Pharmacology: Perfusion, Clotting, Fluid & Electrolyte
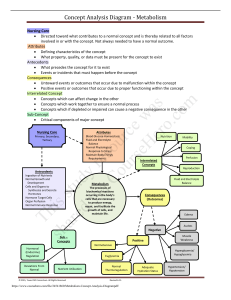
advertisement

1230 Pharmacology Perfusion, Clotting, Fluid and Electrolyte 1. Heart failure (HF) is when the heart muscle weakens and enlarges, losing the ability to pump blood through the heart and systemic circulation. 2. Common causes of HF include chronic HTN, myocardial infarction (MI), coronary artery disease (CAD), heart valve disease, congenital heart disease, and arteriosclerosis. 3. In left sided HF the left ventricle does not pump blood efficiently to the peripheral system causing blood to back up in the lungs, common symptoms include shortness of breath (SOB) and dyspnea. 4. In right sided HF the right ventricle does not pump blood efficiently to the lungs causing blood to back up in the peripheral system, common symptoms include peripheral edema. 5. Preload is blood flow force that stretches ventricle at the end of diastole. 6. Afterload is resistance to ventricular ejection of blood. 7. First line treatment for HF includes IV inotropes (dopamine, dobutamine), phosphodiesterase inhibitors (milrinone), oral diuretics, beta blockers, ACE, ARB, CCB, and vasodilators. 8. Nonpharmacological treatment of HF includes limit salt 2 g/day, 1 or less alcoholic drinks, stop smoking, fluid intake may be restricted, loss weight if needed, decrease saturated fat in diet, mild exercise recommended. 9. Cardiac glycosides, including digoxin, have three effects on the heart muscle inotropic (increase myocardial contraction), chronotropic (decrease HR), dromotropic (decrease conduction thru AV node). 10. Cardiac glycosides are also used to treat atrial fibrillation/flutter. 11. Atrial natriuretic hormone/peptide (ANH pr ANP) released during expansion and filling of atria produce vasodilation and increased GFR resulting in increased urine production and decreased blood volume and pressure. 12. Brain natriuretic peptide (BNP) released from atrial cardiac cells and aids in diagnosis of HF. Digoxin/Cardiac Glycoside Concept/Action/Use Assessment Patient Nursing Interventions/Patient Problem/Planning Teaching Evaluation Perfusion Inhibits sodiumpotassium ATPase promoting increased force of contraction, cardiac output, and tissue perfusion. Decreases ventricular rate. Heart failure atrial fibrillation atrial flutter Ischemia, decreased tissue perfusion, decreased gas exchange, hypoxemia. Patient will demo pulse check, range for pulse, know high potassium foods. Pulse in expected range, decreased heart rate and lung congestion, absence of digoxin toxicity. Digoxin therapeutic range 0.8 – 2 ng/mL Drug/herb history Baseline apical pulse Assess signs and symptoms digoxin toxicity Apical pulse rate below 60 do not administer. The patient will check pulse rate daily before taking digoxin. Ascertain apical pulse rate before administering digoxin. Assess for evidence of digitalis toxicity. Determine signs of peripheral and pulmonary edema. Monitor serum digoxin level. Monitor serum potassium level and report signs and 1230 Pharmacology Perfusion, Clotting, Fluid and Electrolyte symptoms low potassium level weakness, fatigue, abdominal distention, nausea, vomiting, leg cramps. Instruct patient to report symptoms digoxin toxicity loss of appetite, vomiting, diarrhea blurred vision, green or yellow halos, low heart rate, palpitations, or irregular heart rate. 13. Digitalis toxicity signs and symptoms include anorexia, vomiting, diarrhea, blurred vision, green or yellow halos bradycardia, premature ventricular contractions, cardiac dysrhythmias 14. Digoxin cardiotoxicity can cause ventricular dysrhythmias that can be treated with phenytoin and lidocaine. 15. The antidote for digitalis toxicity is digoxin immune fab. 16. Hypokalemia can increase digoxin effects and result in an increased risk for digitalis toxicity. 17. Phosphodiesterase inhibitors are a positive inotropic group of drugs that result in myocardial contractility and vasodilation. 18. Other medications used in HF include vasodilators, ACE inhibitors, ARB’s, diuretics, nesiritide, and some beta blockers. 19. Antianginal medications are used to treat angina pectoris. 