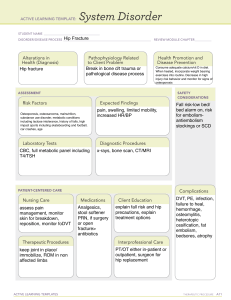
Orthopedic Examination Guide: Spine, Shoulder, Elbow, Hip
advertisement

ORTHO SPINE EXAMINATION 1. 2. 3. 4. LOOK 1. 2. wash your hands, explain the procedure and gain informed consent adequate exposure Aids & adaptions- walking stick/wheelchair Gait- smoothness, speed, symmetry, turning, antalgic, Trendelenburg 3. From behind a. Scars b. Wasting/prominent of muscle- paraspinal, trapezius, gluteal, hamstrings, calf muscles c. Symmetry of each side (any scoliosis- lateral curvature of spine [S shape]) d. Abnormal hair growth- spinal bifida (hair tuft) e. Pelvic tilt 4. From side a. Cervical lordosis- hyperlordosis (spondylolisthesis, osteoporosis, discitis) b. Thoracic kyphosis- hyperkyphosis *>45°+ (vertebral #, scheuermann’s kyphosis) c. Lumbar lordosis- hyperlordosis (obesity, tight lower back muscles) d. Gibbus- acute angulation of spine in Pott’s disease 5. From front a. Posture of head and neck- torticollis b. Symmetrical of shoulder FEEL 1. 2. 3. 4. Temperature, Tenderness, Muscle spasm, Swelling, Spinal level Along entire length of spine Each spinous process- most prominent spinal process T1 Sacroiliac joints Paraspinal muscles *because difficult to observe patient’s face, ask regularly for discomfort and pain MOVE (performed actively- what restrict the movement? pain/stiffness/muscle spasm) A. For cervical movement 1. Lateral flexion: ask patient to place ear on shoulder 2. Rotation: ask patient to look over shoulder 3. Flexion: ask patient to put chin on chest 4. Extension: ask patient to put head back to look at ceiling B. For thoracic movement 1. Right and Left rotation: ask patient to turn to each side For these movement need to fix the pelvis by a. Patient sitting at the edge of back with arm crossed across chest or b. Examiner hold pelvis down C. For lumbar movement 1. Flexion and Extension: ask patient to touch toes with legs straight & lean backwards as far as possible 2. Lateral flexion (left & Right): ask patient to run hand down to the outside of leg, keeping legs straight SPECIAL TEST 1. Straight leg raising test (± sciatic stretch test): to assess nerve entrapment such as sciatica, PID - One hand hold below the ankle and the other above the knee – to make sure knee is extend Look at patient’s face, slowly raise the straight leg Noted at which degree it is painful. Improving compression (relieve) is when the degree is getting bigger If no pain, raise up to 90°, thus no more compression. 2. Lasegue’s test SLR, marked the painful degree Slowly lower the leg, until reach degree where there is no more pain Dorsiflexes the ankle: POSITIVE if there is pain. 3. Bowstring test SLR, marked the painful degree Change the hand that hold above the knee, to be below the knee where fingers are on the lateral hamstring muscle Slightly flex the knee, until no pain Press on the hamstring muscle, PAIN again = POSITIVE = reproduction of radicular pain with popliteal compression 4. Schober’s test: to test range of motion in lumbar spine, may reduced in ankylosing spondylitis 5. Femoral nerve stretch test NEUROLOGICAL EXAMINATION (Upper limb- cervical, Lower limb- lumbar) VASCULAR EXAMINATION SHOULDER EXAMINATION 1. 2. 