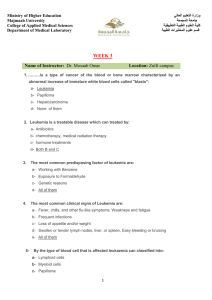
Archives of Medical Research 47 (2016) 593e606 REVIEW ARTICLE Early-age Acute Leukemia: Revisiting Two Decades of the Brazilian Collaborative Study Group Maria S. Pombo-de-Oliveira and Francianne Gomes Andrade, on behalf of the Brazilian Collaborative Study Group of Infant Acute Leukaemia* Pediatric Hematology-Oncology Research Program, Instituto Nacional de C^ancer, Rio de Janeiro, Brazil Received for publication October 28, 2016; accepted November 24, 2016 (ARCMED-D-16-00656). The understanding of leukemogenesis in early-age acute leukemia (EAL) has improved remarkably. Initiating somatic mutations detected in dried neonatal blood spots (DNBS) and in cord blood samples of affected children with leukemia have been proven to be acquired prenatally. However, to date, few epidemiological studies have been carried out exploring EAL that include infants and children 13e24 months of age at the diagnosis. Maternal exposure to transplacental DNA-damaging substances during pregnancy has been suggested to be a risk factor for EAL. Most cases of infants with acute lymphoblastic (i-ALL) or myeloid leukemia (i-AML) have KMT2A gene rearrangements (KMT2A-r), which disturb its essential role as an epigenetic regulator of hematopoiesis. Due to the short latency period for EAL and the fact that KMT2A-r resembles those found in secondary AML, exposure to topoisomerase II inhibitors has been associated with transplacental risk as proxi for causality. EAL studies have been conducted in Brazil for over two decades, combining observational epidemiology, leukemia biology, and clinical data. EAL was investigated considering (i) age strata (infants vs. 13e24 months-old); (ii) somatic mutations associated with i-ALL and i-AML; (iii) ethnic-geographic variations; (iv) contribution of maternal genotypes; and (v) time latency of exposures and mutations in DNBS. Interactions of acquired and constitutive gene mutations are challenging tools to test risk factor associations for EAL. In this review we summarize the EAL scenario (including B-cell precursor-ALL, T-ALL, and AML) results combining environmental and genetic susceptibility risk factors and we raise questions that should be considered for further action. Ó 2016 IMSS. Published by Elsevier Inc. Key Words: Infant leukemia, AML, ALL, Genetic susceptibility, Maternal environmental exposures. Introduction Early-age acute leukemia (EAL) consists of a group of leukemias that include acute lymphoblastic (ALL) and myeloid (AML) leukemias, occurring in neonates, infants, and toddlers. The term infant ALL (i-ALL) is usually applied when the diagnosis is made in children within 11 months after birth. In AML cases, however, the timeframe to categorize i-AML leukemia is extended up to * Listed in Acknowledgments. Address reprint requests to: Maria S. Pombo-de-Oliveira, Pediatric Hematology-Oncology Program, Research Center, Instituto Nacional de C^ancer-INCA, Rua Andre Cavalcanti 37, 6o floor, 20231050, Rio de Janeiro, RJ, Brazil; Phone: (þ55) (21) 32076532; FAX: (þ55) (21) 32076553; E-mail: mpombo@inca.gov.br. 24 months of age (1,2). In some settings, when the clinical signs appear shortly after birth, neonates die thereafter, whereas in others the child shows normal clinical features but hematological disturbances may appear later up to 2 years of age and more (3,4). For epidemiological association risk exposure studies, we categorized EAL as children !2 years of age. However, i-ALL is consensually defined in children !1 year of age, whereas i-AML has been categorized up to 2 years of age in which molecular markers seem similar in age strata. In both circumstances, research has shown that a particular stem cell that acquires somatic mutation during life in utero can acquire additional lesions that alter hemostasis and lead to leukemogenesis. As an example, the vast majority of i-ALL or i-AML present somatic abnormalities that affect 0188-4409/$ - see front matter. Copyright Ó 2016 IMSS. Published by Elsevier Inc. http://dx.doi.org/10.1016/j.arcmed.2016.11.014 594 Pombo-de-Oliveira and Andrade/ Archives of Medical Research 47 (2016) 593e606 the KMT2A/MLL gene with the contention that these abnormalities occur in utero. Epidemiological observations reveal that i-ALL has a peak incidence of 6 months of age, whereas i-AML has a peak at 12 months of age, including congenital or neonatal leukemias. This time frame supports the premise that the disease initiated and accumulated additional genomic lesions during fetal life. Definitive evidence for prenatal origin for the majority of childhood leukemia (CL) was derived from molecular aberrations found in archived neonatal blood spots of children with different leukemia subtypes, molecular screening of cord blood and the common clonal origin of concordant leukemia in twins (5,6). Fetal hematopoiesis is characterized by the fast growth of hematopoietic stem cells (HSC) and the speed of progenitor cell division is very high. Actually, the HSCs in fetal liver are doubling every day from the first weeks of conception and undergo relevant changes over time, either in quantitative parameters (3rde4th weeks) or from actively cycling populations to a predominant quiescent functional cell (from birth to first year of life) (7). It is possible that cells in the first wave of the hematopoietic development with fast-cycling populations are more sensitive to genotoxic insults than HSCs in quiescent phase (8). This phenomenon can sustain the hypothesis raised from the differences in age-specific incidence rates (ASIR) for lymphoid and myeloid origins (7,9,10). The International Agency for Research on Cancer (IARC), the leader of quality-assured incidence data on CL, has disclosed the incidence of cancer varying worldwide (11). The ASIR of CL in Europe and in the Middle East exemplify these differences. In children aged 0 to 14 years, CL has an estimated range from 35.0e46.7 cases per million per year. In the first 2 years of life, the incidence of CL is low and differs according to leukemia subtypes. There is an incidence peak in AML that declines after 2 years of age. In ALL, age trend is just the opposite, a lower incidence in i-ALL and an increased ASIR from 2e5 years old (http://www.euro.who.int/data/assets/pdf. file/0005/97016/4.1). These geographic and leukemia subtype variations in ASIR have been tested with measures of population mixing, indicators of socioeconomic factors, human development index, and time trends among other variables. Hypotheses concerning pathogenesis took into consideration child exposures in fetal life and beyond the first year of life. The majority of these studies relied on information ascertained through population-based cancer registry (PBCR), hospital-based cancer registry (HBCR) and case-control studies (12e14). Despite many scientific efforts and refined technology, identification of plausible causal factors that may be associated with leukemogenesis is still a challenge. Very few translational-epidemiological studies have been carried out that focus on the EAL groups that encompass congenital leukemia (diagnosed within the first month of life), infants (#11 months) and toddlers (a child between the ages of 1 and 2 years). Maternal exposures to substances with potential DNA damage during pregnancy, secondary exposures to smoking and delayed child infections have, through observational epidemiological studies, been suggested as risk factors associated with both i-ALL and i-AML. To assess dose-effect exposures in utero and ascertain how the genetic and epigenetic processes are related to molecular mechanisms is still a demand of etiological studies. We have been performing epidemiological studies on EAL in Brazil since the year 2000, combining data from maternal-child exposures and immune-molecular markers of CL. Our motivation was based on the existence of a network of uniform diagnostic tools to characterize CL subtypes. The availability of clinical data from Brazilian multicenter projects allowed us to explore the complex interaction of biological markers, lifestyle and environmental exposures in order to identify risk factors (15). Herein, we revisit the findings from studies conducted on EAL that included i-ALL and i-AML and discuss the clinical epidemiology features, diagnosis, and biology, combined with environment risk factors and genetic susceptibility in a Brazilian setting. Clinical Epidemiology To address questions related to EAL and to understand the diversity of clinical heterogeneity, we divided our focus into three groups: (A) i-ALL (#11 months of age), (B) ALL (12e24 months old) and (C) i-AML (up to 24 months). The prognosis of EAL that includes neonates and infants is still associated with poor outcome; children aged between 1 and 2 years old with B-cell