20. Define the following: a. Angina pectoris pain caused by inadequate blood flow to cardiac tissues. b. Classic (stable) angina pain with predictable stress or exertion c. Unstable angina progressively severe pain unrelated to activity, stress, exertion d. Variant (Prinzmetal or vasospastic) angina pain at rest 21. Nonpharmacological methods of treating angina include avoid heavy meals, smoking, extreme weather changes, strenuous exercise, emotional upset. Increase proper nutrition, moderate exercise, adequate rest, and relaxation techniques. 22. Three types of antianginal medications are nitrates, beta blocker and CCB. 23. Nitrates cause generalized vascular and coronary vasodilation. Nitroglycerin/Antianginal Concept/Action/Use Assessment Patient Nursing Interventions/Patient Problem/Planning Teaching Evaluation Perfusion Promote vasodilation. Decrease preload and afterload. Decrease tissue perfusion, hypoxemia, myocardial tissue Decreased anginal pain with medications. Note side effects dizziness, headache, faintness Baseline VS Health and drug history Do not abruptly discontinue. Monitor VS especially for hypotension. Position patient sitting or lying for first administration. 1230 Pharmacology Angina, AMI, HTN emergency, pulmonary edema, HF Perfusion, Clotting, Fluid and Electrolyte injury, anxiety, pain, dyspnea. Patient reports angina controlled with medication COP slowly. Dry mouth could interfere with SL absorption, sips of water may be needed. Gloves for ointments and watch when defibrillating, may cause burns. Protect medication from light. If angina not subsided or worse in 5 minutes call 911 SL tabs every 5 min X 3, seek medical attention if pain not relieved. Do not ingest alcohol with nitrates. Do not stop BB or CCB, withdrawal symptoms of tachycardia and pain may be severe. Avoid hairy and broken skin surfaces when applying nitroglycerine patches. May use acetaminophen for headache. 24. Beta Blockers decrease the effects of the sympathetic nervous system by blocking the action of catecholamines thereby decreasing HR and BP. 25. Calcium channel blockers (CCB) relax coronary artery spasms and peripheral arterioles decreasing cardiac O2 demand. 26. Cardiac dysrhythmia is defined as any deviation from normal rate and pattern of heartbeat. 27. In an ECG the P wave reflects atrial activation, the QRS reflects ventricular depolarization, and the T wave reflects ventricular repolarization. 28. When sodium and calcium enter cardiac cells depolarization or cardiac contraction occurs. 29. Four classes of antidysrhythmic are sodium channel blocker, beta blocker, drugs that prolong depolarization, and calcium channel blocker. 30. Sodium channel blocker decrease sodium influx into cardiac cells resulting in decreased conduction velocity, suppression of automaticity, and increased recovery time. 31. Beta1 blockers are cardioselective beta adrenergic blockers resulting in decreased conduction velocity, automaticity, and recovery time. 1230 Pharmacology Perfusion, Clotting, Fluid and Electrolyte Acebutolol hydrochloride/Antidysrhythmias Concept/Action/Use Assessment Patient Nursing Interventions/Patient Problem/Planning Teaching Evaluation Perfusion Block beta1 receptor sites Decrease conduction, velocity, automaticity, and recovery time. Treat premature ventricular contractions. Decreased tissue perfusion, hypoxemia, anxiety. Patient will be in normal sinus rhythm and comply with medication regimen. Evaluate for normal sinus rhythm, side effects and palpitations, shortness of breath, coughing and chest pain. Baseline VS & ECG. Health and drug history. Monitor cardiac enzymes Do not abruptly discontinue. Monitor VS especially for hypotension. Pt avoid alcohol increases hypotension, caffeine increases catecholamine levels, and tobacco causes vasoconstriction. Teach patient to take as prescribed. Teach patient to report side effects dizziness, faintness, nausea, and vomiting. Administer IV push as recommended in drug guide. 32. Calcium channel blockers (CCB) block calcium entry decreasing excitability and contractility. 33. Two purposes for diuretics are to decrease hypertension and edema (peripheral and pulmonary). 