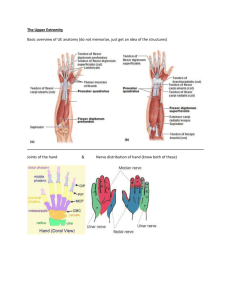
DR. CHOWN SPRING 2022 Midterm Study Guide OT 590: Clinical Competency WEEK 1: RANGE OF MOTION & GONIOMETRY OF THE UE EVALUATION • First, check orders to see what type of motion is allowed (i.e. AROM, PROM, AAROM). • Next, if cleared for range of motion (ROM), recommend AROM before PROM to gauge how far the client can move independently. TYPES OF ROM • AROM • PROM • Observe for compensatory movements • Tone • Check for coordination • Guarding • Motivation • Pain • Pain • Crepitus • Position and stabilize the joint correctly ERROR REDUCTION • The same goniometer should always be used to reduce the chances of instrumental error • Move a body part through its appropriate ROM • Determine the joint's end of the range of motion and end-feel • Palpate the appropriate bony landmarks • Align the goniometer with the landmarks • Read the measuring instrument properly • Record measurements correctly (both active and passive range of motion should be measured and recorded respectively).[1] • The range of motion of each joint should be measured in isolation, to avoid trick movement (simultaneous movement of another joint) and muscle insufficiency which may alter the reading. FACTORS THAT MAY AFFECT ROM OUTCOMES Edema Pain Adhesions Capsular tightness or laxity Tendon excursion Strength deficits FACTORS THAT IMPACT RELIABILITY Size and design of goniometer Type of ROM Amount of force applied Method of documentation (time during day, positive and negative numbers) Placement of goniometer FREQUENCY OF TEST ADMINISTRATION • American Society of Hand Therapists (ASHT) endorses American Medical Association's (AMA) use of plus and minus signs • + is equal to hyperextension, surplus • - is for extension lag, lagging or missing extension • Total Active Motion (TAM) – Sum of active MCP, PIP, and DIP arc of motion in degrees of an individual digit. 1. Subtract total active flexion (TAF) of the MP, PIP, and DIP joints from the total extension (TAF) deficit of the same joints in unaffected and affected hand. 2. Calculate TAM% by dividing the TAM of the injured finger by the TAM of the contralateral finger GONIOMETR Y • Center – placed on axis • Stationary arm – placed on stationary limb • Moving arm – placed over moving limb (i.e. line of travel) • Black numbers for ROM of all extremities; red numbers for foot, only. • Note. When reading degrees, read to the left, not right. Always start at 0 degrees! GONIOMETRY EXAMPLES • Left: Shoulder flexion and extension • Practice: Find shoulder flexion 0-115 degrees • Right: Elbow flexion and extension • Practice: Find 40-110 degrees elbow AROM WEEK 2: GONIOMETRY OF THE LE GONIOMETR Y EXAMPLES • Top: Knee flexion and extension • Practice: Find knee flexion 110 degrees • Bottom: Hip flexion and extension WEEK 3: MANUAL MUSCLE TESTING (MMT) OF THE UE MMT OF THE UE • Manual muscle testing is used to assess function and strength of various muscle, most commonly the UE. • Two techniques: •Break Technique: apply pressure until pt breaks position •Make Technique: resistance through the whole motion/range • No standard scale, as depicted on the right. • 0 – 5 is an ordinal scale, which means there are disproportional distances between grades. • Example: Grade 4 is not twice as strong as grade 2. Note. 3 is full ROM, >4 is subjective • Note. Use a cupping motion when performing MMT. • 0 = flaccid, nothing would happen MMT OF ELBOW • 1 = flicker or trace movements • Might get a little flicker, look at biceps – can slap to give stimuli • 2- = partial ROM, no gravity (so you are holding their arm) • Horizontal plane • Can only go halfway while being supported • 2 = full ROM, no gravity • Can get full ROM, but gravity is still eliminated • 2+ = against gravity position, goes through