precursor ALL (Bcp-ALL) and CD10pos are included in the CL good prognosis risk group. Thus, the overall survival (OS) rates related to ALL in this review should be interpreted with caution. ALL should be investigated separately according to distinct strata, immunophenotyping (CD10pos), cytogenetic category of risk prediction, minimal residual disease markers and early bone marrow response (16,17). On the other hand, for AML, there are few differences regarding biological subtypes in infants and children aged between 1 and 2 years. However, it is very important to determine association with and without Down syndrome (DS). Infant AML with DS represents a distinct leukemia pathogenesis and the spontaneous clinical remission observed in several neonates deserves a special discussion (18). Regarding clinical epidemiology of infants, the distribution frequency of AML and ALL are almost the same. We have retrospectively analyzed 808 EAL cases included in all epidemiological and molecular studies in order to reevaluate their clinical and biological features (summarized in Table 1). The ratio of ALL to AML was 1.8:1.0. There Early-age Acute Leukemia Revisited 595 Table 1. Demographic and clinical aspects of early acute leukemia with main signs and symptoms reported in the BSGIAL, Brazil, 2000e2014 Clinical observations in BSGIAL i-ALL n [ 241 (A) ALL n [ 280 (B) Males Females Age (mean, SD) Whites Non-Whites Persistent fever Pallor CNSpos (seizures) Petechiae Bone pain Easy bleeding Skin nodules and/or tumoral mass Lymph nodes Hepatomegaly Splenomegaly Down syndrome (yes/no) WBC count !10.0 103 11.0e50.0 103 $51.0 103 Hemoglobin level !7.0 $7.1 Platelets !20.0 103 21e100.0 103 $101.0 103 KMT2A/MLL-r Overall survival (95% CI) 53.1% 46.8% 5.6 (3.4) 57.3% 42.7% 59.9% 47.0% 2.0% 50.0% 4.0% 11.0% 2.5% 10.2% 14.2% 49.8% 36.1% 0.3% 7.0 (1.4) 30.9 (11.8) 91.2 (12.4) 5.5 (1.1) 8.7 (1.0) 13.3 (4.3) 49.6 (22.1) 149.8 (20.6) 71.8% 19.7 (8.6e30.8) 52.9% 46.1% 18.5 (3.8) 55.7% 44.3% 40.0% 50.0% 47.0% 5.8% 6.0% 0.4% 8.0% 23.1% 45.4% 43.1% 0.2 7.8 (1.6) 28.4 (11.3) 60.9 (15.6) 5.2 (1.6) 7.1 (1.4) 16.0; (4.24) 40.5 (13.9) 241.6 (11.9) 27.2% 87.1 (75.6e80.6) p* 0.936 0.713 0.702 0.003 0.304 0.255 0.941 0.001 i-AML n [ 287 (C) p** 55.4% 44.6% 11.6 (7.0) 51.6% 48.4% 60.8% 95.0% 1.4% 67.0% 13.9% 10.8% 17.6% 9.6% 78.6% 68.1% 22.5% 5.5 (2.6) 31.4 (12.1) 72.9 (13.8) 5.7 (1.2) 8.7 (1.0) 13.6; (3.9) 48.2 (20.9) 270.0 (13.4) 52.4% 26.7 (10.2e24.0) 0.622 0.188 0.281 0.003 0.003 !0.0001 0.05 BCSGIAL, Brazilian Collaborative Study Group of Infant Acute Leukemia; CI, confidence interval; CNS, central nervous system; i-ALL, infant acute leukemia in children #11 months-old; ALL, acute lymphoblastic leukemia in children 12e24 months-old; i-AML infant acute myeloid leukemia in children #24 months old; SD, standard-deviation. *p value A vs. B; **p value, AþB vs. C (Pearson c2). were no differences regarding sex or ethnicity. The proportion of male and female distribution was not comparable to data previously reported in the literature where the general trend is for the increased proportion of girls to exceed that in boys among infants (19). Twenty-six of 287 (9.0%) patients with i-AML were !1 month of age and characterized as congenital leukemia. Clinical signs observed by their mothers are mainly pallor, petechiae and constant fever. Tumor and increased abdominal volume are also noted. Clinically, EAL differs slightly from CL (children O2 years of age). Infants are characterized by a high white blood count (WBC), hepatosplenomegaly, tumoral lesions (mainly skin nodules), and central nervous system (CNS) involvement. For instance, massive hepatosplenomegaly and skin lesions were more frequently found in i-AML ( p 5 0.003), whereas CNS involvement was more frequent in i-ALL (in some children seizures were a sign as a proxy of leukemia infiltration). Infiltration of the CNS was also found in AML (both FAB-M4 and M5, data not shown). Skin nodules were found in both i-ALL and AML patients. The presence of lymph nodes was more prone in ALL (older children, p 5 0.003). Laboratory investigations of WBC, hemoglobin, and platelet counts were similar among the subgroups. The presence of DS was observed in i-AML ( p 5 0.001). KTM2A/MLL-r were highly frequent in i-ALL but were also found in |27% of children with ALL in the age range of 12e24 months old ( p 5 0.001). These findings support the rationale for including ALL in children O11 months old in epidemiological studies (20). Overall survival (OS) was very poor; i-ALL patients reached |41% in 5-year survival, whereas in i-AML the survival rate was |26%. Unfortunately, we have not adequately improved therapy and effective supportive care to increase the survival rates of CL (21). Because of the very low incidence of i-ALL, there was a call for collaborative studies that resulted in effective improvements for therapeutic issues. The impact of the Interfant collaborative studies brought advances in the biology and outcome of i-ALL with the benefit derived from innovative therapy (22). Differential diagnosis must be considered when young children present symptoms characterized by fever, anorexia and weight loss even in the face of a well-documented infection. For the general pediatrician, an EAL is not the first suspicious diagnosis mainly in some Brazilian endemic parasitic regions where pediatric diseases have signs and 596 Pombo-de-Oliveira and Andrade/ Archives of Medical Research 47 (2016) 593e606 Figure 1. Distribution of specific genetic abnormalities in EAL. (A) Genetic abnormalities in acute lymphoblastic leukemia (ALL) aged #12 months old. a Other abnormalities include complex karyotypes and non-recurrent abnormalities. (B) Genetic abnormalities in acute myeloid leukemia (AML). bOther abnormalities include genomic structural alterations. symptoms similar to those occurring in childhood leukemia. Diagnosis and Biology of Infant Leukemia with and without KMT2A Gene Rearrangements In this section we discuss the discoveries that have emerged from biological questions, diagnostic tests and experimental research in the subtypes of EAL. The diagnosis of any group (ALL or AML) is established through morphological and immunophenotypic examination of lymphoid and myeloid cells according to World Health Organization criteria (23). For better understanding, we subdivided this text into (i) ALL and (ii) AML, independently of age strata. There are distinct frequencies of somatic mutations among i-ALL and i-AML according to a recent publication (16) and that we summarized in Figure 1. Infant Acute Lymphoblastic Leukemia The most frequent immunophenotype in i-ALL is characterized by Bcp-ALL, CD10neg with aberrant expression of myelomonocytic markers. These features indicate that i-ALL may originate in a progenitor cell still not fully committed to the lymphoid lineage. This observation yields to a proposal that the ambiguous-lineage immunophenotype and the multilineage gene expression should consider infant leukemia as one entity, regardless of the characteristics of lymphoid or myeloid features (24,25). Detection of KTM2A/MLL-r can be accomplished by conventional cytogenetics, reverse transcriptase polymerase chain reaction (PCR), and fluorescence in situ hybridization (FISH). Long-distance inverse PCR is an important tool to identify the KTM2A/MLL fusion partner genes and the respective breakpoints. As discussed later, a wide molecular and epidemiology study on EAL has been the driving force of the network of the BCSGIAL (20). During the first years of study, the well-established cytogenetic and molecular techniques were used and, recently, novel technologies have also been incorporated. Whereas much expected data have been obtained and supported the epidemiological questions, the vast number of EAL cases analyzed also prompted the discovery of unusual/interesting clinical findings. Our first comprehensive study characterizing immunophenotype and molecular cytogenetics of EAL with KMT2A-r was published in 2006 (26). This work focused on, but was not restricted to, chromosome 11q23 region where the KMT2A is located. The majority of recurrent chromosomal aberrations is associated with KMT2A with occurrence of several partner genes (TPGs) (27). As expected, KMT2A-AFF1 was the most frequently observed fusion gene, mainly in the age range 0e12 months. KMT2A-r cases were also found in children O12 months old. Although it is well known that some KMT2A TPGs are related to a specific leukemia cell lineage such as AFF1, MLLT1 or MLLT3 in ALL and MLLT10, MLLT3 or ELL in AML (27), unusual cases were found in our study. For example, KMT2A-AFF1 in two T-cell ALL (TALL) cases and KMT2A-MLLT1 in an AML case (26). In summary, these interesting findings emerged from a ‘‘blind’’ approach that has not been strictly directed