflect
WHO guidelines;
ii)
Enhance knowledge and understanding of VMMC;
iii)
Scale up VMMC sites; and
iv)
Explore cost-effective methods of providing mobile VMMC.
3.3.6 Condom Programming
Condom promotion and distribution is one of the key intervention areas for the national
HIV response as part of its commitment to reducing new infections. This intervention area
will build on the successes of the current NASF 2011–2015 which promoted an increase in
distribution of both male and female condoms and in the intensification of education and
awareness-raising. The priority was wide-scale information sharing about the benefits of
54
using condoms and their correct use every time a person has casual sex or has multiple
concurrent sexual partners. The NASF also promoted the condom as a family planning
method and for use in stable relationships among sero-discordant couples. Based on evidence
and programme experience, there are significant disparities in access and condom use among
sexually active age groups. The condom use has been relatively low amongst the age group
15 – 24 years and sex workers. This highlights an important challenge that requires
improving condom programming to reach these population groups.
Programme Priority: The programme priority is to contribute to the prevention of new HIV
infections by scaling up the demand and supply of male and female condoms and lubricants in
order to increase the percentage of men and women who use condoms and lubricants
consistently and correctly during sexual intercourse.
55
Programme indicators and targets: Effective implementation of the programme priorities is
expected to contribute to the achievement of the following results:
Table 11: Condom Programming Targets
Indicator 9: Number of condoms distributed
2013:
2014
2015
2016
Baseline
Target (male condoms)
34, 057,840
41, 000, 000
58,500,000 82,000,000
Target (female condoms)
168,323
1,000,000
1,500,000
2,000,000
Indicator 10: % of men aged 15 - 49 reporting the use of a condom with their
sexual partner in the
last 12 months
2013:
2014
2015
2016
Estimated population in need 1,484,992
1,527,992
1,575,208
1,622,308
% Targeted
43%
43%
43%
44%
Population Target
640,032
657,037
677,339
713,815
Baseline
Indicator 11:
% of women aged 15 - 49 reporting the use of a condom with their sexual
partner in the last 12 months
% of sex workers reporting use of condom with their sexual partners in the
last 12 months
2013:
2014
2015
2016
Estimated population in need 1, 505, 166
1, 549, 611
1, 598, 328
1,646,595
% Targeted
42%
42%
42%
43%
Population Target
624,644
650,837
671,298
708,036
Baseline
Priority Strategies:
i.
Expand access, demand and use of condoms among the sexually active population;
ii.
Improve availability of evidence and use in condom programming;
iii.
Collaborate with Ministry of Education (MoE) on access to condoms, information,
education and communication to learners; and,
56
iv.
Ensure consistent supply and availability of condoms to end users.
3.3.7 Social and Behaviour Change
Social and behaviour change (SBC) aims to promote sustained positive behaviours with high
to low risk communities. SBC uses a variety of methods such as one-to-one talks; group
discussions; community dialogues; individual and group counselling; advocacy; drama; and,
mass media such as radio, television and print materials. In recent times, new technologies
such as Internet, texting and social media (Facebook, Twitter) have been successfully used for
SBC.
Programme Priority: The priority for the SBC programme is to influence social and
behaviour change among the general and key and vulnerable populations, with the aim of
changing social norms and creating demand and adherence for prevention interventions and
for treatment uptake.
57
Programme indicators and targets: Effective implementation of the programme
priorities is expected to contribute to the achievement of the following results:
Table 12: SBC Targets
Indicator 12: % of men aged 15-24 who had sexual intercourse before age 15
2013:
2014
2015
2016
Estimated population in need 1,484,992
1,527,992
1,575,208
1,622,308
% Targeted
16%
16%
30%
30%
Population Target
237,599
244,479
472, 562
486, 692
Baseline
Indicator 13: % of women aged 15-24 who had sexual intercourse before age 15
2013:
2014
2015
2016
Estimated population in need 1,505,166
1,549,611
1,598,328
1,646,595
% Targeted
14%
14%
30%
30%
Population Target
210,723
216,945
479, 498
493, 978
Baseline
Indicator 14: % of men aged 15-49 who had sexual intercourse with more than
one partner in the
last 12 months
2013:
2014
2015
2016
Estimated population in need 3,382,806
3,493,412
3,604,238
3,714,631
% Targeted
20%
20%
19%
19%
Population Target
666,413
698,682
684,805
705,779
Baseline
Indicator 15: Percentage of women aged 15-49 who had sexual intercourse with
more than one
partner in the last 12 months
2013:
2014
2015
2016
Estimated population in need 3,428,762
3,542,839
3,657,139
3,770,240
Percentage Targeted
2%
2%
2%
1%
Population Target
54,860
70,856
73,142
37,702
Baseline
1
Priority Strategies:
i.