3. LOOK: i. ii. iii. iv. v. As always wash your hands, explain the procedure and gain informed consent. As with the other examinations, you should start by exposing the joint. Start by observing the shoulder joint looking from the back, side and front shoulder contour/ same level / symmetrical skin colour changes bruising, injuries, scars muscle wasting : deltoid & trapezius deformity : square of shoulder, popeye sign, winging scapula With the patient still stood, you should perform two quick and easy function tests. This involves the patient placing their hands behind their head and behind their back. This checks that they can perform everyday tasks FEEL: TEMPERATURE & TENDERNESS Next feel over the joint and its surrounding areas for the temperature of the joint as raised temperature may suggest inflammation or infection in the joint. Systematically feel along both sides of the bony shoulder girdle. Start at the sternum sternoclavicular joint work along the clavicle acromioclavicular joint feel the acromion and scapulo-thoracic joint around the spine of the scapula greater tuberosity anterior & posterior joint lines of gleno-humeral joint and finally the muscles around the joint for any tenderness. = “no bony irregularities” Feel for 2D 1P: 2D: Vascular & Neurological status o Radial pulse is palpable & capillary refill time <2s o Motor & Sensory (using cotton) for all (upperlimbs) MOTOR SENSORY C5 Shoulder abduction Deltoid st C6 Elbow flexion Dorsal 1 web space C7 Elbow + wrist extension Tip of middle finger C8 Wrist + finger flexion Tip of little finger (grip strength) T1 Finger abduction Medial aspect of forearm /adduction - o + Reflexes : Biceps (C5,C6), Triceps (C7,C8), Supinator reflex (brachioradialis reflex:C6,C7) 1P : Lymph nodes not enlarged Flexion Extension MOVE: ACTIVE & PASSIVE (we push + feel for crepitus while moving the joints) i. Flexion (0-180°) – bring their arm forward ii. Extension (45-60°) – bend their arm at the elbow and push backwards iii. Abduction (0-150°) – bring their arm out to the side and up above their head iv. Adduction (0-45°) v. external rotation (0-90°) – flex the elbow & tuck it into the side & move the hand outwards vi. internal rotation (70-90°) – how far they can place their hand up their back Ext rotation Abduction Int rotation SPECIAL TEST: There are special tests which can be performed on the shoulder: I. Impingement test : is performed by placing the shoulder out at 90 degrees with the arm hanging down, press back on the arm and check for any pain. o Neer’s test: stabalise pt’s scapula by placing your hand on the scapula arm fully pronated, shoulder flexion, like saying “HAI” style Hitler. Impingement on the sub acromion, painful. ACTIVE test o Hawkin’s test: flex shoulder 90, flex the elbow 90, and internally rotate = like a defense hands position painful. ACTIVE test o Apley’s test: stand behind the patient slightly to side at the shoulder. One hand holds above the shoulder, the other hold below the elbow. Flex : NO pain (because the greater tuberosity go backward. Extent: PAINFUL (greater tuberosity go anteriorly together with the tender) II. Apprehension test is similar but the arm is facing upwards and push back on the arm; the patient may be apprehensive about the movement as the joint feels unstable. III. Scarf test is performed with the elbow flexed to 90 degrees, placing the patient's hand on their opposite shoulder and pushing back, again look for any discomfort IV. Supraspinatus (Rotator Cuff Muscle testing): o Empty can/Jobe’s test o Drop arm test 8. An extension to this station may be to assess each rotator muscle individually. 9. Thank the patient and wash your hands. OTHER SPECIAL TEST FOR UPPER LIMBS: ELBOW: 1. There is an osteocele triangle below the elbow 2. IN EXTENSION (Elbow) it is in the same line 3. When flex the elbow it become triangle 4. Compare both sides are they equal or not WRIST : FINKELSTEIN’S TEST for De Quervains tenosynovitis 1. Flexion & Adduct thumb, 2. Keep inside other fingers (thumb in the palm) 3. We stretch more (ulna deviate downward) painful Wrist : 1. 2. 