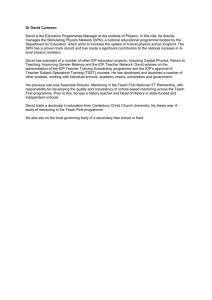
Electrolyte Imbalance Hypernatremia Lab Values Common Causes > 145 mEq/L Clinical Manifestations Nursing Management Thirst, tachycardia, orthostatic hypotension, decreased absent DTR, seizures, coma Cushing’s Hyponatremia Seizures, convulsions, and death Maintain airway, monitor VS, seizure precautions, monitor level of consciousness Coma, seizures, respiratory arrest < 136 Associated with heart failure Hyperkalemia >5.0 Increased risk of cardiac arrest Rare w normal kidney fx Associated with diabetic ketoacidosis Hypokalemia <3.5 Overuse of diuretics, increased aldosterone, NG tube K+ POTASIUM Excess potassium loss through the kidneys is often caused by such meds as corticosteroids, potassium-wasting diuretics, amphotericin B, & large doses of some antibiotics. Vs: slow, irreg pulse Muscle weakness, paresthesia, paralysis, Cardiac dysrhythmias, premature ventricular contraction, ventricular fib, peaked t waves, widened qrs Hyperactive bowel sounds Oliguria Metabolic acidosis Vs: decreased bp, orthostatic hypotension Neuro: altered mental status acute confusion and coma Flattened T wave, elevated U wave, ST depression, prolonged PR interval Hypoactive bowel sounds, paralytic ileus reduced DTR Respiratory failure, cardiac arrest weak and irregular pulse, muscle weakness, fatigue, and ventricular dysrhythmias. Prevent falls, assess for cardiac complications Calcium gluconate, dialysis Admin iv with dextrose and regular insulin Admin sodium bicarbonate to reverse acidosis Fall precautions due to muscle weakness IV K supplementation Food’s high in K = avocados, broccoli, dairy, dried fruit, cantaloupe, bananas, whole grains Hypercalcemia >10.5 Hyperparathyroidism Bone pain, fatigue, weakness, lethargic Ca CALCIUM Hypocalcemia <9.0 Tetany, positive Chvostek’s and Trousseau’s thyroidectomy Hyperphosphatemia >4.5 Hypophosphatemia <3.0 Hypermagnesemia >2.1 Hypomagnesemia <1.3 Hypocalcemia doesn't commonly have symptoms. Pts may exhibit tingling of the face, hands and feet and have a "pins and needles" sensation Think of hypocalcemia Elevations in magnesium levels are accompanied by hypotension, nausea, vomiting & facial flushing. Celiac or Crohn’s Chronic alcoholism Sim to hypocalcemia The treatment of hypocalcemia includes the monitoring of the client's respiratory and cardiac status in addition to providing the client with calcium supplements coupled with vitamin D because vitamin D is necessary for the absorption of calcium. Objectives Describe the role of Sodium (Na), potassium (K), Magnesium (Mg), Calcium (Ca), and Phosphate (PO4) Define hypervolemia and hypovolemia imbalances Discuss the use of Potassium and Magnesium replacement orders. Explain the use of Diuretics and impact on blood electrolytes Give examples of foods high in K, Na, Mg, Ca, PSO4 Identify nursing interventions for early signs and symptoms of potentially life-threatening imbalances in fluids and electrolytes Discuss the role of delirium in the patient with electrolyte imbalances TABLE 16.3 Extracellular Fluid Imbalances Causes and Manifestations ECF Volume Deficit ECF Volume Excess Causes • ↑ Insensible water loss or perspiration (high fever, heatstroke) • Diabetes insipidus • Osmotic diuresis • Hemorrhage • GI losses: vomiting, NG suction, diarrhea, fistula drainage • Overuse of diuretics • Inadequate fluid intake • Third-space fluid shifts: burns, pancreatitis Manifestations • Excess isotonic or hypotonic IV fluids • Heart failure • Renal failure • Primary polydipsia • SIADH • Cushing syndrome • Long-term use of corticosteroids ECF Volume Deficit • Restlessness, drowsiness, lethargy, confusion • Thirst, dry mucous membranes • Cold clammy skin • Decreased skin turgor, ↓ capillary refill • Postural hypotension, ↑ pulse, ↓ CVP • ↓ Urine output, concentrated urine • ↑ Respiratory rate • Weakness, dizziness • Weight loss • Seizures, coma ECF Volume Excess • Headache, confusion, lethargy • Peripheral edema • Jugular venous distention • S3 heart sound • Bounding pulse, ↑ BP, ↑ CVP • Polyuria (with normal renal function) • Dyspnea, crackles, pulmonary edema • Muscle spasms • Weight gain • Seizures, coma A pt is receiving