Strengthen and integrate SBC into high-impact interventions;
ii.
Scale up workplace SBC innovations;
iii.
Strengthening the development of policies and guideline documents
for SBC around health seeking behaviours;
iv.
Advocate with key stakeholders for change of policies and discriminatory laws;
v.
Comprehensive sexuality education and information;
vi.
Scale up SBC in health, public and private sectors to improve
low levels of comprehensive knowledge of HIV; and,
vii.
Design appropriate SBC approaches and IEC materials for key
populations and vulnerable groups.
4.3 1The 1preparedness 1of 1the 1government 1in 1taking 1up 1the 1HIV 1program 1in
1Western 1Province
Table 4.2: 1Goal: 1To 1reduce 1the 1incidence 1and 1prevalence 1of 1HIV
Objectives
To 1ensure 1that 190% 1of
Strategies
1the
population 1know 1their
Encourage 1and 1promote 1universal 1HIV
1testing 1and 1counselling 1
1status
Targeted 1provider-initiated 1HIV 1testing 1and
1counselling 1across 1services 1such 1as 1EPI,
1ANC,
1VMMC, 1family 1planning 1(FP), 1in-patient,
1out-patient, 1TB, 1STI
1Improve 1logistics 1and 1supply 1chain
1management 1for 1HIV 1testing 1reagents 1and
1other 1laboratory 1consumables 1and 1supplies
2
To 1ensure 1that 190% 1of
1people 1living 1with 1HIV
1receive 1lifelong 1ART
100% 1of 1identified 1HIV 1positive 1people
1are 1linked 1to 1care 1and 1treatment 1services.
1Implementation 1and 1scaling 1up 1of 1test
1and 1start
90% 1of 1people 1living 1with 1HIV 1on 1ART
1are 1retained 1in 1care 112 1months 1after
1initiation
1Intensify 1identification 1and 1ART 1initiation
1for 1HIV 1positive 1children 1
Early 1diagnosis 1and 1treatment 1of
1opportunistic 1infections
1Enhance 1implementation 1of 1the 1three 1is
1and 1TB/HIV 1collaborative 1services.
To 1ensure 1that 190% 1of
people 1living 1with 1HIV
Improve 1supply 1chain 1management 1for
1laboratory 1consumables 1
1on
Use 1of 1point 1of 1care 1machines 1
ART 1have 1suppressed
Enhanced 1follow-up 1and 1adherence
1viral
1counselling
Loads
(Source: 1 1Author, 1(2021) 1
Table 4.2 1illustrates 1the 1goal 1to 1reduce 1the 1incidence 1and 1prevalence 1of 1HIV 1to
1make 1sure 1that 190% 1of 1population 1knows 1their 1status. 1The 1following 1strategies
1can 1be 1followed; 1Encourage 1and 1promote 1universal 1HIV 1testing 1and
1counselling, 1targeted 1provider-initiated 1HIV 1testing 1and 1counselling 1across
1services 1such 1as 1EPI, 1ANC, 1VMMC, 1family 1planning 1(FP), 1in-patient, 1outpatient, 1TB, 1STI 1and 1improve 1logistics 1and 1supply 1chain 1management 1for 1HIV
1testing 1reagents 1and 1other 1laboratory 1consumables 1and 1supplies. 1
To 1ensure 1that 190% 1of 1people 1living 1with 1HIV 1receive 1lifelong 1ART 1strategies;
1100% 1of 1identified 1HIV 1positive 1people 1are 1linked 1to 1care 1and 1treatment
1services, 1implementation 1and 1scaling 1up 1of 1test 1and 1start, 190% 1of 1people
1living 1with 1HIV 1on 1ART 1are 1retained 1in 1care 112 1months 1after 1initiation,
1intensify 1identification 1and 1ART 1initiation 1for 1HIV 1positive 1children, 1early
3
1diagnosis 1and 1treatment 1of 1opportunistic 1infections 1and 1enhance 1implementation
1of 1the 1three 1is 1and 1TB/HIV 1collaborative 1services.