less than 50% of ROM • Arm is hanging, can only flex 20 degrees • 3- = more than 50%, but not full ROM • About 120 degrees • 3 = full ROM; holds test position • 3+ = slight pressure, two fingers, don’t let me break you, resist • 4- = slight to moderate pressure, about the palm of hand with slight resistance, anything heavier will break • 4 = moderate pressure, resisting with some force • 4+ = moderate to severe, push more • 5 = pushing really hard SOURCES OF ERROR RELIABILITY Compensatory movements Pain Contractures Tone Deformities Contraindications Lack of understanding Lack of effort Therapist training Different techniques Different amount of resistance Point and line of force applied Speed of resistance Duration of contraction Fatigue Motivation of therapist MMT QUICK SCREEN AROM PROM MMT of shoulder (up/down), biceps (pulling/pushing), squeeze fingers UE MUSCLES EXAMPLES • Abductor Pollicis Brevis (APB) • Function: abduction thumb CMC joint • To test: supinate hand, put your index finger on the volar side of their proximal phalanx, try to have them oppose their thumb while you resist, muscle will try to fire and pop UE MUSCLES EXAMPLES • Flexor Pollicis Longus (FPL) - very strong flexor • • • Function: flexion of the thumb at the interphalangeal joint • To test: block below IP joint of thumb, have them flex the tip • If thumb is in hyperextension, tendon is gone; natural position is slightly flexed Flexor Digitorum Superficialis (FDS) • Function: flexion of the middle phalanges of the four fingers (excluding the thumb) at the proximal IP joints • Isolate or flex at the PIP joint Flexor Digitorum Profundus (FDP) • Function: flexion of the fingers at the MCP and IP joints • Isolate or flex at the DIP joint UE MUSCLES CONT. • Extensor Pollicis Longus (EPL) • Function: extension of the thumb at the MCP and IP joints • To test: Put hand flat on table in pronation, have them lift their thumb off table, EPL will pop UE MUSCLES CONT. • Interossei • Palmar/Volar – ADDUCT • Put your fingers in between theirs and have them squeeze • Dorsal – ABDUCT • Wrap your hand around theirs, have them abduct UE MUSCLES CONT. • Lumbricals • Flex MCP and IP joints – wave goodbye • To test: put your hand on volar side of hand while they are in tabletop, have them try to pull their fingers down HAND ANATOMY: LUMBRICAL MUSCLES DORSAL INTEROSSEL MUSCLES (DAB) FUNCTION: ABDUCT FINGERS PULL FINGERS AWAY FROM MIDLINE (NOT PINKY) NERVE: ULNAR HAND ANATOMY: LUMBRICAL MUSCLES ADDUCTOR POLLICIS MUSCLE FUNCTION: THUMB ADDUCTION HAND ANATOMY: LUMBRICAL MUSCLES PALMAR INTEROSSEI MUSCLES (PAD) FUNCTION: ADDUCT FINGERS NERVE: ULNAR UE MUSCLES CONT. • Extensor Digitorum Communis (EDC) • Function: extends medial four digits at the metacarpophalangeal joints and secondarily at the interphalangeal joints. It also acts to extend the wrist joint • Have them make a claw with their hand, put your hand on their fingertips, apply pressure and have them try to extend, EDC will pop on dorsal side • Flexor Carpi Ulnaris (FCU) • Function: Allows you to ulnarly deviate • Test: elbow at 90, supinate hand, go into flexion and ulnar deviation (up and away) UE MUSCLES CONT. • Biceps Brachii • Function: flexion and supination (outward rotation) of the forearm • Test: supinated, push their forearm down while they flex • Brachialis • Function: flexes the forearm at the elbow • Test: pronated, resist flexion • Brachioradialis • Function: flexes the forearm at the elbow • Test: neutral, thumb up, resist flexion UE MMT: TESTING UE MUSCLES CONT. • Supinator • Biceps are the main muscle responsible for this • To test: elbow at 90, hold their hand like you're giving them a shake, support their elbow, have them try to supinate as you resist • Triceps • Stand up, lean on table, and kick