34. Five categories of diuretics are thiazide and thiazide-like diuretics, loop diuretics, osmotic diuretics, carbonic anhydrase inhibitors and potassium-sparing diuretics. 35. Thiazide diuretics act on the distal convoluted renal tubule. Hydrochlorothiazide/Thiazides Concept/Action/Use Assessment Patient Nursing Interventions/Patient Problem/Planning Teaching Evaluation Elimination. Act on distal convoluted renal tubule Promote sodium, potassium, and water excretion and act directly on arterioles to promote vasodilation. Elimination, fluid overload, abnormal electrolyte levels. Patient blood pressure will decrease and/or patient will have decreased edema. Patient will have normal electrolyte levels. Evaluate for decreased blood pressure, decreased edema, and normal electrolyte levels. Assess baseline vital signs, urine output, edema, serum electrolytes, glucose, and uric acid. Assess history of medications Assess vital signs, weight, urine output, and serum electrolytes and glucose values for baseline levels. Monitor K+ levels. Check extremities for edema. Observe for signs and symptoms of hypokalemia. Monitor the patient’s daily weight and urine output. Suggest that the patient take the drug early in the morning 1230 Pharmacology Hypertension, edema, heart failure, ascites, nephrotic syndrome. Perfusion, Clotting, Fluid and Electrolyte and herbal supplements. to avoid sleep disturbance from nocturia. Instruct patient to slowly change positions from lying to standing because dizziness may occur. Advise patient to use sunblock for photosensitivity. 36. Loop diuretics act on the thick ascending loop of Henle. Furosemide/Loop Diuretic Concept/Action/Use Assessment Patient Nursing Problem/Planning Interventions/Patient Teaching Assess baseline Elimination, fluid Monitor urinary output and vital signs, overload, weight to determine body urine output, abnormal fluid gain or loss. edema, and electrolyte levels. Monitor vital signs and note serum Patient blood decrease in BP. electrolytes. pressure will Administer IV furosemide Assess history decrease and/or slowly, hearing loss may of medications patient will have occur if it is rapidly injected. and herbal decreased Observe for evidence of supplements. edema. Patient hypokalemia (muscle Assess will have normal weakness, abdominal hypersensitivity electrolyte levels. distention, leg cramps to and/or cardiac sulfonamides. dysrhythmias. Monitor potassium levels, especially when a patient is taking digoxin. Suggest that the patient take the drug early in the morning to avoid sleep disturbance from nocturia. Instruct patient to slowly change positions from lying to standing because dizziness may occur. Evaluation Elimination Act on ascending loop of Henle Inhibit sodium, water reabsorption, increase potassium, chloride, calcium, magnesium excretion. Treat heart failure, renal dysfunction, HTN, nephrotic syndrome, acute pulmonary & peripheral edema. Evaluate for decreased blood pressure, decreased edema, and normal electrolyte levels. 37. Osmotic diuretics increase osmolality and sodium reabsorption and are used for kidney failure, decreased ICP and IOP. 38. Carbonic anhydrase inhibitors block the action of carbonic anhydrase and are primarily used for decreasing IOP with open angle glaucoma. 1230 Pharmacology Perfusion, Clotting, Fluid and Electrolyte 39. Potassium-sparing diuretics are weaker than thiazide and loop diuretics and act primarily in the collecting duct renal tubule. Spironolactone/Potassium-Sparing Diuretic Concept/Action/Use Assessment Patient Problem/Planning Nursing Interventions/Patient Teaching Elimination Assess Elimination, fluid Monitor urinary output. Block action of baseline vital overload, Record vital signs and report aldosterone to signs, urine abnormal abnormal changes. promote output, electrolyte levels. Observe for signs and sodium/water edema, and Patient blood symptoms of hyperkalemia excretion and serum pressure will (nausea, diarrhea, potassium electrolytes. decrease and/or abdominal cramping, leg retention. Treat Assess patient will have cramps, numbness and edema, HTN, heart history of decreased edema. tingling hands and feet, failure, medications Patient will have peaked T-wave, and hypokalemia, and herbal normal oliguria). hyperaldosteronism. supplements. electrolyte levels. Administer spironolactone in the morning to avoid nocturia. Advise patients with high serum potassium levels to avoid foods high in potassium. Evaluation Evaluate for decreased blood pressure, decreased edema, and normal electrolyte levels. 