by genotype-phenotype common associations. In addition, this first molecular study served as a platform to other studies, which addressed either epidemiological (20), diagnostic (28) pharmacogenomic or genetic susceptibility questions (29,30). Regarding the diagnostic question, we analyzed a robust series of 148 childhood acute leukemias to investigate the fidelity of NG2 as a cellular membrane marker in predicting KMT2A-r. As expected, positivity of NG2 correlated well with KMT2A-r Early-age Acute Leukemia Revisited cases. Nevertheless, we observed a great variation in NG2 expression among participant centers. Based on that finding, we questioned the need for complementary diagnostic tests to ultimately determine the KMT2A status in multicenter studies (28). We concluded that FISH methods are the gold standard approach to detect KMT2A alteration, although a further test for identification of partner genes is required. Identification of KMT2A-r should be performed by FISH for any epidemiological and clinical study. In 2013, with an international collaborative effort, we were able to extend the analyses of KMT2A-r in the Brazilian series of cases to a genomic breakpoint level and the results showed that different KMT2A breakpoints correlate with age at diagnosis, WBC, and OS. This was the first study demonstrating the association between KMT2A intron 11 breakpoints and poor OS (31). In fact, previous studies demonstrated an imbalance of breakpoint distribution across different age ranges, with adult patients harboring mainly KMT2A intron 9 and 10 breakpoints, whereas breakpoints in intron 11 were more frequently found in infant ALL cases (32,33). Further functional investigations showed that disruption in intron 11 may render a more aggressive phenotype due to the switch of KMT2A function from repressor to activator protein (34). Subsequently, due to the ability to determine those KMT2A breakpoints, backtracking investigations have been performed. In the most recent investigation the temporal order of genetic hits as well as the in utero origin of both KMT2A-r and RAS mutations were studied. Despite the fact that i-ALL with KMT2A-r has a considerable scarcity of somatic mutations, RAS signaling pathway genes are the most frequently mutated (35e39). In our study, we analyzed 92 cases of i-ALL with KMT2A-r and observed that 28.7% have RAS mutations demonstrating the prenatal origin and the subclonal profile of those mutations (40). Although most i-ALL cases are characterized by a high frequency of KMT2A-r and harbor only a few additional mutations, cases without KMT2A translocations were also observed. For instance, we found four cases with ETV6RUNX1 fusion genes, which were further investigated through genome-wide copy number analysis. It is well established that the ETV6-RUNX1 fusion gene can also originate prenatally (41,42); however, the clinical onset of Bcp-ALL development is usually within the typical age peak between 2 and 5 years. We compared these i-ALL with ETV6-RUNX1 cases from older Bcp-ALL children and found recurrent gene deletions (CDKN2A, CKDN2B, MTAP, CD44, ETV6), none of which were specifically related to infants (43). Recently, two studies also evaluated KMT2A negative infant cases. The first found a significant excess of rare germline variations in leukemia-related genes (44), whereas the second showed that such cases have distinct clinical and molecular profiles when compared to non-infants. Interesting that MLL3, a homolog of KMT2A was found in these 597 patients, with frameshift insertions in SET domain similar to adult-AML. They showed an increased number of poor outcome markers such as a poor prednisone response, an immature pro-B phenotype, and fewer genetic alterations (45). Lymphoblastic leukemia in infants is far more frequently associated with an immature Bcp- phenotype; however, rare T-ALL cases also occur. Although most infant studies to date have included T-ALL (24,39), the data are often presented without distinction of lymphoid lineage. To fill this literature gap, our first study evaluated the molecular profile of 15 T-ALL cases among EAL. NOTCH1 mutations were the most frequent alterations observed followed by KMT2A-r (46). Interestingly, although KTM2A-r is uncommon in T-ALL, the MLLT1 gene located at 19p13 is the most frequent TGP found in T-ALL (27). We were able to assemble a unique series of 13 infant T-ALL cases along with matched remission samples and neonatal blood spots. In this second study, we could not only determine the molecular profile but also could elucidate the developmental timing of events for infant T-ALL. In general, the mutational spectra were distinct from those of T-ALL in older cases. For example, we observed for the first time a recurrent MLF1 deletion. For three patients, molecular alterations such as NOTCH1 mutation, KMT2AMLLT1, and PTEN deletion were backtracked to birth. Overall, these data support the idea that infant T-ALL is a unique entity and might be handled as such (47). Infant Acute Myeloid Leukemia Considering that AML is highly incident in adults, one might predict that AML would be rare in infants. However, within the earlier pediatric population (#11 months), i-AML also shows high rates. i-AML is often considered a separate biological entity when associated with DS or when based on the great genetic variability within the age distribution (48). In the epidemiological exposure studies, we excluded the setting of AML with DS. The biology of i-AML differs from that of older children, with a higher frequency of acute monoblastic (AML-M5), megakaryoblastic (AML-M7) and myelomonocytic (AML-M4) subtypes. Higher WBC count at diagnosis and extramedullary tumors are often present. Morphologic, cytogenetic, molecular genetics and initial treatment response show that these patients generally have high-risk prognostic features (18). i-AML cases also show evidence that somatic mutations were acquired in utero, giving rise to preleukemic clones (49). In the pathogenesis of AML, mechanisms at least two classes of cooperating genetic events might occur (type I and type II). As a definition, type I abnormalities lead to uncontrolled proliferation and/or survival of the myeloid cell. Type I mutations are often in activating genes involved in signal transduction pathways such as FLT3, KIT, RAS, and PTPN11. Type II abnormalities impair differentiation and result from chromosomal translocations affecting 598 Pombo-de-Oliveira and Andrade/ Archives of Medical Research 47 (2016) 593e606 hematopoietic transcription factors, such as t(8,21) (q22;q22)/RUNX1-RUNX1T1 and KMT2A-r (50). Recurrent cytogenetic abnormalities are observed in the majority of i-AML (|80%) and large differences in frequency distribution were detected in children #2 and O2 years of age (Figure 1). Higher frequencies of KMT2A-r (51%) and complex karyotypes (18%) are found in i-AML. Complex karyotypes exist for three or more genomic alterations including one structural. In contrast, the most common type II abnormalities are found in children O2 years of age that include t(8,21)(q22;q22)/ RUNX1-RUNX1T1, inv(16)(p13.1q22)/CBFb-MYH11and t(15,17)(q22;q21)/PML-RARa (rarely observed in i-AML). In both age strata (#2 and O2 years), there is a clear difference in the distribution of type I/II aberration frequencies (51). Novel data from the genomic era are emerging to show a number of new gene mutations required for i-AML pathogenesis compared with AML in older patients. One good example of this notorious genetic heterogeneity is the high frequency of unusual KMT2A-TPGs found in AML. Combining cytogenetic and molecular approaches, we described a novel TPG in an 11-month-old boy with AML-M5. The new TPG described was the NEBL fused to KMT2A and the breakpoint definition through longdistance PCR. NEBL is located on chromosome 10 in close proximity to the common TPG MLLT10 (52). Subsequent to this case report and based on the knowledge that both direct and reciprocal KMT2A-r might play a role in leukemogenesis (53), by cloning both cassettes for KMT2ANEBL and NEBL-KMT2A into a sleeping beauty vector, we were able to analyze the biological effects of those transcripts in a conditional cell culture model. The results demonstrated that the reciprocal NEBL-KMT2A fusion protein had more significant growth-promoting potential than KMT2A-NEBL (54). Other acquired genetic translocations can be observed in i-AML. Besides KMT2A-r, the NUP98-HOXD13 is an example of a recurrent event in de novo AML; nevertheless, in infants, this is a rarely found abnormality. In 2011, we described the third NUP98-HOXD13 infant case diagnosed with AML-M4. Furthermore, the availability of archived neonatal blood spots allowed us to prove, for the first time, the in utero origin of NUP98-HOXD13 (55). Other than