intravenous fluids postoperatively following cardiac surgery. Nursing assessments should focus on which postoperative complication? Antidiuretic hormone & aldosterone levels are commonly increased following the stress response before, during, & immediately after surgery. This increase leads to sodium & water retention. Adding more fluids intravenously can cause a fluid volume excess & stress upon the heart & circulatory system. GERD – caffeine, smoking, AAA – worried about rupture – to prevent control BP to prevent rupture. If intact = no s/s. if dissecting aneurism = sharp severe pain with sudden onset, priority to get them to surgery asap bc hemorrhage Obstructed bile duct – stateroeah (fatty stools bc bile can’t get out to emulsify fats leading to incomplete digestion) HYPOvalumia = concern for hypoperfusion, BP < 90 (systolic), CAD – RF smoking, family history, age, gender, HTC (modifiable) Hypertension and hyperlipemia) Cataracts – blurred vision and photophobia Ulcerative colitis and Crohn’s disease – NPO to let things calm down, Complications – nutritional issue not met, fistulas (opening or tunnel where there shouldn’t be one), Constipation – assess for paralytic ileus listen to bowel sounds HYPO below obstructions HYPER above obstruction To prevent constipation pt edu : drink 2-3 L, eat high fiber foods – raw green vegetables, HYPOkalemia – diuretics, NG tube, S/S: cardiac disturbances MONITOR FOR CARDIAC ARRYTHMIAS Muscle cramps, taking Lasix, complain of cramps – check potassium levels DVT – lovonox, complication pulmonary embolism, Fluid overload – pitting edema, crackles in lung sounds, can indicate pulmonary edema, bc can interfere with oxygenation Glaucoma – increase ocular pressure of optic nerve can cause blindness, NOT curable or reversible DASH diet and DASH friendly foods Know normal for electrolytes Coosysectomy where we remove the gallbladder can be done laparoscopically or via open inscention REVIEW POST OP RESTRICTIONS To improve communication with pt with hearing loss – slowly but norm, min background noise, eye contact, Nitroglycerin – vasodilator of blood vessels that perfuse the heart. Under tongue. If still pain after 3 doses, call 911. 3 tabs every 5 minutes, call ems after 3rd MONA – chest pain: morphine, O2 to improve oxygenation, nitro, aspirin to prevent platelet aggregation (not EC) Post of complication – adolectis risk of pneumonia, to prevent this encourage early ambulation and incentive spirometry, big deep breaths, cough, frequent turn, deep breath q 2 hours; dvt why lovonox and emphasize early ambulation PAD vs PVD PAD – pain with walking (intermittent claudation), legs will be shiny, pale, loss of hair, limb ischemia PVD – edema, calf pain, red, ulcers with heavy weepy drainage, Stop smoking, get good nutrition, Stable angina – predictably chest pain provoked by known cause like mowing the lawn causes pain relieved with rest and or nitro s/s that it had progressed to unstable angina – unpredictable, can occur at rest or night time, may or may not be relieved by nitro, can increase in frequency and severity of pain Practice1 Review Glaucoma increased iop leading to optic nerve damage and the number 1 cause of blindness – Symptoms of cataracts include painless blurred vision and a decrease in the ability to perceive colors. AT1 Exam 2 mod 7 and 8 Visual Problems (21) Diff between astigmatism and myopia, etc. Visual impairment what is your job – emotional support, GOAL is promote safety and fx abilities How do you handle a pt that is blind always walk ahead and let them grab by the arm to the side of the client ELDERLY – risk for falls = full precautions, confusion, disorientation What do you do? Chemical = continuous eye irrigation with iv tube or morgan lens; penetrate object=cover both eyes=eye shield and then go to ER Intraocular disorders Macular degeneration – central loss of vision Cataract – opacity of the lens, develops over time, if untreated it’s the number 1 cause of blindness; decreased visual acuity, painless loss of vision; photosensitivity; halo around lights; absent red reflex (can be tumor also) risk factors – diabetes, older, Prescription glasses, avoid night, Surgery – pre op: mydriatic (pupil dilation )or cycloplegic agent, NSAIDs, topical antibiotics, anxiety meds Post op avoid increases in IOP photophobia; wear eye patch (risk for falls) until doctor again, pain that doesn’t go away with meds or Decrease IOP - don’t bend over waist; avoid sneezing, cough, strain; hyperflexion of head, titling head back to wash hair, limit housework and rapid jerky movements at least for a month after surgery. Vitamin C and E good *GLAUCOMA increase in IOP related to problem with optical nerve. TREATABLE BUT NO CURE. IOP NORMAL 10-21 MM HG OPEN ANGLE MILD PAIN AND GRADUAL LOSS OF PERPHERAL VISION (TUNNEL vision) POAG Abnormal IOP between 22-32 mm Hg; drop therapy Closed angle: sudden, EXTREME pain “extreme, severe, sudden” Acute, medical emergency Severe pain Caused by Blurry vision or halos N&V bc of pain Iop > 30 mm Hg MGMT chronic (open) meds can slower progression How do you help prevent glaucoma – early detection HOW DO YOU TEACH YOUR PT TO PREVENT GLACOM? - tell them to get eye exams 2-4 if 40-64; if >65 eye exam q 1-2 yrs Retinopathy - ,.. What stage of hypertension Why? Secondary –acute kidney disease causes PRIMARY HYPERTENSIN es or idiopathic (African American) persistent increased SVR (systemic vascular resistance) most common – who has it? CAUSES – soda = stress, smoking, sedentary life; obesity, oral contraceptives; diet high sodium high cholesterol, diseases DM, renal disease, HF, Hyperlipidemia; A – African men and age CHAPTER 37 Vascular disorder Arteries – peripheral artery disease – progressive narrow and degeneration of arties in bilateral upper and lower extremities. r/f: smoking, CKD, HTN, Hyper lipidemia S/S: PAD =ARTS (absent pulses, absent hair=cool legs, round red sores (blood pooling), toes and feet pale or black (eschar), sharp calf pain (intermittent claudication) PVD s/s VEINY Compression socks for PVD Pt edu – positioning pvd veins=elevate Constriction Cross legs Constrictive clothing Cigarettes Caffeine Cold temp Toenails trimmed only by dr. Xxxxxxcc FLUID BALANCE Monitor level of consisnes no matter Calcium 9.0-10 Hypocalcemia – trousseau and chovkes ii DTR assessment Hypervolemia – pulmonary edema; I Hypovolemia – low BP Test Review GI System – endoscopy known what this is Endoscopy: EGD Vegan diet – supplements Types of nutrition – oral, enteral, parenteral PAD – problem not enough blood No hair, complain of muscle aches, foot and hands are cold and blue and pale, ulcers, nails are thick and brittle, cold why does a person have DVT? DVT - Impaired flowing, thrombosis, ephitalial damage hyper coagulable states --> clot can dislodge and go to lungs are cause pulmonary edema or to brain=stroke PVD – edema in the legs, normal pulse, no sores no pain, pain with standing, hyperpigmentation, huge veins, warm, POOLING OF BLOOD TOO MUCH compression socks, legs up to increase venous return, NO MASAGE if known clot they should be on bed rest and encourage to elevate legs IF SOB AND SHARP CHEST PAIN and (unilateral leg) one sided pain likely pulmonary edema and must contact provider Strider, sternal retraction, use of accessory muscles are signs of respiratory failure (Calcium effects muscle) exam 2 on March 9th Adult Theory DIGESTIVE SYSTEM diff between upper and lower GI and know the organs in each Assessment Objective data Gerontological considerations Decrease appetite; carries, periodontal disease; diminished taste buds; lesee sense of smell; decreased saliva production More susceptible to dehydration Dx studies for GI system Know what do you teach – mri, endoscopy, GI SERIES – issues with the upper GI Drink barium Prep pts with clear liquid diet 1 day before the exam; NPO after midnight; increase fluid intake to flush out barium, stools will be white for 24-72 hours Endoscopy Bowel prep and NPO; Chapter 39 Diets – lacto ovo vegetarian, etc. What do you have to teach a person that wants to be a vegetarian – have to have more vitamins and teach them to eat proteins Vegans – lack B12 Therapeutic communication on diet Malnutrition Under or over nutrition than body requirements Nursing assessment – refer to dietitian Nursing DX: imbalanced nutrition, self-care deficit, deficient