40. Hypertension (HTN) is an increase in BP above 140/90. 41. Nonpharmacological treatment of HTN include stress-reduction techniques, exercise, salt restriction, decreased alcohol ingestion, and smoking cessation. 42. Guidelines for HTN determination are set by joint national committee on prevention, detection, and reduction of high blood pressure (JNC 8, 2017). 43. Six categories of antihypertensives are diuretics, sympatholytic, direct-acting arteriole vasodilator, ACE inhibitor, ARB’s, and CCB. 44. Five categories of sympatholytic are beta adrenergic blocker, centrally acting alpha2 agonists, alpha adrenergic blocker, adrenergic neuron blocker, alpha 1 and beta1 blockers. 45. Beta-adrenergic blockers reduce cardiac output by diminishing the SNS response. Metoprolol/Beta Blocker Concept/Action/Use Assessment Perfusion Block beta1 receptor sites, Baseline VS. Health and drug history. Patient Nursing Problem/Planning Interventions/Patient Teaching Hypertension, Monitor vital signs. fatigue. Monitor laboratory results, especially BUN, Evaluation Evaluate for decreased blood pressure, and 1230 Pharmacology reduce cardiac output by diminishing sympathetic nervous system response. Treat heart failure, HTN, acute myocardial infarction, and angina. Monitor cardiac enzymes Perfusion, Clotting, Fluid and Electrolyte Patient will have decreased blood pressure and comply with medication regimen. serum creatinine, AST, and LDH. Do not abruptly stop taking beta blockers as rebound hypertension may result. Advise patients to avoid over-the-counter drugs without first checking with a health care provider. Advise patient to wear a medic alert. adherence to medication regimen. 46. Centrally acting alpha2 agonists decrease sympathetic activity, increase vagus activity, decrease cardiac output, and decrease serum epinephrine, norepinephrine and renin resulting in reduced peripheral vascular resistance and increased vasodilation. 47. Alpha-adrenergic blockers result in vasodilation and decreased blood pressure. Prazosin hydrochloride/Alpha-Adrenergic Blocker Concept/Action/Use Assessment Patient Nursing Interventions/Patient Problem/Planning Teaching Evaluation Perfusion Dilate peripheral blood vessels by blocking alpha1 adrenergic receptors. Treat hypertension. Hypertension, fatigue. Patient will have decreased blood pressure and comply with medication regimen. Evaluate for decreased blood pressure, and adherence to medication regimen. Baseline VS. Health and drug history. Monitor vital signs. Check daily for fluid retention in extremities and weight gain. Advise patients to comply with the drug regimen. Advise patient not to take OTC cough and cold medications without first contacting their provider. Inform patients that orthostatic hypotension may occur. Teach patient to monitor daily weights. 48. Adrenergic neuron blockers are potent antihypertensive that block the release of norepinephrine. 49. Alpha1 and Beta1 adrenergic blockers block both receptors and cause vasodilation which decreases resistance to blood flow. 1230 Pharmacology Perfusion, Clotting, Fluid and Electrolyte 50. Direct-acting arteriole vasodilators are potent antihypertensive by relax smooth muscle of the blood vessels. 51. Angiotensin-converting enzyme inhibitor (ACE) prevent the formation of angiotensin II and the release of aldosterone. 52. The primary SE of ACE inhibitor is constant irritated cough. 