To 1ensure 1that 190% 1of 1people 1living 1with 1HIV 1on 1ART 1have 1suppressed 1viral
1loads 1strategies; 1improve 1supply 1chain 1management 1for 1laboratory 1consumables,
1use 1of 1point 1of 1care 1machines 1and 1enhanced 1follow-up 1and 1adherence
1counselling. 1
Figure 5.2: 1shows 1the 1general 1programs 1which 1were 1done 1by 1the 1government
1
(Source: 1Author, 12021)
Figure 18 1indicates 1the 1general 1programs 1which 1were 1done 1by 1the 1government,
1therefore, 1from 1the 1graph 1it 1shows 1that 1in 1the 1year 12016 1$604 1m 1was
1invested, 12017 1$669m 1was 1invested, 12018 1$748m, 12019 1$863m 1and 12020 1$1,
1068m. 1The 1funds 1for 1this 1HIV/AIDS 1management 1cost 1programs 1were 1coming
1from 1various 1partners 1and 1the 1Zambian 1budget 1as 1illustrated 1in 1figure 16 1on
1the 1Zambia 1HIV 1funding 1sources 12012-2015. 1This 1shows 1that 1the 1government
1was 1ready 1to 1take 1up 1HIV 1programs 1in 1Western 1province. 1The 1Government 1of
1Zambia, 1the 1cooperating 1partners, 1the 1private 1and 1business 1communities 1will
1significantly 1meet 1the 1cost 1of 1implementing 1this 1plan. 1Implementation 1of 1this
1programme 1is 1going 1to 1cost 1approximately 1US$ 1348.8 1million. 1With 1the
1continuing 1decline 1in 1the 1price 1of 1ARV 1drugs 1and 1diagnostics 1it 1is 1expected
1that 1the 1unit 1cost 1of 1treatment 1will 1reduce 1over 1a 1period 1of 1time. 1
4
An 1estimation 1of 1the 1HIV 1resources 1needed 1to 1achieve 1the 1NASF 1goals,
1adjusted 1for 1the 1‘test 1and 1treat’ 1strategy 1that 1these 1needs 1continue 1to 1increase
1and 1if 1Zambia 1is 1to 1attain 1its 1goals, 1a 1potential 1funding 1gap 1could 1be
1experienced. 1 1Importantly, 1in 1the 1longer-term 1projections 1(e.g. 1EQUIP, 12017:
1T&T 1cost 1estimates 1to 12030), 1revealed 1that 1the 1costs 1will 1eventually 1begin 1to
1plateau 1around 12025, 1due 1to 1the 1impact 1of 1both 1the 1prevention 1efforts 1as 1well
1as 1the 1preventative 1effect 1of 1the 1scale-up 1of 1test 1and 1treat 1(NAC, 12017).
CHAPTER 1FIVE: 1CONCLUSION 1AND 1RECOMMENDATIONS
5.0 1Introduction 1
This 1chapter 1is 1organized 1into 1three 1major 1sections. 1Section 15.1 1provides 1the
1overall 1conclusion 1to 1the 1study. 1Section 15.2 1highlights 1the 1recommendations 1and
1last 15.3 1suggest 1future 1proposed 1topics 1to 1be 1undertaken. 1However, 1this 1survey,
1focused 1on 1the 1following 1research 1objectives; 1To 1assess 1benefits 1derived 1from
1the 1program 1since 1its 1establishment 1in 12012 1in 1Western 1Province 1establish 1how
1much 1investment 1has 1been 1made 1towards 1reducing 1the 1HIV/AIDS 1infections, 1to
1establish 1the 1best 1investment, 1need 1based 1options 1to 1be 1undertaken 1towards
1HIV 1high 1impact 1activities 1in 1Western 1Province 1and 1to 1determine 1the
1preparedness 1of 1the 1government 1in 1taking 1up 1the 1HIV 1program 1in 1Western
1Province
5.1 1Conclusion 1
The 1research 1above 1was 1to 1analyse 1the 1government 1and 1implementing 1partners
1cost 1implication 1on 1HIV/AIDS 1case 1management 1from 12012 1- 12017: 1a 1case 1of
1Western 1Province, 1Zambia. 1While 1the 1specific 1objectives 1were; 1to 1assess
1benefits 1derived 1from 1the 1program 1since 1its 1establishment 1in 12012 1in 1Western
1Province 1establish 1how 1much 1investment 1has 1been 1made 1towards 1reducing 1the