back arm | or seated, bring arm back, support humerus, have them going into extension and resist • Difficult for older adults, or individuals with rotator cuff injuries UE MUSCLES CONT. • Empty Can Test • Tests the supraspinatus (important muscle of rotator cuff) • Arms up like superman • Position: elbow extended, shoulder in horizontal abduction, turn hand down like holding a can one hand on shoulder, push down at wrist, if you ask them to hold and arm slowly goes down = injury • Lift Off Test • Hand on back, palm facing out, try to lift hand off back, can gently resist • Tests for subscapular – STRONGEST muscle of rotator cuff (responsible for internal rotation) • Arm hides like a submarine HAND ANATOMY: JOINTS Click to add text HAND ANATOMY: INTRINSIC MUSCLES Function: fine motor, grasp Click to add text HAND ANATOMY: THENAR MUSCLES ABDUCTOR POLLICIS BREVIS (APB) FLEXOR POLLICIS BREVIS (FPB) OPPONENS POLLICIS (OP) FUNCTION: APB - ABDUCT FPB - FLEX OP - OPPOSE HAND ANATOMY: HYPOTHENAR MUSCLES ABDUCTOR DIGITI MINIMI (AND) FLEXOR DIGITI MINIMI BREVIS (FDM) OPPONENS DIGITI MINIMI (ODM) FUNCTION: ADM – ABDUCT LITTLE FINGER FDMB – FLEX LITTLE FINGER AT MCJ ODM – FLEX AND LAT ROTATE LITTLE FINGER AT CMC JOINT HAND ANATOMY: INTRINSIC MUSCLES Function: fine motor, grasp Click to add text HAND ANATOMY: EXTRINSIC MUSCLES Function: gross motor of hand and wrist HAND ANATOMY: EXTRINSIC MUSCLES Function: gross motor of hand and wrist HAND ANATOMY: EXTRINSIC MUSCLES Function: gross motor of hand and wrist HAND ANATOMY: EXTRINSIC MUSCLES Function: gross motor of hand and wrist WEEK 4: MMT OF THE LE & PINCH/GRIP TESTING MMT OF LE • Evaluation: • Testing: • PVD • Dorsiflexion MMT • History of diabetes • Plantar Flexion MMT • Weight bearing status • Hamstring MMT • Fall risks • Quadriceps MMT • Consult with PT • Thomas Test – Measure the flexibility of the hip flexors • Mobility equipment • Energy level • Any wounds or deformities DORSI/PLANTAR FLEXION MMT • Dorsi flexion • Have patient lay supine, stand at the end of the bed or next to it, put one hand on their tibia, other hand on the top of their foot, ask them to point their toes to their face and resist • Plantar flexion • In the same position, move your hand to the bottom of their foot and ask them to point their toes to the floor and resist DORSI/PLANTAR FLEXION ANATOMY HAMSTRING/QUADRICEPS MMT • Hamstrings • Function: Flex knee, ext hip • While patient is laying supine, have them lift their knee, place your left arm underneath their knee and your right hand on posterior side of tibia, tell patient to try to bring their foot to their butt while you resist • Quadriceps • Function: Ext knee, flex hip • In the same position, move your hand to the anterior side of tibia, tell patient to kick the soccer ball while you resist PINCH TESTING • Pinch strength is tested utilizing a pinch gauge, as depicted on the left. • Types of pinch: A.Tip pinch B. 3-jaw chuck C. Lateral/key pinch GRIP TESTING • Grip testing is completed using a dynamometer, as depicted on the right. • Positioning: • The client is seated with shoulder adducted, elbow flexed to 90 degrees with the forearm and wrist in neutral. • When ready the subject squeezes the dynamometer with maximum isometric effort, which is maintained for about 5 seconds. No other body movement is allowed. • The mean value of three trials is recorded, and both hands are compared. • Jamar testing measures hand-eye coordination as well as manual dexterity of the arm and hand for manipulative work. • Research has shown a link between Jamar testing, depression, and malingering • Position: 2 WEEK 5: HAND THERAPY ASSESSMENTS SEMMES– WEINSTEIN • Evaluation MONOFILAMENTS • Environment • Quiet room, normal temperature, good light • Materials • Monofilaments