53. Angiotensin II receptor blocker (ARB) also prevent the release of aldosterone. Valsartan/Angiotensin ll-Receptor Blocker (ARB) Concept/Action/Use Assessment Patient Nursing Interventions/Patient Problem/Planning Teaching Evaluation Perfusion. Act on renin– angiotensin– aldosterone system Block angiotensin II and prevent release of aldosterone. Treat HTN and heart failure. Hypertension, fatigue. Patient will have decreased blood pressure and comply with medication regimen. Evaluate for decreased blood pressure, and adherence to medication regimen. Baseline VS. Health and drug history. Monitor vital signs. Check daily for fluid retention in extremities and weight gain. Advise patients to comply with the drug regimen. Inform patients that orthostatic hypotension may occur. Teach patient to monitor daily weights. Do not abruptly stop taking as rebound hypertension may result. Medication may cause harm to fetus. Dizziness and lightheadedness common during initial therapy. Monitor for angioedema. Teach patient to avoid foods high in potassium. 54. Direct renin inhibitors cause a reduction both angiotensin I and II and aldosterone. 55. CCB’s promote vasodilation. Amlodipine/Calcium Channel Blocker Concept/Action/Use Assessment Patient Nursing Interventions/Patient Problem/Planning Teaching Evaluation Perfusion Inhibits influx of calcium across vascular smooth muscle cell Hypertension, fatigue. Patient will have decreased blood pressure and Evaluate for decreased blood pressure, and adherence to medication regimen. Baseline VS. Health and drug history Monitor vital signs. Check daily for fluid retention in extremities and weight gain. 1230 Pharmacology membrane to promote vasodilation. Treat HTN and heart failure. Perfusion, Clotting, Fluid and Electrolyte comply with medication regimen. Advise patients to comply with the drug regimen. Inform patients that orthostatic hypotension may occur. Teach patient to monitor daily weights. Monitor for angioedema. Pt avoid alcohol increases hypotension, caffeine increases catecholamine levels, and tobacco causes vasoconstriction. 56. Define the following: a. Thrombus formation of a clot in a blood vessel b. Embolus a blood clot moving thru the bloodstream. c. Anticoagulants prevent formation of blood clot in circulation. d. Antiplatelet prevents platelet aggregation. e. Thrombolytic breaks up clots that have formed. 57. Anticoagulants help prevent venous problems deep venous thrombosis (DVT) and pulmonary embolism (PE) as well as arterial problems coronary thrombosis, myocardial infarction (MI), artificial cardiac valves, and cerebrovascular accident (CVA). Heparin/Anticoagulant Concept/Action/Use Assessment Patient Nursing Interventions/Patient Problem/Planning Teaching Evaluation Perfusion/Clotting Bind with antithrombin III Inhibit action of thrombin. Inhibit conversion of fibrinogen to fibrin. Inhibit clot formation. Prevent venous thrombosis. Bleeding, dehydration, tissue injury Patient’s PTT and aPTT will be in therapeutic range and patient free of side effects. History of bleeding disorders. Baseline VS. Health and drug history PTT and aPTT Monitor PTT and aPTT before administering heparin. Examine patient’s nose, mouth, skin (especially older patients), urine for bleeding. Check stool for occult blood. Keep antidote protamine sulfate on hand. Teach patient to inform dentist when taking an anticoagulant. Advise patient to use a soft toothbrush to prevent bleeding gums. 1230 Pharmacology Perfusion, Clotting, Fluid and Electrolyte Warfarin/Oral anticoagulant Concept/Action/Use Assessment Patient Nursing Interventions/Patient Problem/Planning Teaching Evaluation Perfusion/Clotting Inhibit clot formation. Inhibit hepatic synthesis of vitamin K, thus affecting the clotting factors II, VII, IX, and X Prevent venous thrombosis. Bleeding, dehydration, tissue injury Patient’s INR will be in therapeutic range (2-3) and patient free of side effects. History of bleeding disorders. Baseline VS. Health and drug history INR Monitor INR therapy. Examine patient’s nose, mouth, skin (especially older patients), urine for bleeding. Check stool for occult blood. Keep antidote Vitamin K on hand. May need Fresh Frozen Plasma for hemorrhage. Teach patient to inform dentist when taking an anticoagulant. Advise patient to use a soft toothbrush to prevent bleeding gums. Advise patient to use a safety razor. Advise patient to wear a medic alert tag. Advise patient to check with provider when using OTC medications and not to use aspirin, it will increase bleeding risk. Patient should eat consistent amounts of Vitamin K containing foods. Teach patient for any cut or injury apply direct pressure for a minimum of five to ten minutes with clean dry absorbent material. 