KMT2A-r, aberrations such as t(7,12) (q36;p13)/MNX1-ETV6 and t(7,12)(q32;p13) encompasses almost 30% of i-AML (56). The chromosome translocations t(8,16)(p11;p13)/MYST3-CREBBP (57), t(1,22) (p13;q13)/RBM15-MKL1 (58), and inv(16)(p13.3q24.3)/ CBFA2T3-GLIS2 (59) (the latter two associated with nonDS acute megakaryoblastic leukemia [AMKL]) are also specifically associated with i-AML group and with adverse prognosis. The incidence of these rearrangements could be underestimated because of the inherent difficulty in detection using conventional cytogenetics (60). The chromosome translocation t(8,16)(p11;p13) that generates the MYST3-CREBBP fusion gene seems to have an age-dependent association with prognosis because 28% of i-AML were diagnosed in the first month of life (congenital leukemia). This translocation is associated with spontaneous remission and warrants a watch-and-wait strategy before any aggressive therapy. Older children require intensive chemotherapy (57). Reviewing the morphological features of i-AML we have observed some cases with hemophagocytosis in blast cells. This remarkable feature was associated with the reciprocal fusion gene MYST3-CREBBP and AML with monocytic differentiation (AML-M5). Differential diagnosis should be performed with hemophagocytic syndrome being a deadly disease (57,61). The chromosome abnormality t(1,22)(p13;q13)/RBM15-MKL1 was found exclusively associated with i-AML with megakaryoblastic differentiation (i-AMKL subtype) in |30% of children !1 year of age (51). Another abnormality restricted to i-AMKL subtype is the CBFA2T3-GLIS2 fusion gene, identified in a cryptic translocation of cytogenetically normal i-AML. In both groups, infant survival was poor (62,63). Type I aberrations are rare in i-AML, and we observed that the frequency of FLT3 and KIT mutations increase with age. In children #2 years of age, the majority of cases did not harbor the common type I aberrations (51,64). The genesis and alleyways by which these fusion genes are associated with different leukemia subtypes remain largely unknown. There are hypotheses that the risks of developing EAL are modulated by complex interactions between inherited predispositions at genetic and epigenetic levels, environmental exposures to damaging agents and chance events (model summarized in Figure 2). That is why these EAL are so intriguing. As a whole, in EAL the window of clinical onset and the environmental exposures is open very briefly. The effects of contact with various substances contact might be transmitted at a fetal cellular level with uniform exposure through the placental barrier. Although relatively little is known about the exact oncogenic mechanisms of environmental fetal insults, many known carcinogen metabolites can potentially transpose the placenta barrier and elicit genomic and epigenetic effects at many levels. These include effects on DNA repair, cell-cycle control, cellmethylation, chromatin alterations and apoptosis. It has been demonstrated that environmental conditions during fetal development alter epigenetic mechanisms that silence genomic regions, conferring an important role to placental genetic and epigenetic profiles in protecting the fetus from substance insults (65). Observational Epidemiology, Maternal Exposures and EAL Risk Factors The incidence rates of cancer represent a virtual portrait of health in context with environmental factors and potential Early-age Acute Leukemia Revisited 599 Figure 2. Model of the hypothesis for the modulated risk of developing EAL by the complex interactions between inherited predispositions at genetic and epigenetic levels, environment exposures to damaging agents and chance of events. causative agents associated with malignancies. Eventually, specific exposure to ionizing and non-ionizing radiation, chemicals, virus and a wide range of familial and genetic syndromes contribute to CL. However, evidence-based epidemiology has demonstrated that 80% of CL in the first decade of life are ALL and vary in immune-phenotype according to ASIR. In Brazil, we estimated the ASIR of CL according to world populations aged 0e4 years in 18 PBCR with 8 years of consolidated datasets (Figure 3). We observed a regional variation in incidence rates. An incidence peak in i-AML with a rate of 18.32 per million, declining to 10.65 per million for children O2 years old, was found. In contrast, i-ALL has a lower incidence rate (12.88 per million) and an increased ASIR from 24 months old up to 67.77 per million in children 48 months of age. When age- and gender-specific incidence rates were evaluated, males #11 months old had higher rates (44 per million) than females (20 per million). ALL/AML ratio in children #11 months of age was 0.7 (66). Along with their biological heterogeneity and clinical outcomes, i-ALL and i-AML are split in this age range and still require a broad division for cell origin, gene aberrations and exposure associations. In some EAL settings, backtracking has demonstrated that somatic genetic alterations occurring during fetal life are associated with the effects of potential damage to fetal DNA during pregnancy (67). HSC expand in fetal liver and in bone marrow over a short period, and cells receive continuous stimuli for proliferation, differentiation, and cellular division. Therefore, this fast-cycling cell population is more exposed to genotoxic insults than quiescent cells. Transplacental exposures to certain substances are harmful to the fetus. This is why the great majority of EAL with KMT2A/MLL-r and other genomic aberrations occur in utero. It was previously postulated that transplacental exposures to DNAtopoisomerase-II inhibitors (Topo-II inhibitors), which form cleavable complexes, was related to infant leukemia with KMT2A/MLL- r (68). Among i-AML, genomic aberrations are peculiar and markedly different from those found in older children. The group of Topo-II inhibitors comprise known substances such as benzene metabolites (benzoquinone), isoflavones (genistein), flavonoids, quercetin, lignin, podophyllin resin, quinolone, pesticides. These among others have been questioned by some epidemiologists who designed studies to explore maternal exposures shortly before or during pregnancy. Risk associations were found for maternal exposures to maternal fetal losses, maternal alcohol consumption, dipyrone, [odds ratio (OR), 1.45], metronidazole, (OR, 1.72), quinolones (OR, 2.25) and hormones. Maternal and childbirth characteristics, consumption of dietary-specific DNA topo-II inhibitors, pesticide exposures and parental smoking were also investigated (Table 2). Overall, most of the CL caseecontrol studies handled in recent decades did not separate i-ALL or i-AML from questions primarily designed to address the hypothesis that maternal exposures would be associated with leukemia in offspring. The maternal history of fetal loss and risk of CL carried out in some studies produced contradictory results. Alcohol consumption during pregnancy has increased ALL (OR, 2.0) and AML (OR, 2.6), whereas no association with maternal-paternal smoking during pregnancy before or 600 Pombo-de-Oliveira and Andrade/ Archives of Medical Research 47 (2016) 593e606 Figure 3. Age-adjusted incidence rate for childhood leukemia (#4 years old) in 18 PBCR in Brazil according to leukemia subtype, 1999e2009. AAIR, adjusted by world population/per million; NALL, non-lymphoblastic leukemia; ALL, acute lymphoblastic leukemia. Sources: Population-Based Cancer Registries; MP/Fundaç~ao Instituto Brasileiro de Geografia e Estatıstica (IBGE); MS/INCA/CPV/Divis~ao de Vigil^ancia e Analise de Informaç~ao; www.inca.gov. br. Courtesy of Dr. Rejane Reis. (A color figure can be found in the online version of this article.) after the index child’s birth was observed. Meta-analysis and or pool analysis investigated the association between maternal-child birth characteristics, exposures during pregnancy to solvent, paint, and petroleum and demonstrated variable risk associated with CL. Relevant epidemiological studies related to maternal exposures and CL (up to September 1, 2016) were identified by searching PubMed; however, there are very few EAL exclusively tested. Ten years after our first publication in 2006, a new extensive review of the literature failed to reveal additional studies, apart from those of our own group, that focused exclusively on infants. Our major aim was to explore maternal environmental exposures during pregnancy and the risk of EAL with KMT2A/MLL-r (latter, not exclusively). A hospitalbased case-control study was designed in the year 2000 and conducted since then. The result of the study was divided into three periods: 1st) from 2000e2006, the study was restricted to infants (#11 months) and toddlers (#18 months) cases. Controls were children without