fluid volume, risk for impaired skin integrity (albumin know levels according to Lewis), activity intolerance; GOALS ideal body weight, consume specified number of calories, have no adverse consequences Postoperative diet progression Clear liquids, full liquids, soft diet, reg diet Types of nutrition support – oral feeding (PO); enteral nutrition (doff hob tube and goes through your mouth, using stomach; more safe; promotes healthy bowel; 30-45 degree head of bed to prevent aspiration; how to check proper placement of tube –> x-ray bc want to make sure not in lungs; HOB>30; FLUSH TO MAINTAIN PATENCY IF MEDS (10CC before and after); check position on insertion and before feeding --> before you flush, aspirate to make sure in stomach; PRIORTY IS MONITORING FOR ASPIRATION and nutrition status (sugar level checks every 6 hours bc at risk for hyperglycemia); parenteral nutrition (PEG tube goes more risk of infection; right into blood; TPN; use nasogastric tube for decompression of the stomach; BIGGEST disadvantage is that you are not using your bowels; IF FINISHES A BAG AND NEXT ONE IS NOT READY – HANG 10% DEXTROSE IN WATER TO PREVENT HYPOGLYCEMIA; never do meds) UlCertive colitis – left lower quadrant GERD – obesity is number 1 cause; nursing interventions: assess resp changes, edu diff between angina s/s and GERD, assess ability to swallow and gag reflex GERD know well; N&V notice how to assess, know Zofran; nutrition focus; Metabolic syndrome N & V complication = aspirations Ileostomies and colostomies – avoid gas causing foods – beans, eggs, carbonates beverages; stomal blockage – nuts, raw carrots, popcorn; odor – eggs, fish, garlic Cholecystitis – inflammation of the gallbladder Pain and tenderness in UR pain can radiate to R shoulder Cataracts S/S change in vision; worse at night; blurred vision; white color pupil Goals: educate them to min anxiety; prevent infection/complication Treatment: varies on severity; optimize lighting; change prescription; surgical removal of clouded lens Post-op prevents increased ocular pressure (IOP- coughing, bending down, vomiting increases); no rubbing eyes; wear sunglasses; report purulent draining (signs of infection); avoid activities that increase IOP; 4-6 weeks to completely heal; report changes in vision immediately; Complications of cataract – infection and bleeding PROVIDE PT EDU Eval – improved vision, control pain, better at ADLS Age related macular degeneration – loss of central vision, exact etiology unknown; ppl >60 y.o. Exudative (wet) vs nonexudative (dry) MOST COMMON dry; MOST SERIOUS wet Risk factors – age, genetics in families, smoking, uncontrolled hypertension, females Vision loss is not reversible but don’t tell pts that nothing can be done Glaucoma damage to optic nerve due to increased IOP or due to decrease fluid drainage or overproduction of fluid secretion = increase in IOP Normal IOP range 10-21 mmHg POAG – open-angle gradual onset; HA, loss of peripheral vision, IOP>21; ACG – closed-angle sudden onset, medical emergency, rapid onset IOP>30 mmHg, loss of PERLA, photophobia; sudden any symptoms immediately notify provider Risk factors – age, diabetes, uncontrol hypertension Hearing loss in elderly can lead to cognitive deficient cardiac output --- decreased cardiac output = decreased Table 32-2 in txt bk Normal SBP <120 and <80 Elevated 120-129 and HIGH SALT INTAKE 32-2 Water follows sodium --> eat salt = retain water = increase BP emphasize low sdum diet for pt. with hyper tension Clinical manifestations of hypertension would you asses? BP. Asymptomatic until severe and target organ disease occurs fatigue, dizziness, HA, etc. COMPLICATIONS target organ diseases occur most frequently in heart, brain, (Left ventricular hypertrophy: heart muscle thickens in left ventricle --> when heart is relaxing it can’t fill up with much blood bc not enough room so then not perfusing significant blood Peripheral vascular disease Kidney and eye damage Diagnostic studies – ECG, chest x-ray for cardio myopathy, screen for diabetes (blood glucose), CMP ESTABLISH BASELINE BP BEFORE STARTING THERAPY For pts with high BP – low salt, DASH diet GOALS – achieve and maintain goal BP