1HIV/AIDS 1infections, 1to 1establish 1the 1best 1investment, 1need 1based 1options 1to
1be 1undertaken 1towards 1HIV 1high 1impact 1activities 1in 1Western 1Province 1and 1to
5
1determine 1the 1preparedness 1of 1the 1government 1in 1taking 1up 1the 1HIV 1program
1in 1Western 1Province. 1
Therefore, 1 1with 1support 1from 1UNAIDS 1and 1AIDS 1council 1has 1led 1this
1important 1HIV 1and 1investing 1and 1spending 1assessment 1(NASA) 1 1and 1it 1is
1envisaged 1that 1the 1findings 1shall 1inform 1policy 1choices, 1improve 1implementation
1of 1the 1NASF 1priority 1services, 1and 1identify 1potential 1allocative 1and 1technical
1efficiency 1gains. 1In 1the 1context 1of 1declining 1external 1funding, 1the 1extent 1of
1dependency 1of 1the 1Zambian 1HIV 1response 1on 1these 1funds 1is 1alarming 1and
1points 1to 1a 1looming 1sustainability 1crisis, 1if 1the 1government 1cannot 1mobilize
1increased 1funding 1and 1make 1more 1efficient 1use 1of 1available 1funds. 1The 1gains
1made 1in 1the 1country 1towards 1epidemic 1control 1maybe 1seriously 1jeopardised. 1The
1assessment 1faced 1some 1challenges 1with 1data, 1and 1these 1highlight 1the 1need 1for
1continual 1efforts 1to 1improve 1all 1actors’ 1coding 1and 1reporting 1of 1their 1HIV
1expenditures. 1
5.2 1Recommendations 1
The 1study 1recommended 1that;
5.2.1 Zambia 1should 1develop 1a 1health 1and 1HIV/AIDS 1(combined) 1financing
1strategy 1
5.2.2 Zambia 1should 1be 1assisted 1in 1finding 1options 1and 1lessons 1from 1other
1countries 1exposed 1to 1similar 1situations.
5.2.3 Zambia 1should 1consider 1establishing 1trust 1funds, 1besides 1the 1already
1established 1health 1insurance 1programs.
5.2.4 Low 1rates 1of 1insurance 1coverage 1pose 1a 1challenge 1to 1the 1long-run
1sustainability 1and 1equity 1of 1access 1to 1HIV 1and 1health 1services 1in 1the
1face 1of 1declining 1donor 1resources. 1
5.3 1Future 1research 1
This 1study 1was 1on 1the 1analysing 1the 1government 1and 1implementing 1partners
1cost 1implication 1on 1HIV/AIDS 1case 1management 1from 12012 1- 12017: 1a 1case 1of
6
1Western 1Province, 1Zambia. 1The 1study 1covered 1only 1Western 1province. 1Another
1study 1should 1be 1done 1on 1financial 1sustainability 1of 1the 1governments 1and
1implementation 1partners 1on 1cost 1implication 1on 1HIV/AIDS 1management 1from
12012-2020. 1The 1proposed 1future 1topic 1should 1be 1under 1taken 1in 1order 1if 1the
1grants 1invested 1in 1HIV 1/AIDS 1has 1effectively 1reached 1its 1intended 1objectives,
1in 1order 1to 1reduce 1the 1financial 1burden 1for 1the 1future 1expenditures. 1
7
REFERENCES
Ajzen, 1I., 11991. 1The 1theory 1of 1planned 1behavior. 1Organizational 1behavior 1and
1human 1decision 1processes, 150(2), 1pp.179-211.
Atum,S 1B 1(2016) 1Health 1Benefit 1Plans 1in 1Latin 1America. 1Washington, 1DC,
1Inter-American
Development 1Bank.
Akpo 1(2002). 1Participatory 1Communication 1Strategy 1Design. 1SADC/ 1FAO 1Harare,
1Zimbabwe.
Banigbe, 1B., 1Audet, 1C.M., 1Okonkwo, 1P., 1Arije, 1O.O., 1Bassi, 1E., 1Clouse, 1K.,
1Simmons, 1M., 1Aliyu, 1M.H., 1Freedberg, 1K.A. 1and 1Ahonkhai, 1A.A., 1(2019) 1Effect
1of 1PEPFAR 1funding 1policy 1change 1on 1HIV 1service 1delivery 1in 1a 1large 1HIV
1care 1and 1treatment 1network 1in 1Nigeria. 1PloS 1one, 114(9).