malignancies aged up to 48 months at recruitment; 2nd) from 2007e2012, the study incorporated new questions related to child exposures in the first two years of age, thus, child ages increased to #5 years of age. The variables concerning maternal exposures during pregnancy remained. Finally, from 2011e2015, the study had a special focus in an AML setting. In the first analysis, a total of 210 newly diagnosed cases of EAL were enrolled (1:3 ratios, with matched controls). Controls were selected from the same hospitals where EAL cases were treated. The strong significant association observed with estrogen exposure (OR, 8.76) during pregnancy was the surprising finding not explored in previous investigations (20,67). The possible biological reason for KTM2A/MLL formation was tested in experimental studies by Schnyder et al. (69). Genomic DNA from the TK6 human lymphoblastoid cell line exposed to different levels of either E2 or 4-OH-E2 was analyzed by ligation-mediated PCR and inverse PCR. After exposure to E2, increased rates of DNA double-strand breaks within the KTM2A/MLL breakpoint cluster region were observed along with KMT2A-r (69). In another study on 92,719 women recruited into the Danish National Birth Cohort, 1.2% of women referred took contraceptives during pregnancy, the percentage being higher among mothers of infant leukemia (|6%), especially those carrying KTM2A/ MLL abnormalities (70). The following analysis was used to test whether high birth weight was associated with EAL. We compared the birth weight distribution among EAL and comparisons were performed with the general population using the stratum 2500e2999 g as a reference. An increased significant trend on the OR between i-ALL and birth weight were observed in children with birthweight 3000e3999 g Table 2. Summary of the main epidemiological study results of risk factors conducted in each infant leukemia group Study group Risk factor associations EAL 154; controls 842 EAL (ALL and AML) was associated with maternal fetal losses with 5-fold increased risk ( p 5 0.001), whereas $2 fetal losses were associated with 12-fold increased risks ( p 5 0.001). Maternal alcohol consumption during pregnancy: OR,1.43; 95% CI (1.00e2.04) for ALL and OR, 2.64; 95% CI (1.36e5.06) for AML. More females: OR,1.58; 95% CI (1.17e2.13); increased risk for children who weighed O4000 g at birth OR, 2.28; 95% CI (1.26e4.13); previous maternal miscarriage: OR,1.45; 95% CI (1.00e2.09). Herbal teas (medicine): OR, 2.93; 95% CI (1.57e5.48); DNA-damaging drugs: OR, 1.71; 95% CI (1.03e2.84); mosquito pesticides: OR, 5.14; 95% CI (1.27e20.85); overall pesticides: OR, 3.67; 95% CI (1.54e8.74); dipyrone: OR, 2.83; 95% CI (1.15e6.99). Maternal exposure to mind-altering drugs: i-ALL OR, 1.8; 95% CI (1.0e3.1), p ! 0.01. Yeazel, 1995 AL 240; controls 255 Maternal consumption of dietary-specific DNA topoisomerase-II inhibitors associated with AML with KTM2A-r OR, 1.9; 95% CI (0.5e7.0). Spector et al., 2005 AL-case mother, 337 control mother, 697 ALL 765 (i-ALL 19 and AML 25); controls 1681 No statistical significance was found, but in T-ALL settings OR, 0.21; 95% CI (0,08e0.51); only 30 i-ALL included Milne et al., 2011 Paternal smoking associated with ALL OR,1.45 (1.1e1.7); AML OR, 1.50 (1.0e2.3); observed an increased OR directly proportional to number of cigarettes smoked; EAL, 97 cases. Rudant et al., 2008 EAL 202, ALL 193, AML 49; controls 480 Dipyrone; adjOR, 95% CI (1.45e2.08). Hormones taken during pregnancy: adjOR 8.76, 95% CI, (1.45e2.08); overall pesticides: adjOR, 2.78, 95% CI (1.53e2.83); herbal medicine OR, 2.93, 95% CI (1.57e5.48). Pombo de Oliveira et al., 2006 Comparisons with the general population (2500e2999 g as reference); i-ALL 3000e3999 g presented an OR, 1.68, 95% CI (1.03e2.76); birthweight 4000 g or more OR 5 2.28 (95% CI 1.08e4.75), p !0.01. Pregnancy maternal smoking, no overall association; subset of mothers who smoked O20 cigarettes/day an adjOR, 5.28 (95% C.I, 1.40e19.95) for i-ALL was observed. Maternal use of hair dyes and straightening products: adjOR, 1.78, 95% CI, 1.13e2.81for i-ALL and an adjOR of 2.43 (95% CI 1.13e5.22) for AML was observed. Increased risk estimates of EAL associated with maternal exposure during pregnancy to pesticides were observed: either for i-ALL (adjOR 2.10, 95% CI 1.14e3.86) or i- AML (adjOR 5.01, 95% CI 1.97e12.7). Among ALL in children 11e23 months, OR 1.88, 95% CI 1.05e5.23. Alcohol reported by 43% of i-ALL mothers and 39% of AML mothers. This analysis failed to demonstrate the increased risk association of EAL with maternal intake of alcohol during pregnancy; however, consumption of alcohol O1 glass/week OOR, 7.18 (1.09e47.3) for AML Maternal exposure to analgesic intake dipyrone showed OR, 1.63, 95% CI (1.06e2.53) during lactation, OR, 2.00 CI (1.18e3.39). Acetaminophen just the opposite: OR, 0.39 (0.17e0.93) Koifman et al., 2008 i- ALL 203 and AML 88; controls 558 i-ALL 181, AML 115; controls 468 i-ALL 49, AML 74; controls 266 i-ALL 64; controls 81 EAL 252, i-AML 59, i-ALL (?) EAL 231, controls 411 Reference Shu et al., 1996 Ross, 1997 Alexander et al., 2001 Wen et al., 2002 Early-age Acute Leukemia Revisited Children’s Cancer Study Group Children’s Cancer Study Group Children’s Cancer Study Group International Study Group, UK 1994e1999 Children’s Cancer Group, USA, Canada and Australia Children’s Oncology Group USA, 1996e2002 Australian Group (meta-analyses) ESCALE study (national registrybased case-control study) Summary of the main epidemiological studies conducted in EAL, Brazil 2006e2014 1. High birth weight 2. Maternal smoking during pregnancy 3. Hair dyes and straightening products 4. Pesticides 5. Maternal alcohol consumption 6. Maternal exposure to analgesics n Ferreira et al., 2012 Couto et al., 20013 Ferreira JD et al., 2013 Couto A et al., 2015 i-ALL, infant acute lymphoblastic leukemia (age #12 months); AML, acute myeloid leukemia (ages up to 24 months); EAL, early-age leukemia including both ALL and AML (ages up to 24 months); OR, odds ratio; CI, confidence interval; adjOR, adjusted OR. 601 602 Pombo-de-Oliveira and Andrade/ Archives of Medical Research 47 (2016) 593e606 (OR, 1.69), and those with birthweight $4000 g showed an OR, 2.28 in a dose-response effect ( p !0.01) (71). An increased risk was also observed for KTM2A-MLLþve cases (OR, 2.68), although a trend with a borderline statistical significance. Hence, because this analysis was performed on the same subjects, it is a reasonable hypothesis that the association between birth weight and EAL could be a result of the effect of maternal hormonal intake during the pregnancy, inducing an increase in the child’s birth weight. Nevertheless, when adjusted for sex, income, pesticide exposures and hormonal intake, the data reveal an independent effect of birth weight on the association with EAL. Next, in an extended investigation revisiting the same dataset, we explored the association of specific types of pesticides, mainly those used on pets and in mosquito control (72). Pesticide exposure was carefully evaluated according to responses from mothers relative to any contact occurring during the periconceptional period throughout each pregnancy trimester and after birth (during breastfeeding). The chemical content of product brand names was also identified. The association with EAL was tested according to variables such as household (domestic use), agricultural use and accidental (unintentional use). Pesticides were classified as pyrethrins and/or pyrethroids around households and insecticides related to agricultural activities. Pyrethrins are widely used in Brazil to kill bugs and mosquitoes. In this analysis, pyrethroids were the most frequently used pesticide during pregnancy as reported by the interviewed participants (21% of all case-mothers and 83% of control-mothers). As a whole, positive associations were observed between maternal exposure to pesticides and EAL (adjusted OR [adjOR], 2.10) and for i-AML (adjOR 5.01). An exposure to permethrin was associated with high risk for i-ALL (adjOR, 2.47) and adjOR, 7.28 from i-AML. In terms of biological plausibility for such specific exposure, experimental work demonstrated that pyrethroids enhance WNT proto-oncogene expression at a low concentration, which implicates perturbation of the regulation of cell fate during embryogenesis. In a model of breast carcinogenesis model, such overexpression and elevated estrogen levels have led to tissue proliferation (73). Maternal exposure to hair dyes and hair straightening products during pregnancy and EAL were also tested. In this investigation, the risk factor variables, the commercial brand names of the cosmetic products, were cautiously translated to their respective chemical components. Substances were classified according to their chemical