and hand map/colored pencils • Client History • Thorough history can help guide where to focus the test • Reference Area • Find an unaffected area and establish what is “normal” for the patient • Application GIANT BOOBS PULL REDRECKS • Begin with normal threshold filaments and progress filaments until the patient can identify the touch (1/3 trials is considered an affirmative response) • Filaments are applied 1.0-1.5 seconds at a time, lifted off the skin 1.0-1.5 seconds TWO-POINT DISCRIMINATION • Ability to perceive the difference of 1 or 2 stimuli • A light application of the tool using one or two points. • Must be longitudinal, not horizontal or crooked. • The hand or UE is comfortable and vision is occluded • Testing is performed in a randomized sequence and points are in a longitudinal fashion, perpendicular to the skin • 7/10 responses are considered accurate! • Scoring (Note. Document fingers, size, and number of trials) • Normal is 0.5 cm or less • Fair is 0.6 cm to 1.0 cm • Poor is 1.1-1.5 cm • Always start at 0.5 cm; Testing is discontinued at 1.5 cm • Note. Quickest assessment STEREGNOSIS • Stereognosis - the ability to perceive and recognize the form of an object in the absence of visual and auditory information, by using tactile information to provide cues from texture, size, spatial properties, and temperature, etc. • Steps • Choose about 5 common household items • Explain and demonstrate the test • With vision occluded, place object in the client’s hand (you should test both hands for reference) • Record how many objects they are able to identify and record Note. Typically used for CVA patients NERVE INNERVATION NERVE IMPINGEMENT TESTS Pronator Syndrome Carpal Tunnel • Median nerve impinged just below the elbow • Test: Shake hands with patient, tell them to pronate, add resistance: • pain = positive sign • Median nerve impinged at wrist level • You need medium strength to lay down the carpet • Test: Tinel’s test – tap directly down the center of the forearm elbow to wrist on the palmer side: pain = positive sign, Phalen’s test – prayer position: pain = positive sign, Durkan’s test – apply compression by use of fingers over the wrist for 30 seconds, numbness of fingers = positive sign Cubital Tunnel • Ulnar nerve entrapment at the elbow • Test: Elbow flexion held for 30 seconds, numbness of pinky and ring finger = positive sign Radial Tunnel Syndrome • Radial nerve impinged directly below the lateral epicondyle of the elbow • Test: apply resistance to ring finger extension, pain = positive sign Cervical / Double Crush Syndrome • Bilateral hand numbness = positive sign CARPAL TUNNEL Median Nerve TESTING RADIAL NERVE DAMAGE • Cannot make a thumbs up • Wrist Drop • Unable to extend wrist • Radial Tunnel Syndrome • Can be misdiagnosed as tennis elbow/lateral epicondylitis • A few cm distal from the lateral epicondyle, palpate over epicondyle and if it doesn't hurt, move down to radial tunnel, pain = + • To test: shake their hand and have them try to supinate as you resist, pain = + • Middle finger test – put finger on back side of distal phalanx, have them try to extend as you resist, pain = + MEDIAN NERVE DAMAGE • Cannot make an "OK" sign (tip to tip) • Hyperthenar Atrophy • Take your two hands, look straight down, make sure the thenar eminence looks meaty/concave, not convex/flat • Ape Hand • Thumb is flat against index finger, cannot abduct thumb • Benediction/Preacher's sign (can be median or ulnar) • RF and SF flexed, thumb, IF and MF extended, can't make a fist • AIN Syndrome • Anterior Interosseus Nerve; presents like an "L" shape, FPL of thumb and FDP of index do not work MEDIAN NERVE DAMAGE • Hyperthenar Atrophy • Take your two hands, look straight down, make sure the thenar eminence looks meaty/concave, not