Board, 1P.S.A., 1Plans, 1C.O. 1and 1Partnerships, 1P.P., 1(2003) 1The 1United 1States
1President's 1Emergency 1Plan 1for 1AIDS 1Relief.
Cailhol, 1J., 1Craveiro, 1I., 1Madede, 1T., 1Makoa, 1E., 1Mathole, 1T., 1Parsons, 1A.N.,
1Van 1Leemput, 1L., 1Biesma, 1R., 1Brugha, 1R., 1Chilundo, 1B. 1and 1Lehmann, 1U.,
1(2013) 1Analysis 1of 1human 1resources 1for 1health 1strategies 1and 1policies 1in 15
1countries 1in 1Sub-Saharan 1Africa, 1in 1response 1to 1GFATM 1and 1PEPFAR-funded
1HIV-activities. 1Globalization 1and 1health, 19(1), 1p.52.
Cotlear, 1BV, 1McIntyre, 1D., 1F. 1Meheus, 1J-A 1Rottingen 1 1et 1al 1(2012.) 1Strategies
1towards 1universal 1coverage 1in 1Rwanda: 1lessons 1learned 1through 1mutual 1health
1organizations. 1UNICO 1Series, 1The 1World 1Bank, 1Washington, 1DC. 1 1
Creswell, 1M 1(2008) 1Research 1Methodology. 1Methods 1and 1technique 1(2nd 1Ed),
1New 1Delhi: 1New 1Age 1International 1Limited.
Denzin, 1K 1and 1Lincolin, 1S 1(2000) 1, 1Research 1Methods 14th 1Edition, 1Newyork:
1mcGraw-hill 1 1
DHIS, 12019. 1Progress 1Reports 12005, 1Mongu: 1Western 1Provincial 1Health 1Office.
Kates, 1J. 1and 1Leggoe, 1A.W., 1(2005). 1US 1federal 1funding 1for 1HIV/AIDS: 1the 1FY
12006 1budget 1request. 1Washington 1D.C
8
Katz, 1I.T., 1Bassett, 1I.V. 1and 1Wright, 1A.A., 12013. 1PEPFAR 1in 1transition—
implications 1for 1HIV 1care 1in 1South 1Africa. 1New 1England 1Journal 1of 1Medicine,
1369(15), 1pp.1385-1387.
Lawn, 1S.D., 1Harries, 1A.D. 1and 1Wood, 1R., 12010. 1Strategies 1to 1reduce 1early
1morbidity 1and 1mortality 1in 1adults 1receiving 1antiretroviral 1therapy 1in 1resourcelimited 1settings. 1Current 1Opinion 1in 1HIV 1and 1AIDS, 15(1), 1p.18.
Leibowitz, 1A.A., 1Mendes, 1A.C. 1and 1Desmond, 1K., 12011. 1Public 1funding 1of
1HIV/AIDS 1prevention, 1treatment 1and 1support 1in 1California. 1Journal 1of 1acquired
1immune 1deficiency 1syndromes 1(1999), 158(1), 1p.e11.
1MOH, 1(2018). 1Zambia 1Population-based 1HIV 1Impact 1Assessment 1(ZAMPHIA)
12018
MOH, 1(2018) 1Consolidated 1Guidelines 1of 1the 1Management 1of 1HIV 1in 1Zambia.
1Lusaka: 1Ministry 1of 1Health.
NAC 1(2017). 12017. 1National 1AIDS 1Strategic 1Framework 12017 1– 12021. 1Lusaka
Odekunle, 1F.F. 1and 1Odekunle, 1R.O., 1(2016) 1The 1impact 1of 1the 1US 1president’s
1emergency 1plan 1for 1AIDS 1relief 1(PEPFAR) 1HIV 1and 1AIDS 1program 1on 1the
1Nigerian 1health 1system. 1The 1Pan 1African 1medical 1journal, 125.
Peters, 1A.J., 1Scharf, 1M.M., 1van 1Driel, 1F.T. 1and 1Jansen, 1W.H., 12010. 1Where
1does 1public 1funding 1for 1HIV 1prevention 1go 1to? 1The 1case 1of 1condoms 1versus
1microbicides 1and 1vaccines. 1Globalization 1and 1health, 16(1), 1p.23.