Hydrochlorothiazide – diuretic, take in am not pm (so no night peeing), increase fluids and low sodium, orthostatic hypotension can occur ANTI-HYPERTENSIVES – exam won’t cover meds Assess orthostatic abnormal SBP decrease 20 mm Hg or more INCREASED RISK OF FALLS Nursing implementation: watch fluid, VS, dietician and physical therapist Home BP monitoring teaching Reason for poor adherence – unpleasant side effects of drugs so edu in advance to avoid or we can switch them; high cost/lack of insurance; To increase compliance – educate about risks and complications How do we know drug therapy is working? - BP down compared to baseline, BUN and creatinine improved, weight loss, RISK FACTORS AND WHO WOULD BE MOST AT RISK – SMOKING Chapter 33 CAD & Angina CAD coronary artery disease type of blood vessel disorder Cardio exercise is important bc promote collateral circulation in case of vessel occlusion RF: modifiable and nonmodifiable – focus on mod ones like HDL, LDL, smoking, obesity, etc. Risk factors for CAD that increase workload of heart and demand for O2, Health promo – id high-risk person – health hx, fam hx, lifestyle, precense of cardio symptoms DRUG THERAPY Lipid-lowering (statins = first line; inhibit cholesterol synthesis, decrease ldl, increase hdl, and lower crp); Rosuvastatin (Crestor) most potent, serious adverse effects (rare): liver damage and myalgia (CK-MM) and muscle cramps Chronic Stable Angina Chronic and progressive, asymp or chest pain, occurs when o2 demand of heart outweighs O2 supply; 2 types (stable vs unstable; ONLY STABLE FOR THIS TEST) S/S: chest pain with predictable pattern (ie during same activities, relieved by rest or nitroglycerin) Goal: reduce O2 demand or increase supply to help optimize myocardial profusion Nitrates – causes vasodilation Ace inhibit, beta (decrease heart rate), calcium channel Sit upright, give O2, get 12 lead ekg to rule out mycard infarction, assess VS, heart and breath sounds PT EDU reducing risk factors – low sodium diet and physical activity; meds nitrates or baby aspirin; ADMI NITROGLYCERIN 1 tab odt, 1 q 5 minutes up to 3 doses, if still pain --> call 911 bc could be heart attack may cause: HA, dizziness, flushing, orthostat; can be used prophylactically DX: 12 lead, labs, echo, exercise stress test Gold standard to dx and id CAD that can cause stable angina: is cardiac catheterization (procedure) to identify and localize CAD Stable angina occurs in a predictable pattern and be familiar with nitroglycerin teaching points. Table 37.1 PAD thickened walls --> decreased profusion --> so loss of hair, etc. PAD intermittent claudication or rest pain in foot PVD no pain but heaviness in lower extremities venous insufficiency (venous statis in lower extremities) Fluid and electrolytes Water maintains of blood volume transport of glucose waste, 2/3 intracellular and 1/3 extracellular Intracellular = potassium an magnesium Inter = sodium and chloride H, na, k, mg, ca + cl, s, phosphate, bicarbonate Number measure what's in ECF Mg 1.5-2.5 Phosphorus 2.5-4.5 K 3.5 - 5 Ca++ 8.5-10.5 Cl- 95-105 Na+ 135-145 mmEq/L Mg+ intracellular cation hypermagneisea = muscle relaxation Hypomagnesaemia = muscles are excited K intracellular cation – intracellular excitation Hyperkalemia > 5.0 tall peaked t waves Muscle twitching/ cramps (early) Muscle weakness/paralysis (late) Cardiac dysrhythmias Caused by k sparing diuretics HYPOkalemia <3.5 result of body fluid loss or diuretics Cells cannot repolarize causes spasms and legs cramps Bradycardia Flatten t wave Ca+ 8.5 -10.5 mg/dL Decreased albumin (made in liver) Motor neuron excitability HYPERcalcemia – decreased muscle contraction HYPOcalcemia – trousseaus sign and Chvostek's sign HYPERcalcemia – decreased DTRs, bone pain, dysthymias, cardiac monitoring loop diuretic=s to promote calcium excretion NA extracellular excitation Water follows sodium Hyponatremia more water than sodium caused by CHF HYPERnatremia Too much sodium not enough water s/s thirst dry mucus membranes edema diminished cardio output Correction and management of underlying causes GERD avoid – fatty foods, caffeine, chocolate, alcohol, smoking, nicotine, peppermint, and spearmint