convex/flat MEDIAN NERVE DAMAGE (CONT.) • Pronator Syndrome • Located right below the elbow, due to repetitive movements • To test: Tell patient to shake your hand, have them try to pronate while you resist, pain = + • Carpal Tunnel • Between the hypo and thenar eminence • Phalen's sign – prayer stretch • Reverse Phalen's – dorsal side of hands • Tinel's sign – tap over median nerve; start proximal to distal • Durkan's Test – push down and hold on carpal tunnel, fingers go numb = + ULNAR NERVE DAMAGE • Cannot cross their fingers • Froment's Sign • Take a piece of paper, tell client to pretend they are texting, slide paper under their thumbs, have them try to hold the paper as you pull it away, if their thumb IPs hyperflex = positive • Adductor pollicis brevis is not working, thumb will cheat and FPL will kick in to help • Wartenberg Sign • SF sticks out to side and floats in space, cannot adduct their finger • Intrinsic muscles are not working, missing adduction – ulnar nerve fires the intrinsics • Benediction/Preacher's Sign (can be ulnar or medial) • RF and SF flexed, thumb, IF and MF extended, can't make a fist POSITIVE: FROMENT' S SIGN Texting FROM your phone to get an umbrella POSITIVE: WARTENBER G'S SIGN Drinking tea under an umbrella with Dr. Penny in Wartenberg tea = pinky out Umbrella = ulnar nerve Wartenberg = name ULNAR NERVE DAMAGE (CONT.) • Claw Hand • SF and RF MCP joints are hyperextended, IP joints are flexed (can affect all digits) • 1st Dorsal Interosseous Atrophy • Thumb webspace – atrophy, no fleshy area; may see wasting in between the metacarpals • Guyon's Canal • Located off the pisiform, bottom of wrist and ulnar side; SF and RF will go numb • Tinel's Sign • Activity that aggravates it: cycling, weightlifters • Cubital Tunnel • Wraps around posterior side of elbow, very superficial, "garden hose" • When you flex your elbow for 30 seconds and SF & RF go numb, but goes away after you straighten = positive GUYON'S CANAL 1ST DORSAL INTEROSSEOUS ATROPHY ULNAR NERVE MEDIAN NERVE RADIAL NERVE THORACIC OUTLET SYNDROME • If they have symptoms in hand, look proximal • Symptoms coming from neck? Cervical problem? • 90% of the time it comes from the neck • If symptoms are bilateral = RED FLAG! NERVE LOCATION S LEFT HAND WEEK 6: TRANSFERS AND STAIRS CASE SCENARIO 36-year-old female in MVA 2 weeks ago. Sustained right tibial plateau fracture. On best rest for 2 weeks because of sepsis and DVT in right leg. ORIF performed on day of admission. OT/PT evaluate and treat and up to chair. • What to do first: HPI, past medical history, premorbid functions • Testing: • Physical: AROM, PROM, MMT • Neuro: Sensory testing • Cognitive: Observe WEEK 9: KINESIOTAPE SKIN AND ITS SENSORY RECEPTORS THE ENDOGENOUS ANALGESIC SYSTEM • Pain is modulated by Kinesio Tex Tape’s effect on the skin and superficial fascia • Compressive forces may stimulate mechanoreceptors • Decompressive forces may decrease inflammation and unload mechanoreceptors • Either force can relieve pain APPLICATION • I Strip: Tension focused within the therapeutic zone directly over target issue • Y Strip: Tension is dispersed through and between two tails over target issue • X Cut: Tension is focused directly over target issue and dispersed through tails at each end • Fan Cut: Tension is dispersed over target issue through multiple tails KINESIO TAPING® TENSION PERCENTAG E GUIDELINES • Super Light 0-10% • Paper off 10-15% (stretch already in tape) • Light 15-25% (see fibers) • Moderate 25-35% • Severe 50-75% (looking through and see pattern) • Full 75-100% • 0% tension anchor or end BASIC KINESIO TAPING MUSCLE APPLICATIO N CONCEPTS D to P (I to O) • Distal Proximal • To inhibit overused muscle – acute conditions, muscle spasm • 15% to 25% tension • DIP P