Saleh 1K, 1Bitran 1R, 1Couttolenc, 1B 1(2018) 1 1A 1Synthesis 1Report 1The 1Financial
1Sustainability 1Of 1HIV/AIDS 1and 1Universal 1Health 1Coverage 1Programs 1in 1SubSaharan 1Africa: 1Case 1Studies 1From 1Cote 1D´Ivoire, 1Kenya, 1Tanzania, 1And
1Nasarawa 1State 1In 1Nigeria 12018, 1AUS0000397-REVISED-HIV-Financing-studyfinal-June28-2018.pdf 1
Shuttle 1worth, 1(2008) 1Case 1Study 1Regarding 1Design 1and 1Methodology, 1Second
1Edition: 1 1Sage 1publication.
UNAIDS 1(2014) 1An 1ambitious 1treatment 1target 1to 1help 1end 1the 1AIDS 1epidemic.
1Geneva: 1UNAIDS. 1
9
UNAIDS, 1(2019) 1Trend 1of 1HIV 1New 1Infections. 1[Online] 1 1Available 1at:
1http://aidsinfo.unaids.org/ 1[Accessed 129th 1August 12019].
WHO 12019. 1HIV/AIDS 1Key 1Facts. 1World 1Health 1Organisation, 1Geneva.
Wimmer, 1M 1and 1Dominick, 1B 1(2003) 1Proposal 1and 1Thesis 1Writing 1An
1Introduction, 1Nairobi: 1Pauline 1Publications 1Africa
WPHO, 1(2019). 1Mid-Term 1Expenditure 1framework 12019 1- 12022. 1Mongu: 1Ministry
1of 1Health 1- 1Western 1Provincial 1Health 1Office.
ZAMPHIA, 12018. 1ZAMBIA 1POPULATION-BASED 1HIV 1IMPACT 1ASSESSMENT
1ZAMPHIA 12015–2016.
[Online] 1Available
1at:https://phia.icap.columbia.edu/wpcontent/uploads/2016/09/ZAMBIA-Factsheet.FIN_.pdf
1[Accessed 129th 1August 12019].
10
Appendix 11: 1 1Questionnaire 1District 1Health 1Office
QUESTIONNAIRE: 1 1FOR 1DISTRICT 1HEALTH 1OFFICE
Dear 1Respondent, 1
My 1name 1is 1Lucky 1Museta 1I 1am 1a 1student 1from 1University 1of 1Lusaka
1conducting 1a 1research 1on 1the 1analysis 1of 1the 1government 1and 1implementing
1partners 1cost 1implication 1on 1HIV/AIDS 1case 1management 1infections 1from 12012
1- 12017: 1a 1case 1of 1western 1province, 1as 1part 1of 1my 1dissertation 1leading 1to 1the
1award 1of 1Bachelor`s 1Degree 1in 1Business 1Economics 1and 1Management 1Studies. 1I
1would 1therefore, 1be 1grateful 1for 1your 1assistance 1in 1completing 1the 1following
1questions 1to 1the 1best 1of 1your 1knowledge. 1The 1responses 1that 1you 1will 1provide
1in 1this 1research 1will 1be 1treated 1with 1confidentiality 1and 1only 1meant 1for
1academic 1purposes. 1 1
Instruction 1
Please 1TICK 1your 1response 1(√)
Background 1information
1.
Age: 1a) 120 1– 125 1 1years 1□b) 126 1- 130 1years 1□c)30 1– 140 1years 1□d)
1Above 150 1years□
11
2. Sex 1: 1a) 1Male 1□b) 1Female 1□ 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1
1111111111111111111111111111111111111111111111
1111111111111111111111111111111111111111111111
111111111111111
Marital 1status: 1a) 1Single 1□b) 1Married 1□others 1□ 1 1 1 1 1 1 1 1 1 1 1 1 1
Section 1B: 1Benefits 1derived 1from 1the 1program 1since 1its 1establishment 1in 12012
1in 1Western 1Province 1establish 1how 1much 1investment 1has 1been 1made 1towards
1reducing 1the 1HIV/AIDS 1infections
3. Does 1your 1institution 1receive 1funds 1to 1carry 1out 1HIV/ 1AIDS 1program?
Yes 1□ 1 1 1 1 1 1No 1□ 1
4. If 1yes 1to 1question 14 1above 1list 1the 1HIV/AIDS 1programs 1been 1conducted
1in 1your 1health 1facilities 1in 1your 1district.
i.
………………………………………………
ii.
……………………………………………..
iii.
…………………………………………
iv.