structure (acids, alcohols, aldehydes, amines, ketones, chlorides, esters, phenols, inorganic substances, etc). Whenever compounds have multiple functional groups the variable group was classified according to the predominant one. An increased risk (adjOR, 1.78) was observed for i-ALL, whereas for AML it was even higher (adjOR 2.43) (74). Products containing 2-amino-3-hydroxypyridine, carbomer, cetrimonium chloride, 2-methyl-5-hydroxyethylaminophenol, ethanolamine, butylparaben/ethylparaben, m-aminophenol, oleth-30 and polyquaternium-22 were associated with adjusted i- ALL risk (OR, 2.76). Limitations of these investigations concern the small number of cases according to leukemia subtypes, categorizing products with a large variety of chemical compounds, precise information of time-length of maternal exposures, and whether the exposure was permanent or temporary. As may occur in a hospital-based case-control study, the design may lead to recall and selection bias. The evidence of a particular type of association risk with selected substances and EAL should be confirmed by studies in pooled analyses with other exposed and non- exposed populations. For instance, cigarette smoking and maternal alcohol consumption during pregnancy were investigated. In our investigations, the results failed to support the hypothesis of an increased associated risk of EAL, neither by the interaction with tobacco nor by alcohol consumption (75,76). Again, the pitfalls of such studies take into consideration the level of maternal perception of rapport to censored topics that may lead to imprecise exposure estimates. Epidemiological studies are still being performed in order to test parental occupation and other maternal-child EAL risk factors. Genetic Susceptibility in the Modulation of Exposures Multiple genetic lesions are a requirement for development of a malignant clone and disease. Genetic polymorphisms defined by single nucleotide polymorphism (SNP) natural variations occur randomly in the general population and confer a susceptibility or predisposition to diseases (77). This has been explored as an important part of the risk factor constellation of EAL because environmental exposure of the child to xenobiotics, directly or indirectly, can contribute to the accumulation of somatic mutations. The main investigated gene polymorphisms comprised the genes CYP1A1, CYP2D6, CYP2E1, CYP3A4, CYP3A5, EPHX1, GSTM1, GSTP1, GSTT1, MDR1, MPO, NAT1, NAT2, and NQO1 reviewed recently by Brisson et al. (78). Genetic susceptibility conferred by SNPs of genes encoding enzymes involved in the activation and detoxification of xenobiotic metabolisms modulates the risk of CL (79). It is important to consider that physiological immaturity is significant regarding susceptibility to xenobiotic exposure of infants and toddlers (80). Because of a consistent increased risk of EAL associated with maternal exposure to dipyrone during pregnancy, we tested the distribution of NAT2 polymorphisms in dyads previously investigated in the exploratory study (20,81). N-acetyltransferase 2 is a phase II metabolic enzyme that catalyzes the conjugation (N-acetylation) and activation (O-acetylation) of heterocyclic amine drugs such as metamizole (dipyrone), a Early-age Acute Leukemia Revisited non-steroidal anti-inflammatory drug widely used in Brazil as analgesic and antipyretic. SNPs in some distinct positions of the NAT2 alleles result in either rapid or slow acetylation, modifying the risk of potentially toxic substances. NAT2 slow acetylation phenotype was associated with EAL (OR 8.90). Mothers exposed or not to dipyrone were associated with the child’s risk of leukemia (OR, 4.48 and 4.27, respectively). However, the combination of dyads NAT2 slow/slow phenotypes conferred a very high risk of EAL (OR, 30.0; 95% CI, 5.87e279.7) (81). Following in the footsteps of our observational epidemiological results, we next studied the leukemogenic pathways in EAL, keeping in mind the consistent identification of somatic gene mutations occurring in fetal life such as KTM2A/MLL-r and/other fusion genes or additional gene mutations (82). These somatic mutations might occur due to errors in cellular differentiation, modulated by some inherited gene variant (83). Because we were intrigued by the results that maternal tobacco smoking during pregnancy was not casually associated with EAL, we tested whether EAL subtypes were associated with KTM2A/MLL-r, RAS mutation and some genetic susceptibility. Previous studies demonstrated a strong association of AML-RASmut and exposure to solvents (OR 4.8) (84). Our data demonstrated a strong association between EAL with RASmut and the presence of household smoking during the pregnancy or during the early life of the child; children with NAD(P)H: quinone oxidoreductase (NQO1) rs1800566 (C609T) polymorphism increased nearly threefold the risk of developing EAL (OR 5 2.97). The presence of at least one variant allele of NQO1 rs1800566 showed an increased risk of EAL (OR 5 4.24) (85). The detoxification enzyme NQO1 is a flavoenzyme that detoxifies benzene metabolites, quinines, and azo-dyes. NQO1 has an important function to protect cells against mutagenicity from free radicals and oxygen metabolites (86). The NQO1 C609T (P187S) polymorphisms have been strongly associated with the risk of childhood ALL, particularly for IL with MLL-r (87). We found that NQO1 C609T modified risk in pediatric leukemia depending on age range and the variant genotype in combination with other gene polymorphisms such as Paraoxonase 1 (PON1) gene variant. Paraoxonase 1 (PON1) has antioxidant properties and functional activity in the oxidative stress process. PON1 functions to destroy oxidized lipids and hydrolyzes active metabolites of several organophosphorus pesticides (88). The most common PON1 polymorphisms A21439G (PON1 Q192R) and T12801A (PON1 L55M) cause variability in enzyme activity, affecting its sensitivity to xenobiotic metabolism in young children (89). We investigated NQO1 and PON1 polymorphisms associated with EAL considering leukemia subtypes and age at onset of disease. We found that infant leukemia with KTM2A/MLL-r was strongly associated with NQO1 C609T variant genotype 603 (OR, 2.93), whereas PON1L55M polymorphisms increased the risk of ALL in children $13 months of age (OR, 3.2). The inadvertent exposure to hormones (biochemically similar to Topo-II inhibitors) has also been tested in which the rationale was that estrogen metabolites lead to the formation of quinone as well as reactive oxygen species, thus mutagenic substances. Estrogen metabolism is modulated by CYPs, GSTs and SULTs enzymes that in the presence of genetic variant forms affect their activity. CYP1B1 catalyzes biotransformation of estradiol to 4-hydroxyestradiol, whereas the missense variant CYP1B1, rs1056836 leads to a leucine to valine change at protein level (p.L432V) (30). CYP3A4 acts for the 2-hydroxylase ion of estradiol, whereas CYP3A5 catalyzes 4-hydroxyestradiol in the liver. A polymorphism at the 50 promoter region of CYP3A4 generates an adenine to guanine substitution (CYP3A4, rs2740574). Yet, in estrogen metabolism, GSTs and SULTs inactivate estrogen and intermediate compounds, so avoiding the formation of carcinogens such as 3,4estradiolquinones. Two polymorphisms SULT1A1*2, rs9282861 and SULT1A1*3, rs1801030 have been reported to decrease both activity and thermostability of the enzyme (30). GSTT1*0, CYP3A4*1B, and CYP3A5*1 were associated with increased risk of iAML after adjustment for multiple comparisons in non-whites and male children (OR 5 1.91, 95% CI: 1.12, 3.28; OR 5 2.44, 95% CI: 1.10, 5.43; OR 5 1.98, 95% CI: 0.96, 4.10, respectively). Notably, CYP1B1 was not expressed in the majority of EAL cases and, when expressed, varied according to genotype status and gender. Maternal-fetal genotypes showed a pronounced association with EAL according to CYP3A4*1B and GSTT1*0, demonstrating that genetic polymorphisms involved in estrogen metabolism confer different susceptibility risks to EAL, modulating leukemia subtype in males. In conclusion, acute leukemia in early childhood gathers groups of different biological subtypes characterized by somatic mutations associated with specific age strata. Overall, CL represents a paradigm for multidisciplinary research over four decades. Although more than two-thirds of ALL can be cured with current clinical trials, a subgroup stratified by early-age (neonates, infants, and toddlers) remains a challenge. Several questions remain to be answered through research on epidemiological, biological and genetic bases. The sum of epidemiological and molecular information appears to support the hypothesis that maternal exposures before conception, during pregnancy, and during lactation are unravelling pieces of the puzzle of processes associated with increased risk of EAL. Increased risks in the offspring of exposed mothers highlight the aforementioned periods of biological vulnerability in EAL. Considerations should be made to establish disease prevention policies which, once established, will be clinically similar worldwide. 