to D (O to I) • Proximal Distal • To facilitate weak muscle-chronic conditions, rehabilitation • 15% to 35% tension • PDF Therapeutic Direction is the recoil of the tape toward the anchor Therapeutic Zone is the region of tape applied to targeted tissue WEEK 10: NEURO TESTING UE TESTING Finger-to-thumb Test Each tip to thumb Looking for: Fluidity of movement, overflow (other hand mirrors when patient does one hand, heavy concentration Test: bilaterally, one hand at a time, eyes open, then eyes closed Finger to nose Looking for: fluidity of movement (smooth and coordinated), hitting target (dysmetria: no sense of distance; overshoot, or miss target), weakness, tremors Rapid alternating movements Dysdiadochokinesia: cannot copy movement Looking for: smoothness of movement Difficult for individuals with brain lesions Pronator Drift Test Lesion on opposite side of drift Test: eyes close, arms out elbows straight with palms up UE TESTING Rebound phenomenon Test: Pretend you are arm wrestling, resist, then let go Positive sign: overshoot, hit him/herself Negative sign: can prevent themselves from hitting themselves Archimedes spiral Draw spiral circle going outward, then pt has copy it Testing tone Tone: amount of resistance to passive range of motion; velocity dependent, needs to be fast, fluctuate speed o Hypertonia: more resistance cogwheeling (a jerky feeling in your arm or leg that you can sense when moving or rotating your affected limb or joint) o Hypotonia: floppy, Jell-O; range is greater than expected Proprioception Test: seated with arm on table, pt closes eyes, “tell me if my pushing your thumb up or down”, about 3 times, mix it up Looking for: speed of response, hesitation/confidence of response TREMOR TESTING Intention tremors • Definition: involuntary, rhythmic muscle contractions (oscillations) that occur during a purposeful, voluntary movement; tremor when you are intending to do something • Common for MS Resting tremors • Definition: occurs when the muscle is relaxed, such as when the hands are resting on the lap • With this disorder, a person's hands, arms, or legs may shake even when they are at rest • Common for Parkinson’s • Pill rolling Essential tremors • Definition: a nervous system (neurological) disorder that causes involuntary and rhythmic shaking • affect almost any part of your body, but occurs most often in your hands • especially when you do simple tasks, such as drinking from a glass or tying shoelaces ***tremors: different rhythmic frequencies OTHER MOTOR SYMPTOMS Dysmetria: a condition in which there is improper measuring of distance in muscular acts (overshooting) o hypermetria: overreaching (overstepping) o hypometria: underreaching (understepping) Bradykinesia: lowness of movement o It is one of the cardinal symptoms of Parkinson's Ataxia: uncoordinated movement o look/move drunk Clock drawing test • Test: tell pt draw the face of a clock (cue based on needs: “draw circle then fill in the numbers”; “start with the 12 at the top” • Next (grade up), tell them to put the hands in a certain time • tests for: left/right side neglect; stroke patients • left side neglect is more common Apraxia: Difficulty with skilled movements even when a person has the ability and desire to do them • IdeationalNo idea or concept of a task; can’t start a task, or think of the steps • Ideomotor • Understands the concept, but motor-wise is wrong • Can perform spontaneously, but can’t on command OTHER MOTOR SYMPTOMS Dressing • Dressing task/sequencing of dressing doesn’t make sense • Test: dressing assessment, initial eval Constructional • inability of patients to copy accurately drawings or three-dimensional constructions • Test: jenga, pyramid LE TESTING Heel-to-shin Test • Slide heel straight down opposite shin • Looking for: smooth, coordinated movement; pure coordination Toe taping • Looking for: Coordination • Tape foot in rhythmic fashion Arm swing • Looking for: rhythmic swinging of arms Romberg test • Proprioceptive test • Test: standing, ability to catch them/they can be supported; eyes open, have hands on their side, then, pt closes eyes (observe)Positive: lean or fall to one side; relying on eyes to keep balance TYPES OF GAIT Hemiplegic gait: one side; hike hip and swing leg due to weakness (could have foot drop) o UE could be clenched to body o Overcompensating techniques Diplegic gait (spastic gait): bilateral side o o o o Walk on tippy toes Adductors are very tight, feet rotated inward UE constructed to body Cerebral palsy Neuropathic gait (steppage gait) o High stepping to clear foot due to foot drop o Common in foot drop Ataxic gait (uncoordinated walking) o Wide stance to stay balanced to avoid following o Drunk walk home from troopers Sensory gait (stomping gait) o Common with: sensory seeking, diabetic due to lose of sensation/neuropathy Parkinsonian gait o o o o Narrow BOS, shuffling gait; no steppage or arm swing Universal flexion (UE, trunk, etc) Heavy leaning forward to start walking Very stiff and rigid movement WEEK 11: MODALITIES Frequency ULTRASOUND • Superficial: 3 MHZ • Deep: 1 MHZ Intensity • Thermal: greater than 0.8 • Nonthermal: 0.8 or less Pulse versus continuous • Thermal: chronic, improve elasticity • Nonthermal: acute, healing • Turning stove on and off = water never boils Time • Lots of tissue = more time • Less tissue = less time ULTRASOUND DECISION MAKING GUIDELINE Non-thermal Inflammatory or Acute Phase 0.2 w/cm² 20% duty cycle Mild heating Proliferative or subacute phase 0.2 to 0.8 w/cm² 50% duty cycle Therapeutic heating Remodeling or chronic phase 0.8 to 2.0 w/cm² 100% duty cycle TENS 1. Types of TENS a. TENS used for Pain control i. Acute pain or chronic pain ii.High rate: frequency is really high (acute) 1. Sensory setting iii.Low rate: frequency is low (chronic) 1. Motor setting 2. Chronic = 3 months or more iv.Noxious is rarely used b. Order of recruitment i. Sensory -> motor -> noxious TENS Sensory is always first, then early motor, then motor (contraction) *Inverse relationship between the amplitude and the pulse duration (if one goes up the other goes down) Remember: • Black – smoke over fire = Motor Point (NMES Only) • Increased rate = increased muscle fatigue • Ramp time: Normal = 2.0 seconds • We are now trying to fire ‘motor’ units vs sensory. - Thus compared to TENs, rate, pulse and intensity may be slightly higher • Red electrode = positive (anode) • Black electrode = negative (cathode) • Frequency = require approximately 35 to 50 pps to produce smooth tetanic contraction • Pulse Duration = 150 to 350 microseconds to stimulate motor nerves • Farther apart the deeper it does (pads) • Chronic pain = low rate (thumping sensation) NMES a. Muscle strengthening/muscle re-education b. Know terms: i. Pulse rate ii. Pulse width/duration iii.On/Off time (rest breaks) 1. Goal oriented a. Ex. Going to the gym: no rest between sets = exhausted, cannot continue b. Start with long rest and slowly decrease break time iv.Ramp up ramp down 1. Kicking door open = scared response (rapid, painful reaction) vs. slowly opening the door = comfortable response (gentle, functional reactions) v. Modulation: solution to the problem vi.Accommodation: feeling, what is happening to the physical vii.Asymmetrical biphasic = small muscles viii.Symmetrical biphasic = large muscles WEEK 13: COGNITIVE SCREENING MINI MENTAL The Mini-Mental State Exam (MMSE) is a widely used test of cognitive function among the elderly; it includes tests of orientation, attention, memory, language and visual-spatial skills. GLASGOW