…………………………………………. 1
5. Which 1of 1the 1HIV/AIDS 1programs 1has 1much 1fund 1been 1invested 1in. 1
Write 1your 1answer 1in 1the 1space 1provided 1A=very 1much 1B 1= 1much
1C=not 1much
S/N HIV/AIDS 1PROGRAMS 1
RESPONSE 1
(answer 1your 1choice)
1
ARVs 1drug
2
VCT
3
Male 1Circumcision
4
Anti-natal
5
Sensitisation 1on 1HIV/ 1AIDS 1and 1other
1items
12
Section 1C: 1The 1best 1investment, 1need 1based 1options 1to 1be 1undertaken 1towards
1HIV 1high 1impact 1activities 1in 1Western 1Province
6. Do 1you 1have 1other 1external 1organisations 1which 1help 1in 1carrying 1out 1the
1HIV/AIDS 1programs 1
Yes 1 1 1 1□ 1 1 1 1 1No 1 1 1 1 1□
7. Do 1these 1external 1organisations 1(NGO’s) 1give 1you 1funds 1to 1promote 1the
1HIV/AIDS 1programs 1apart 1from 1the 1government 1funds? 1
Yes 1 1 1□ 1 1 1 1 1 1No 1 1 1□ 1
8. If 1yes 1in 1question 17 1list 1the 1organisation 1that 1have 1invested 1in 1HIV
1activities 1in 1your 1district
i.
……………………………………..
ii.
…………………………………………
iii.
…………………………………………
iv.
……………………………………….. 1 1
Section 1D: 1The 1preparedness 1of 1the 1government 1in 1taking 1up 1the 1HIV
1program 1in 1Western 1Province
9. Does 1the 1government 1provide 1enough 1resource 1for 1the 1HIV/IDS 1programs
Yes 1□ 1 1 1 1No 1□
10. Do 1your 1health 1facilities 1in 1the 1district 1carrying 1out 1the 1HIV/AIDS
1programs
Yes 1□ 1No 1□
11. What 1type 1of 1services 1do 1your 1health 1facilities 1offering 1in 1the 1district
1towards 1HIV/AIDS
1programs?.........................................................................................
………………………………………………………………………………….
THANK 1YOU 1FOR 1YOU 1TIME
13
Appendix 12: 1 1Interview 1guide 1for 1District 1Health 1Office
INTERVIEW 1GUIDE: 1FOR 1DISTRICT 1HEALTH 1OFFICE
Researcher 1introduction 1
My 1name 1is 1Lucky 1Museta 1I 1am 1a 1student 1from 1University 1of 1Lusaka
1conducting 1a 1research 1on 1the 1analysis 1of 1the 1government 1and 1implementing
1partners 1cost 1implication 1on 1HIV/AIDS 1case 1management 1infections 1from 12012
1- 12017: 1a 1case 1of 1western 1province, 1as 1part 1of 1my 1dissertation 1leading 1to 1the
1award 1of 1Bachelor`s 1Degree 1in 1Business 1Economics 1and 1Management 1Studies. 1I
1would 1therefore, 1be 1grateful 1for 1your 1assistance 1in 1completing 1the 1following
1questions 1to 1the 1best 1of 1your 1knowledge. 1The 1responses 1that 1you 1will 1provide
1in 1this 1research 1will 1be 1treated 1with 1confidentiality 1and 1only 1meant 1for
1academic 1purposes. 1 1
Background 1information
14
1. Age: 1
2. Marital 1status: 1
Item 1or 1questions 1to 1be 1asked 1to 1respondents 1in 1an 1interview 1
Section 1B: 1Benefits 1derived 1from 1the 1program 1since 1its 1establishment 1in 12012
1in 1Western 1Province 1establish 1how 1much 1investment 1has 1been 1made 1towards
1reducing 1the 1HIV/AIDS 1infections
3. Does 1your 1institution 1receive 1funds 1to 1carry 1out 1HIV/ 1AIDS 1program?
4. 1How 1are 1the 1funds 1been 1invested? 1list 1the 1HIV/AIDS 1programs 1been
1conducted 1in 1your 1health 1facilities 1in 1your 1district.