58. Heparin increases clotting time by combining with antithrombin III and inactivating thrombin. 59. Lab test to monitor heparin is PTT and a PTT and the antidote for heparin is protamine sulfate. 60. Low molecular weight heparin (LMWH) produces more stable anticoagulant responses. 61. Oral anticoagulants inhibit hepatic synthesis of vitamin K. 1230 Pharmacology Perfusion, Clotting, Fluid and Electrolyte 62. Lab test to monitor warfarin is PT or INR and the antidote for warfarin is vitamin K. 63. Antiplatelets are used to prevent MI, stroke, and transient ischemic attack (TIA) Clopidogrel/Antiplatelet Concept/Action/Use Assessment Patient Nursing Interventions/Patient Problem/Planning Teaching Evaluation Perfusion/Clotting Suppress platelet aggregation. Prevent arterial thrombosis with unstable angina, AMI, stroke, TIA Bleeding, tissue injury Patient will be free of subsequent thromboembolism and without side effects. History of bleeding disorders. Baseline VS. Health and drug history May take with aspirin. Stop meds 7 days before surgery. Do not use with hx of peptic ulcer disorder, active bleeding, or intracranial hemorrhage. Ginger, garlic, ginkgo, feverfew, and green tea my increase bleeding. 64. Thromboembolism is occlusion of artery or vein that results in ischemia and necrosis. 65. Thrombolytics are used for AMI, PE, DVT, noncoronary arterial occlusion, and thrombolytic stroke. Alteplase/Thrombolytic Concept/Action/Use Assessment Patient Nursing Interventions/Patient Problem/Planning Teaching Evaluation Perfusion Bind to fibrin promoting conversion of plasminogen to plasmin which digests fibrin in a clot and degrades fibrinogen, prothrombin, and other clotting factors disintegrating clots. Disintegrate clots and restore perfusion due to AMI, PE, DVT, thrombolytic stroke Bleeding, tissue injury Clot dissolved and perfusion restored History of bleeding disorders. Baseline VS. Health and drug history Monitor vital signs, increased pulse and decreased BP may indicate hemorrhage and shock. VS every 15 min for first hour, every 30 min for 8 hours and then hourly for 24 hours total. Observe for signs and symptoms of active bleeding. Have antidote aminocaproic acid on hand. Observe for signs of allergic reaction to thrombolytics, itching, hives, flushing, fever, dyspnea, bronchospasm, hypotension, and/or cardiovascular collapse. Avoid administering aspirin or NSAIDs for pain or discomfort 1230 Pharmacology Perfusion, Clotting, Fluid and Electrolyte when receiving a thrombolytic. Monitor ECG for reperfusion or dysrhythmias. Avoid venipuncture/arterial sticks. 66. Define the following: a. Hyperlipidemia excess of one or more lipids in the blood stream b. High-density lipoprotein ‘good’ cholesterol, smallest and densest lipoprotein removes excess cholesterol from bloodstream. c. Low-density lipoprotein ‘bad’ cholesterol, 50-60% fat increases risk of CAD d. Very-low-density lipoprotein mostly triglycerides e. Chylomicrons large particles of fatty acids and cholesterol 67. Nonpharmacological cholesterol lowering methods include low fat diet, lean meat, lose weight, exercise, smoking cessation. 68. Antihyperlipidemic include five types of bile-acid sequestrants, fibrates, nicotinic acid, cholesterol absorption inhibitors, hepatic 3-hydroxy-3-methylglutaryl-coenzyme A (HMG-CoA) reductase inhibitors or statins. Atorvastatin/Antihyperlipidemic Concept/Action/Use Assessment Patient Nursing Interventions/Patient Problem/Planning Teaching Evaluation Perfusion Inhibit HMG-CoA reductase enzyme in the liver. Hyperlipidemia Ischemia, nausea, and vomiting, decreased visual acuity, hyperglycemia Patient cholesterol level will be within normal limits without side effects. Baseline VS Health and drug history Liver function. Monitor the patient’s blood lipid levels. Monitor lab values for liver function. Observe for signs and symptoms of GI upset. Emphasize drug compliance and inform patient that it may take several weeks before blood lipid levels decline. Instruct patient to have annual eye examinations and report changes in visual acuity. Encourage patient to report any unexplained muscle tenderness or weakness that may be caused by rhabdomyolysis. Do not stop abruptly, may cause serious rebound that 1230 Pharmacology Perfusion, Clotting, Fluid and Electrolyte could lead to acute myocardial infarction and possible death. 