604 Pombo-de-Oliveira and Andrade/ Archives of Medical Research 47 (2016) 593e606 Conflict of Interest None declared. Acknowledgments and co-Authorships Special thanks to Dr. Anthony Ford who kindly reviewed the manuscript with critical points and provided English language polish; to Mariana Emerenciano and Marcela B. Mansur who selected studies to be revisited and included and to all the dedicated technicians of the Pediatric Hematology-Oncology Program. The authors are grateful to all the collaborators who participated actively in the network of the Brazilian Collaborative Study Group of Infant Acute Leukaemia and considere them co-authors: Eny Guimar~aes Carvalho, Ana M. Marinho da Silva, Jozina Marian de Andrade Agareno, Maria Dolores Dorea, Flavia Nogueira Serafim Araujo,Lilian Maria Burlachini,Cyntia Curvello Teresa Cristina Cardoso, Nilma Pimentel de Brito, Bruno M. Rocha Freire, Maurıcio de Souza Meire, Terezinha J. Marques Salles, Renata S. Carvalho Gurgel, Andrea Gadelha Nobrega, Eloisa Cartaxo Eloy Fialho, Gustavo Ribeiro Neves, Vitoria Regia Pinheiro, Silvia R. Brandalise, Isis M. Quezado Magalh~aes, Jose Carlos Martins Cordoba, Anna Carolina Silva Dias, Patricia Carneiro de Brito, Rosania M. Baseggio, Marcelo dos Santos Souza, Atalla Mnayarji, Meyriele Bacarini Machado, Elaine Sobral da Costa, Marcelo Land, Paulo Ivo Cortez de Araujo, Fernando de Almeida Wernerck, Monica Lankszner, Alexandre Apa, Soraya Rouxinol, Maria Luiza Macedo Silva, Gilberto Ramos, Joaquim Caetano Aguirre, Wellington Mendes, Maria Lucia Marinho Lee, Alejandro Mauricio Arancibe, Renato Melaragno, Renato de Paula Guedes Oliveira, Lilian Maria Cristofani, Claudia Teresa Oliveira, Denise B. Silva, Ana Freund Winn, Imaruı Costa, Mara Albonei Dudeque Pianovski, Mariana Emerenciano, Sergio Koifman ( posmortem). References 1. Chessells JM, Eden OB, Bailey CC, et al. Acute lymphoblastic leukaemia in infancy: experience in MRC UKALL trials. Report from the Medical Research Council Working Party on Childhood Leukaemia. Leukemia 1994;8:1275e1279. 2. Bhojwani D, Yang JJ, Pui CH. Biology of childhood acute lymphoblastic leukemia. Pediatr Clin North Am 2015;62:47e60. 3. Isaacs H. Fetal and neonatal leukemia. J Pediatr Hematol Oncol 2003;25:348e361. 4. Moura SV, Andrade F, Magalh~aes IQ, et al. Clinical and molecular epidemiology of neonatal leukemia in Brazil. Leuk Lymphoma 2015;56:903e909. 5. Greaves MF. Leukemia in twins: lessons in natural history. Blood 2003;102:2321e2333. 6. Greaves M. In utero origins of childhood leukaemia. Early Hum Dev 2005;81:123e129. 7. Eaves CJ. Hematopoietic stem cells: concepts, definitions, and the new reality. Blood 2015;125:2605e2613. 8. Udroiu I, Sgura A. Genotoxic sensitivity of the developing hematopoietic system. Mutat Res Rev Mutat Res 2016;767:1e7. 9. Bowie MB, Kent DG, Dykstra B, et al. Identification of a new intrinsically timed developmental checkpoint that reprograms key hematopoietic stem cell properties. Proc Natl Acad Sci U S A 2007;104: 5878e5882. 10. Babovic S, Eaves CJ. Hierarchical organization of fetal and adult hematopoietic stem cells. Exp Cell Res 2014;329:185e191. 11. Curado MP, Voti L, Sortino-Rachou AM. Cancer registration data and quality indicators in low and middle income countries: their interpretation and potential use for the improvement of cancer care. Cancer Causes Control 2008;20:751e756. 12. Stiller CA, Kroll ME, Boyle PJ, et al. Population mixing, socioeconomic status and incidence of childhood acute lymphoblastic leukaemia in England and Wales: analysis by census ward. Br J Cancer 2008;98:1006e1011. 13. Poole C, Greenland S, Luetters C, et al. Socioeconomic status and childhood leukaemia: a review. Int J Epidemiol 2006;35:370e384. 14. Rodriguez-Galindo C, Krailo M, Frazier L, et al. Children’s Oncology Group’s 2013 blueprint for research: Rare tumors. Pediatr Blood Cancer 2012;60:1016e1021. 15. Pombo de Oliveira MS, Koifman S, Vasconcelos GM, et al. Development and perspective of current Brazilian studies on the epidemiology of childhood leukemia. Blood Cells Mol Dis 2009;42: 121e125. 16. Pui CH, Carroll WL, Meshinchi S, et al. Biology, risk stratification, and therapy of pediatric acute leukemias: An update. J Clin Oncol 2011;29:551e565. 17. Lauten M, Moricke A, Beier R, et al. Prediction of outcome by early bone marrow response in childhood acute lymphoblastic leukemia treated in the ALL-BFM 95 trial: differential effects in precursor B-cell and T-cell leukemia. Haematologica 2012;97:1048e1056. 18. Creutzig U, van den Heuvel-Eibrink MM, Gibson B, et al. Diagnosis and management of acute myeloid leukemia in children and adolescents: recommendations from an international expert panel. Blood 2012;120:3187e3205. 19. Ross JA, Xie Y, Davies SM, et al. Prescription medication use during pregnancy and risk of infant leukemia (United States). Cancer Causes Control 2003;14:447e451. 20. Pombo-de-Oliveira MS, Koifman S, Brazilian Collaborative Study Group of Infant Acute Leukemia. Infant acute leukemia and maternal exposures during pregnancy. Cancer Epidemiol Biomarkers Prev 2006;15:2336e2341. 21. Ferman S, Santos Mde O, Ferreira JM, et al. Childhood cancer mortality trends in Brazil, 1979-2008. Clinics (Sao Paulo) 2012;68: 219e224. 22. Pieters R, Schrappe M, De Lorenzo P, et al. A treatment protocol for infants younger than 1 year with acute lymphoblastic leukaemia (Interfant-99): an observational study and a multicentre randomised trial. Lancet 2007;370:240e250. 23. Arber DA, Orazi A, Hasserjian R, et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood 2016;127:2391e2405. 24. Biondi A, Cimino G, Pieters R, et al. Biological and therapeutic aspects of infant leukemia. Blood 2000;96:24e33. 25. Armstrong SA, Hsieh JJ, Korsmeyer SJ. Genomic approaches to the pathogenesis and treatment of acute lymphoblastic leukemias. Curr Opin Hematol 2002;9:339e344. 26. Emerenciano M, Agudelo Arias DP, Coser VM, et al. Molecular cytogenetic findings of acute leukemia included in the Brazilian Collaborative Study Group of Infant Acute Leukemia. Pediatr Blood Cancer 2006;47:549e554. 27. Meyer C, Hofmann J, Burmeister T, et al. The MLL recombinome of acute leukemias in 2013. Leukemia 2013;27:2165e2176. 28. Emerenciano M, Renaud G, Sant’Ana M, et al. Challenges in the use of NG2 antigen as a marker to predict MLL rearrangements in multicenter studies. Leuk Res 2011;35:1001e1007. 29. Mata JF, Silveira VS, Mateo EC, et al. Low mRNA expression of the apoptosis-related genesCASP3, CASP8, and FAS is associated with low induction treatment response in childhood acute lymphoblastic leukemia (ALL). Pediatr Blood Cancer 2010;55:100e107. 30. Lopes BA, Emerenciano M, Gonçalves BA, et al. Polymorphisms in CYP1B1, CYP3A5, GSTT1, and SULT1A1 are associated with early age acute leukemia. PLoS One 2015;10:e0127308. Early-age Acute Leukemia Revisited 31. Emerenciano M, Meyer C, Mansur MB, et al. The distribution of MLL breakpoints correlates with outcome in infant acute leukaemia. Br J Haematol 2013;161:224e236. 32. Cimino G, Rapanotti MC, Biondi A, et al. Infant acute leukemias show the same biased distribution of ALL1 gene breaks as topoisomerase II related secondary acute leukemias. Cancer Res 1997;57: 2879e2883. 33. Reichel M, Gillert E, Angerm€uller S, et al. Biased distribution of chromosomal breakpoints involving the MLL gene in infants versus children and adults with t(4;11) ALL. Oncogene 2001;20: 2900e2907. 34. R€ ossler T, Marschalek R. An alternative splice process renders the MLL protein either into a transcriptional activator or repressor. Pharmazie 2013;68:601e607. 35. Taketani T, Taki T, Sugita K, et al. FLT3 mutations in the activation loop of tyrosine kinase domain are frequently found in infant ALL with MLL rearrangements and pediatric ALL with hyperdiploidy. Blood 2004;103:1085e1088. 36. Liang DC, Shih LY, Fu JF, et al. K-Ras mutations and N-Ras mutations in childhood acute leukemias with or without mixed-lineage leukemia gene rearrangements. Cancer 2006;106:950e956. 37. Driessen EM, van Roon EH, Spijkers-Hagelstein JA, et al. Frequencies and prognostic impact of RAS mutations in MLLrearranged acute lymphoblastic leukemia in infants. Haematologica 2013;98:937e944. 38. Prelle C, Bursen A, Dingermann T, et al. Secondary mutations in t(4; 11) leukemia patients. Leukemia 2013;27:1425e1427. 39. Andersson AK, Ma J, Wang J, et al. The landscape of somatic mutations in infant MLL-rearranged acute lymphoblastic leukemias. Nat Genet 2015;47:330e337. 