COMA SCALE Categorization Coma: No eye opening, no ability to follow commands, no word verbalizations (3-8) Head Injury Classification Severe Head Injury----GCS score of 8 or less Moderate Head Injury----GCS score of 9 to 12 Mild Head Injury----GCS score of 13 to 15 EXECUTIVE FUNCTION Attention Memory Calculation Abstract thought Visual and body perception (agnosia) Mini Mental State Test Orientation Concentration Problem-solving Reaction time Sequencing Spatial (copy a design, clock face) Judgement and insight LOBE FUNCTIONS Lobe Alteration in Higher Function Frontal Apathy, disinhibition Temporal Memory Parietal Calculation, perceptual & spatial orientation (nondominant hemisphere) Occipital Perceptual & spatial orientation LOBE FUNCTIONS WEEK 15: VITALS VITALS!!! PR Less than 60 BPM = bradycardia More than 100 BPM = tachycardia RR = 15 – 20 breaths per minute BP = 120/80 O2 = 95-100% Temperature <94 hypoxia (blue) <90 medical emergency BLOOD PRESSURE Measure of pressure exerted by blood as it flows through the arteries Blood pressure is recorded in millimeters of mercury and is recorded as a fraction Pulse Pressure Systolic pressure is written over the diastolic pressure • Example: 136/72 The difference between the systolic and diastolic blood pressures • Example: 110/70 • Pulse pressure is 40 DETERMINANTS OF BLOOD PRESSURE Cardiac Output Peripheral Vascular Resistance • Weak heart = volume with each contraction = C. O. = BP • Strong heart = volume with each contraction = C. O. = BP • Vasoconstriction (smaller lumen) = increased resistance = BP • Vasodilatation (larger lumen) = decreased resistance = BP Blood Volume Blood Viscosity (thickness) • Decreased volume = Decreased blood pressure • Increased volume = Increased blood pressure • Increased RBC (more RBC/less plasma) • Measured by hematocrit (> 6065% = elevated BP) FACTORS AFFECTING BLOOD PRESSURE • Age • Older person: Elasticity/ flexibility of the arteries decreases, and BP rises • Stress and Emotions • Race • Sex • Exercise • Diurnal Variations • Medications • Environment • Disease Process • Lifestyle • Smoking • Alcohol • Cholesterol FACTORS AFFECTING BODY TEMPERATUR E Age Basal metabolic rate (BMR) Diurnal Variations Hormones/ Catecholamines Stress Exercise Environment TAKING A PULSE Use radial artery most of the time Don’t use neck pulses Count one full minute Should be strong and easy to feel Reported as “P= 85” Gender FACTORS AFFECTING PULSE RATE Exercise Fever Medications Hypovolemia (high blood volume) Stress, fear, & pain Position changes (supine, sit, stand) Pathology RESPIRATION Observe while patient is at rest Don’t let them observe you counting (they can unconsciously change their rate) Up, down = one cycle Count for one full minute Reported as “RR=16” Anxiety/stress/pain FACTORS AFFECTING Activity RESPIRATION Increased environmental temperature Decreased environmental temperature Increased altitude Medications Increased intracranial pressure Age During anaesthesia the oxygen saturation should always be 95 - 100%. If the oxygen saturation is 94% or lower, the patient is hypoxic and needs to be treated quickly. A saturation of less than 90% is a clinical emergency (WHO, 2011, pg. 8) Normal 95%-100% ORTHOSTATIC/ POSTURAL HYPOTENSION • BP that falls 20 mm Hg or more when a patient sits or stands • Orthostatic hypotension • Blood leaves the central organs (esp. the brain) and moves to periphery causing the person to feel faint • BP 3x: assess by taking BP while lying, sitting, then standing NORMAL VITAL SIGNS CHANGE WITH AGE, SEX, WEIGHT, EXERCISE TOLERANCE, AND CONDITION Temperature 97.8 - 99.1 °F/ average 98.6°F 36.1–37.8 °C / average 37°C Pulse 60 - 100 beats per minute Respiration 12 - 18 breaths per minute Blood Pressure 90/60 mm/Hg to 120/80 mm/Hg