69. Peripheral arterial disease (PAD) is a form of peripheral vascular disease (PVD) characterized by numbness and coolness of extremities, claudication causes pain and weakness of a limb when walking and possible leg ulcers. Cilostazol/Vasodilator and antiplatelet Concept/Action/Use Assessment Patient Nursing Interventions/Patient Problem/Planning Teaching Evaluation Perfusion Causes peripheral vasodilation. Inhibits platelet aggregation. Peripheral vascular disease and intermittent claudication Ischemia, hypotension, discomfort, decreased visual acuity, hyperglycemia Improved perfusion in extremities with decreased pain without side effects. Baseline VS Health and drug history Signs and symptoms inadequate perfusion in extremities: pallor, pain, coldness in extremities Monitor vital signs, especially blood pressure and heart rate. Inform patient that a desired therapeutic response may take 1.5 to 3 months. Advise patient not to smoke (causes vasospasms) or ingest alcohol (increases hypotension). Encourage patient to change position slowly but frequently to avoid orthostatic hypotension. Instruct patient not to take aspirin or other salicylates as they may increase antiplatelet activity. Patient should report flushing, headaches, and dizziness. May be take with food of GI upset occurs. 70. Pentoxifylline is a hemorheological agent or blood viscosity reducer agent that improves microcirculation and tissue perfusion in patients with intermittent claudication or Buergers disease. 71. Intracellular fluid (ICF) is fluid inside the cells. 72. Extracellular fluid (ECF) is fluid outside the cell, interstitial, intravascular and transcellular. 1230 Pharmacology Perfusion, Clotting, Fluid and Electrolyte 73. The major intracellular cation is potassium. 74. The major extracellular cation is sodium. 75. Define the following: a. Osmosis movement of water across a semipermeable membrane from low concentration to high concentration b. Diffusion movement of molecules from low concentration to high concentration c. Hydrostatic pressure force of fluid within a compartment d. Osmolality number of particles dissolved in serum. e. Active transport needs energy to move substances across cell membrane. f. Tonicity measurement of the concentration of IVF g. Isotonic approximately same osmolality as ECF or plasma (fluid replacement stays in vascular space) h. Hypotonic less osmotic pressure than ECF (moves fluid into cells) i. Hypertonic greater osmotic pressure than ECF (moves fluid out of cells and into vascular system) j. Crystalloid solution of fluid and electrolytes that move across capillary walls. k. Colloid solution contains protein or large molecules that increase oncotic pressure and pull fluid into vascular system. 76. Potassium is essential for electrical activity and muscle contraction. 77. Signs and symptoms of hypokalemia fatigue, muscle weakness, anorexia, N/V severe: paresthesia, leg cramps, confusion rhabdomyolysis, myoglobinuria, ventricular dysrhythmias, cardiac arrest, flat or inverted T-waves. 78. Signs and symptoms hyperkalemia cardiac dysrhythmias, tachycardia followed by bradycardia, paresthesia of face tongue hands and feet, nausea, diarrhea, abdominal cramping. Potassium Concept/Action/Use Assessment Patient Nursing Interventions/Patient Problem/Planning Teaching Evaluation Electrolyte balance Nerve conduction and muscle contraction Correction of potassium deficit Hypokalemia Fluid imbalance K+ level will normalize with normal ECG and without side effects. Baseline VS Health and drug history If patient is on digoxin check for digoxin toxicity (low K+ levels enhance the action of digoxin). Signs and symptoms hypokalemia Give oral K+ with at least 8 oz water or juice. Administer K+ containing IV solutions via a calibrated infusion pump. Monitor ECG during infusions. IV K+ must be diluted with 100 to 1000 mL and infused at a rate of no more than 10 mEq per hour. Never give K+ IM, IV push or IV bolus: rapid infusion may result in cardiac arrest. 