40. Emerenciano M, Barbosa Tda C, de Almeida Lopes B, et al. Subclonality and prenatal origin of RAS mutations in KMT2A (MLL)rearranged infant acute lymphoblastic leukaemia. Br J Haematol 2015;170:268e271. 41. Mori H, Colman SM, Xiao Z, et al. Chromosome translocations and covert leukemic clones are generated during normal fetal development. Proc Natl Acad Sci U S A 2002;99:8242e8247. 42. Ford AM, Bennett CA, Price CM, et al. Fetal origins of the TELAML1 fusion gene in identical twins with leukemia. Proc Natl Acad Sci U S A 1998;95:4584e4588. 43. Emerenciano M, Bungaro S, Cazzaniga G, et al. ETV6-RUNX1 fusion gene and additional genetic changes in infant leukemia: a genome-wide analysis. Cancer Genet Cytogenet 2009;193:86e92. 44. Valentine MC, Linabery AM, Chasnoff S, et al. Excess congenital non-synonymous variation in leukemia-associated genes in MLLinfant leukemia: a Children’s Oncology Group report. Leukemia 2014;28:1235e1241. 45. Van der Linden MH, Boer JM, Schneider P, et al. Clinical and molecular genetic characterization of wild-type MLL infant acute lymphoblastic leukemia identifies few recurrent abnormalities. Haematologica 2016;101:e95ee98. 46. Mansur MB, Emerenciano M, Splendore A, et al. T-cell lymphoblastic leukemia in early childhood presents NOTCH1 mutations and MLL rearrangements. Leuk Res 2010;34:483e486. 47. Mansur MB, van Delft FW, Colman SM, et al. Distinctive genotypes in infants with T-cell acute lymphoblastic leukaemia. Br J Haematol 2015;171:574e584. 48. Chaudhury SS, Morison JK, Gibson BES, et al. Insights into cell ontogeny, age, and acute myeloid leukemia. Exp Hematol 2015;43: 745e755. 49. Wiemels JL, Xiao Z, Buffler PA, et al. In utero origin of t(8;21) AML1-ETO translocations in childhood acute myeloid leukemia. Blood 2002;99:3801e3805. 50. Kelly LM, Gilliland DG. Genetics of myeloid leukemias. Annu Rev Genomics Hum Genet 2002;3:179e198. 605 51. Balgobind BV, Hollink IH, Arentsen-Peters ST, et al. Integrative analysis of type-I and type-II aberrations underscores the genetic heterogeneity of pediatric acute myeloid leukemia. Haematologica 2011;96:1478e1487. 52. Coser VM, Meyer C, Basegio R, et al. Nebulette is the second member of the nebulin family fused to the MLL gene in infant leukemia. Cancer Genet Cytogenet 2010;198:151e154. 53. Marschalek R. Mechanisms of leukemogenesis by MLL fusion proteins. Br J Haematol 2011;152:141e154. 54. Emerenciano M, Kowarz E, Karl K, et al. Functional analysis of the two reciprocal fusion genes MLL-NEBL and NEBL-MLL reveal their oncogenic potential. Cancer Lett 2013;332:30e34. 55. Emerenciano M, Meyer C, Macedo-Silva ML, et al. Backtracking to birth of the NUP98-HOXD13 gene fusion in an infant acute myeloid leukemia. Leukemia 2011;25:1192e1194. 56. Tosi S, Harbott J, Teigler-Schlegel A, et al. t(7;12)(q36;p13), a new recurrent translocation involving ETV6 in infant leukemia. Genes Chromosomes Cancer 2000;29:325e332. 57. Coenen EA, Zwaan CM, Reinhardt D, et al. Pediatric acute myeloid leukemia with t(8;16)(p11;p13), a distinct clinical and biological entity: a collaborative study by the International-Berlin-FrankfurtMunster AML-study group. Blood 2013;122:2704e2713. 58. Carroll A, Civin C, Schneider N, et al. The t(1;22) (p13;q13) is nonrandom and restricted to infants with acute megakaryoblastic leukemia: a Pediatric Oncology Group Study. Blood 1991;78:748e752. 59. Gruber TA, Gedman AL, Zhang J, et al. An Inv(16)(p13.3q24.3)encoded CBFA2T3-GLIS2 fusion protein defines an aggressive subtype of pediatric acute megakaryoblastic leukemia. Cancer Cell 2012;22:683e697. 60. Von Bergh AR, van Drunen E, van Wering ER, et al. High incidence of t(7;12)(q36;p13) in infant AML but not in infant ALL, with a dismal outcome and ectopic expression of HLXB9. Genes Chromosomes Cancer 2006;45:731e739. 61. Andrade FG, Noronha EP, Baseggio RM, et al. Identification of the MYST3-CREBBP fusion gene in infants with acute myeloid leukemia and hemophagocytosis. Rev Bras Hematol Hemoter 2016;38: 291e297. 62. Masetti R, Pigazzi M, Togni M, et al. CBFA2T3-GLIS2 fusion transcript is a novel common feature in pediatric, cytogenetically normal AML, not restricted to FAB M7 subtype. Blood 2013;121: 3469e3472. 63. Masetti R, Rondelli R, Fagioli F, et al. Infants with acute myeloid leukemia treated according to the Associazione Italiana di Ematologia e Oncologia Pediatrica 2002/01 protocol have an outcome comparable to that of older children. Haematologica 2014;99: e127ee129. 64. Andrade FG, Noronha EP, Brisson GD, et al. Molecular characterization of pediatric acute myeloid leukemia: results of a diagnostic and national multicentric study in Brazil. Arch Med Res 2016;47: 656e667. 65. Filiberto AC, Maccani MA, Koestler D, et al. Birthweight is associated with DNA promoter methylation of the glucocorticoid receptor in human placenta. Epigenetics 2011;6:566e572. 66. De Souza Reis R, de Camargo B, de Oliveira Santos M, et al. Childhood leukemia incidence in Brazil according to different geographical regions. Pediatr Blood Cancer 2011;56:58e64. 67. Alexander FE, Patheal SL, Biondi A, et al. Transplacental chemical exposure and risk of infant leukemia with MLL gene fusion. Cancer Res 2001;61:2542e2546. 68. Ross JA, Potter JD, Robison LL. Infant leukemia, topoisomerase II inhibitors, and the MLL gene. J Natl Cancer Inst 1994;86: 1678e1680. 69. Schnyder S, Du NT, Le HB, et al. Estrogen treatment induces MLL aberrations in human lymphoblastoid cells. Leuk Res 2009;33: 1400e1404. 606 Pombo-de-Oliveira and Andrade/ Archives of Medical Research 47 (2016) 593e606 70. Vanhees K, de Bock L, van Schooten FJ, et al. The role of estrogenic compounds in the etiology of pediatric leukemia. Leuk Res 2009;33: e210ee211. 71. Koifman S, Pombo-de-Oliveira MS. Brazilian Collaborative Study Group of Infant Acute Leukemia. High birth weight as an important risk factor for infant leukemia. Br J Cancer 2008;98:664e667. 72. Ferreira JD, Couto AC, Pombo-de-Oliveira MS, et al. In utero pesticide exposure and leukemia in Brazilian children less than 2 years of age. Environ Health Perspect 2012;121:269e275. 73. Kasat K, Go V, Pogo BG. Effects of pyrethroid insecticides and estrogen on WNT10B proto-oncogene expression. Environ Int 2002; 28:429e432. 74. Couto AC, Ferreira JD, Rosa AC, et al. Pregnancy, maternal exposure to hair dyes and hair straightening cosmetics, and early age leukemia. Chem Biol Interact 2013;205:46e52. 75. Ferreira JD, Couto AC, Pombo-de-Oliveira MS, et al. Pregnancy, maternal tobacco smoking, and early age leukemia in Brazil. Front Oncol 2012;2:151. 76. Ferreira JD, Couto AC, Emerenciano M, et al. Maternal alcohol consumption during pregnancy and early age leukemia risk in Brazil. Biomed Res Int 2015;2015:732495. 77. Chokkalingam AP, Buffler PA. Genetic susceptibility to childhood leukaemia. Radiat Prot Dosimetry 2008;132:119e129. 78. Brisson GD, Alves LR, Pombo-de-Oliveira MS. Genetic susceptibility in childhood acute leukaemias: a systematic review. Ecancermedicalscience 2015;9:539. 79. Bolufer P, Barragan E, Collado M, et al. Influence of genetic polymorphisms on the risk of developing leukemia and on disease progression. Leuk Res 2006;30:1471e1491. 80. Perera FP, Jedrychowski W, Rauh V, et al. Molecular epidemiologic research on the effects of environmental pollutants on the fetus. Environ Health Perspect 1999;107(Suppl 3):451e460. 81. Zanrosso CW, Emerenciano M, Gonçalves BA, et al. N-acetyltransferase 2 polymorphisms and susceptibility to infant leukemia with maternal exposure to dipyrone during pregnancy. Cancer Epidemiol Biomarkers Prev 2010;19:3037e3043. 82. Wiemels J. Perspectives on the causes of childhood leukemia. Chem Biol Interact 2012;196:59e67. 83. Inaba H, Greaves M, Mullighan CG. Acute lymphoblastic leukaemia. Lancet 2013;381:1943e1955. 84. Barletta E, Gorini G, Vineis P, et al. Ras gene mutations in patients with acute myeloid leukaemia and exposure to chemical agents. Carcinogenesis 2004;25:749e755. 85. Andrade FG, Furtado-Silva JM, Gonçalves BA, et al. RAS mutations in early age leukaemia modulated by NQO1 rs1800566 (C609T) are associated with second-hand smoking exposures. BMC Cancer 2014; 14:133. 86. Vasiliou V, Ross D, Nebert DW. Update of the NAD(P)H:quinone oxidoreductase (NQO) gene family. Hum Genomics 2006;2:329e335. 87. Smith MT, Wang Y, Skibola CF, et al. Low NAD(P)H:quinone oxidoreductase activity is associated with increased risk of leukemia with MLL translocations in infants and children. Blood 2002;100:4590e4593. 88. Costa LG, Cole TB, Vitalone A, et al. Measurement of paraoxonase (PON1) status as a potential biomarker of susceptibility to organophosphate toxicity. Clin Chim Acta 2005;352:37e47. 89. Huen K, Harley K, Brooks J, et al. Developmental changes in PON1 enzyme activity in young children and effects of PON1 polymorphisms. Environ Health Perspect 2009;117:1632e1638.