5. Which 1of 1the 1HIV/AIDS 1programs 1has 1much 1fund 1been 1invested 1in. 1
Section 1C: 1The 1best 1investment, 1need 1based 1options 1to 1be 1undertaken 1towards
1HIV 1high 1impact 1activities 1in 1Western 1Province
6. The 1other 1external 1organisations 1which 1help 1in 1carrying 1out 1the 1HIV/AIDS
1programs 1
7. External 1organisations 1(NGO’s) 1give 1you 1funds 1to 1promote 1the 1HIV/AIDS
1programs 1apart 1from 1the 1government 1funds? 1
8. Names 1the 1organisation 1that 1have 1invested 1in 1HIV 1activities 1in 1your 1district
Section 1D: 1The 1preparedness 1of 1the 1government 1in 1taking 1up 1the 1HIV
1program 1in 1Western 1Province
9. The 1government 1provide 1enough 1resource 1for 1the 1HIV/IDS 1programs
10. The 1health 1facilities 1in 1the 1district 1carrying 1out 1the 1HIV/AIDS 1programs
11. Type 1of 1services 1do 1your 1health 1facilities 1offering 1in 1the 1district 1towards
1HIV/AIDS 1programs?.........................................................................................
………………………………………………………………………………….
15
THANK 1YOU 1FOR 1YOU 1TIME
Appendix 13: 1 1Interview 1guide 1for 1Implementing 1partners 1(NGOs)
INTERVIEW 1GUIDE: 1FOR 1IMPLEMENTING 1PARTNER 1(NGO’s)
Researcher 1introduction 1
My 1name 1is 1Lucky 1Museta 1I 1am 1a 1student 1from 1University 1of 1Lusaka
1conducting 1a 1research 1on 1the 1analysis 1of 1the 1government 1and 1implementing
1partners 1cost 1implication 1on 1HIV/AIDS 1case 1management 1infections 1from 12012
1- 12017: 1a 1case 1of 1western 1province, 1as 1part 1of 1my 1dissertation 1leading 1to 1the
1award 1of 1Bachelor`s 1Degree 1in 1Business 1Economics 1and 1Management 1Studies. 1I
1would 1therefore, 1be 1grateful 1for 1your 1assistance 1in 1completing 1the 1following
1questions 1to 1the 1best 1of 1your 1knowledge. 1The 1responses 1that 1you 1will 1provide
16
1in 1this 1research 1will 1be 1treated 1with 1confidentiality 1and 1only 1meant 1for
1academic 1purposes. 1 1
Background 1information
12. Age: 1
13. Marital 1status: 1
Item 1or 1questions 1to 1be 1asked 1to 1respondents 1in 1an 1interview 1
Section 1B: 1Benefits 1derived 1from 1the 1program 1since 1its 1establishment 1in 12012
1in 1Western 1Province 1establish 1how 1much 1investment 1has 1been 1made 1towards
1reducing 1the 1HIV/AIDS 1infections
14. Does 1your 1institution 1donate 1funds 1to 1carry 1out 1HIV/ 1AIDS 1program?
15. 1How 1are 1the 1funds 1been 1donated 1are 1invested 1in? 1list 1the 1HIV/AIDS
1programs 1you 1most 1donate 1to 1health 1facilities 1in 1your 1district.
16. Which 1of 1the 1HIV/AIDS 1programs 1does 1you 1NGO 1invested 1in 1mostly? 1
Section 1C: 1The 1best 1investment, 1need 1based 1options 1to 1be 1undertaken 1towards
1HIV 1high 1impact 1activities 1in 1Western 1Province
17. The 1other 1external 1organisations 1which 1help 1in 1carrying 1out 1the 1HIV/AIDS
1programs 1
18. External 1organisations 1(NGO’s) 1give 1you 1funds 1to 1promote 1the 1HIV/AIDS
1programs 1apart 1from 1the 1government 1funds? 1
19. Names 1the 1organisation 1that 1have 1invested 1in 1HIV 1activities 1in 1your 1district
Section 1D: 1The 1preparedness 1of 1the 1government 1in 1taking 1up 1the 1HIV
1program 1in 1Western 1Province
20. The 1government 1provide 1enough 1resource 1for 1the 1HIV/IDS 1programs
21. The 1health 1facilities 1in 1the 1district 1carrying 1out 1the 1HIV/AIDS 1programs
22. Type 1of 1services 1do 1your 1organisation 1funds 1most 1to 1health 1facilities
1offering 1in 1the 1district 1towards 1HIV/AIDS
1programs?..........................................................……….
17
THANK 1YOU 1FOR 1YOU 1TIME
TURNITIN REPORT
18
19
20
21