1230 Pharmacology Perfusion, Clotting, Fluid and Electrolyte and hyperkalemia Monitor renal function and urine output, below 25 mL per hr may lead to hyperkalemia. Monitor IV site closely, infiltration may lead to tissue necrosis. Monitor K+ levels frequently. Monitor and teach patient sings and symptoms hypokalemia nausea and vomiting, polyuria, abdominal distention, muscle weakness, cardiac dysrhythmias. Monitor and teach patient hyperkalemia oliguria, abdominal cramps, tachycardia, nausea, numbness tingling in extremities. Teach patient K+ in diet. 79. Sodium plays a major role in fluid volume balance and plasma osmolality. 80. Signs and symptoms hyponatremia muscle weakness, decreased DTR, headache, lethargy, confusion, seizures, coma abdominal cramps, N/V, tachycardia pale skin hypotension. 81. Signs and symptoms hypernatremia dry sticky mucous membranes flushed dry skin, agitation increased body temp, dry tongue, N/V, anorexia, tachycardia, hypertension, muscle twitching, hyperreflexia, seizures coma. 82. Calcium promotes nerve and muscle contraction. 83. Signs and symptoms of hypocalcemia anxiety irritability, tetany, hyperactive DTR, spasms hands, wrists, feet, ankles, positive Chvostek’s and Trousseau, laryngeal spams, cardiac dysrhythmias. 84. Signs and symptoms hypercalcemia fatigue, muscle weakness, depressed DTR, confusion, memory impairment, anorexia, N/V constipation kidney stones. Intravenous Calcium Concept/Action/Use Assessment Patient Nursing Interventions/Patient Problem/Planning Teaching Evaluation Electrolyte balance. Weight loss, decreased sensation in Calcium level will normalize with Baseline VS Health and drug history Monitor serum total calcium and ionized calcium levels. 1230 Pharmacology Nerve conduction and muscle contraction Calcium deficit Perfusion, Clotting, Fluid and Electrolyte Assess for signs and symptoms hypocalcemia and hypercalcemia Assess for low albumin levels which decrease total calcium levels. If patient is on digoxin, elevated calcium levels can enhance digoxin action. upper extremities, reduced motor function Monitor vital signs and report abnormal findings. Monitor IV closely IV infiltration can cause tissue necrosis. Monitor ECG during IV infusions. Calcium chloride concentrations greater than 20 mg per mL should be given in a central line and at a rate of no more than 1 mg per 10 minutes. Check for IV compatible solutions, NS, D5W and D10W. Oral forms need Vit D and should be taken with meals to reduce GI distress. Chronic use of calcium antacids can cause constipation. Monitor and teach patients signs and symptoms hypocalcemia tetany, muscle cramps, numbness and tingling hands and feet, bleeding and cardiac dysrhythmias. Monitor and teach patient signs and symptoms of hypercalcemia flabby muscles, pain over bony areas, kidney stones normal ECG and without side effects. 85. Magnesium promotes transmission of neuromuscular impulses. 86. Signs and symptoms of hypomagnesaemia tetany like hyperexcitability ventricular tachycardia, Vfib and hypertension. 87. Signs and symptoms hypermagnesemia lethargy, drowsiness, weakness, paralysis, loss of DTR, hypotension, heart block. 88. Chloride is a major contributor to acid-base balance. 89. Signs and symptoms of hypochloremia tremors, twitching slow shallow breathing. 90. Signs and symptoms of hyperchloremia weakness lethargy deep rapid breathing unconsciousness. 91. Phosphorus is essential in bone and teeth formation and neuromuscular activity. 1230 Pharmacology Perfusion, Clotting, Fluid and Electrolyte 92. Signs and symptoms of hypophosphatemia fatigue, muscle weakness, depressed DTR, confusion, hyperventilation, anorexia, N/V constipation 93. Signs and symptoms hyperphosphatemia tetany, hyperactive DTR, spasms hands, wrists, feet, ankles, positive Chvostek’s and Trousseau, tachycardia nausea diarrhea abdominal cramps. References McCuistion, L. E., Vuljoin-DiMaggio, K., Winton, M. B., & Yeager, J. J. (2021). Pharmacology (10th ed.). St Louis, MO: Elsevier.