3. level of bony prominence: ulna styloid / radial styloid, not in the same level (NORMAL). Radial more distal (longer). So if fracture, it may go up radius shortening ELBOW EXAMINATION LOOK/INSPECTION From front: 1. Carrying angle (Normal: 10°-15° of valgus) 2. Varus / Gun stock deformity From side: 1. Flexion deformity At the elbow: 1. Scars & rashes 2. Muscle wasting 3. Rheumatoid nodules 4. Swellings 5. Psoriatic plaques PALPATION 1. Temperature across the joint & forearm – using back of hand 2. Swelling & tenderness – palpate the joint lines a. Olecranon process – if tender = bursitis b. Medial epicondyle – Golfer elbow c. Lateral epicondyle – Tennis elbow d. Radial head – below & lateral to epicondyle 3. Bony irregularities 4. 2P Neurovascular of upper limbs – pulses & motor sensory 5. 1D lymph nodes MOVEMENTS (active passive) 1. Extension & Flexion (0-145) 2. Pronation (70) & Supination (85) – feel for crepitus when passive move & must be at the side (don’t abduct the shoulder) SPECIAL TEST: 1. Tennis elbow – Lateral epicondylitis a. Any tenderness at lateral epicondyle b. Hold in pronated position & make a fist c. Extend the wrist against resistance 2. Golfer’s elbow – Medial epicondylitis a. Any tenderness at medial epicondyle. b. Hold out arms in pronated position & make a fist c. Flex the wrist against resistance HIP EXAMINATION 1. Wash your hands, explain the examination and gain informed consent. 2. Ask the patient to walk for you. LOOK: a. Gait: o Antalgic – limp o Trendelenberg – waddling due to proximal muscle wasting o High stepping gait – foot drops b. Walking aids used? : o Axillary crutches o Elbow crutches o Walking stick o Zimmer frame c. From front: o Deformities : limb rotation, fixed flexion, Valgus / Varus o Symmetrical / asymmetrical o Wasting : quadriceps d. From side: lumbar lordosis ( suggestive of Lumbar lordosis) e. From behind: o Scoliosis o Wasting : gluteal muscles o scars f. Trendelenberg sign test (while standing): This is done by asking the patient to alternately stand on one leg. Stand behind the patient and feel the pelvis. It should remain level or rise slightly. If the pelvis drops markedly on the side of the raised leg, then it suggests abductor muscle weakness on the leg the patient is standing on Next, you should ask the patient to lie on the bed. FEEL Tenderness & temperature changes a. Greater trochanter : ASIS go behind (posterior) then below (inferior) the 1st most prominent (tender: trochanteric bursitis) b. Lesser trochanter (tender: Iliopsoas strain) c. Ischial tuberosity (tender: hamstring strain) d. Sarcoiliac joints e. 2 Distals: a. Vascular : Dorsalis pedis, Posterior tibialis b. Motor Sensory : Dorsiflex f. 1 Proximal : Inguinal lymph nodes MOVE : ACTIVE & PASSIVE Flexion(120°) = flex the knee to 90 degrees and passively flex the hip by pushing the knee towards the chest. ABDuction (45°)= stabilize the pelvis by your hand on the contralateral ilium. Hold ankle to make sure hip not rotated. ADDuction (30°)= stabilize the ipsilateral hip first, then just like abduction. Internal rotation (40°)= Flex hip & knee 90° rotate foot LATERALLY role the shin LATERALLY External rotation (45°) = Flex hip & knee 90° rotate foot MEDIALLY role the shin MEDIALLY Extension (20°)= in prone (meniarap), actively extend the hip MEASUREMENT Position the patient: - Supine - Squared pelvis : mark both ASIS with a marker/eye liner, take a tape and connect both ASIS with the tape, and let the rest of the tape falls at the edge of the bed. If it is not perpendicular, thus adjust the pelvis until both ASIS line is perpendicular to the bed - Legs in the same posture / Identical position Compare measurement of both sides: 1. Apparent leg length = xyphisternum – Medial malleolus. if asymmetrical : flexion deformity or spinal abnormalities 2. True leg length = ASIS – Medial maleolus 3. Segmental length – it’s done if True length is shorten a. Femur : ASIS – medial knee joint line b. Tibia : Medial knee joint line – medial malleolus If both sides are equal segmentally Dx: Tibial # If both sides are NOT equal, thus do the Bryant Triangle 4. Bryant Triangle a. Vertical line from ASIS perpendicular to the bed downward b. Horizontal line from Greater trochanter upward Vertical line c. Meeting point between the vertical and horizontal lines are marked Horizontal line d. Measure the horizontal line from the meeting point to the Greater trochanter SHORTEN = SUPRA-trochanteric : INTER-trochanteric # / Neck of femur # NOT SHORTEN = IINFRA-trochanteric : SUB-trochanteric # / Shaft of femur # SPECIAL TEST: 1. Thomas’s test : for FIXED FLEXION HIP DEFORMITY - Lying flat, observe from the side, any exaggerated lumbar lordosis - Confirm it by putting my hand between 2B: back & bed - Flex both knee & hip and ask the patient to hold the knees. - Test again, by putting hand between the 2B:Back &bed, now I cannot put my hand between them. Meaning that the lumbar lordosis is obliterated - Patient keep on holding the normal limb, try extend the affected side - If NO FFD, patient can straightly extend the affected side - In case of FFD, try to extend, there is resistant, around 30° 8. Thank the patient and wash your hands again KNEE EXAMINATION 1. Intro, wash hands, explain about the examination, ask consent and adequate exposure 2. Ask him to walk lie on bed LOOK: 1. Gait : limping? 2. Deformities: a. Valgus (knock knees) b. Varus (bow legged) c. Genu Recurvatum = hyperextension of knee beyond normal 10° d. Fixed flexion deformities 3. Muscle wasting : Quadriceps bulk 4. Symmetrical / asymmetrical 5. Skin changes: cars, redness, rashes 6. Swellings : (main causes in knee) a. Bony swellings b. Synovial thickening c. Fluid collection – e.g: Baker’s cyst in OA (popliteal swelling – from behind) FEEL: TEMPERATURE & TENDERNESS border of the patella for any tenderness behind the knee for any swellings along all of the joint lines for tenderness o medial & lateral aspects of the joint, 2 soft triangular hollows o superior to the hollow at the point of insertion of the patellar tendon. MOVE : ACTIVE + PASSIVE (push + feel for crepitus) Compare both sides flexion (150°) = bring foot to bottom extension (10°) SPECIAL TEST: 1. BULGE test: SMALL EFFUSION (lying or sitting hanging by edge of the bed) a. Put hand 15 cm proximal to knee joint (at the anterior thigh) b. Slide hand /milking down towards knee = to empty the SUPRAPATELLA BURSA (if hanging at the bed, no need to do this) c. Press on medial side (3x) to empty the MEDIAL compartment. All fluid is in lateral compartment d. Release medial pressure, & press on the LATERAL side (1x) e. BULGE at the MEDIAL = effusion 2. PATELLA TAP : LARGE EFFUSION a. Empty the SUPRAPATELLA BURSA b. Maintain constant downwards pressure c. 2 fingers on patella, press firmly & briskly downward d. There is colliding sound (hit the underlying femur) and it will bounce back 3. McMurray’s test : assess the menisci a. One hand hold the knee, one hand hold sole of the foot (support) b. Fully flex knee c. Apply VALGUS stress to the knee (tolak knee ke dalam) d. The other hand EXTERNALLY rotates the leg (tibia) & EXTEND the knee e. Pain/audible click = torn MEDIAL meniscus (more common, atleast remember this one is enough, no need to remember the lateral, nanti confuse) f. *for LATERAL meniscus =fully flex, give varus stress, internal rotation, extend the knee 4. INSTABILITY TESTS: a. VALGUS & VARUS STRESS TEST : Medial/Lateral Collateral ligament i. Valgus stress test 1. Supine 2. Knee fully extend 3. Hold ankle & thigh 4. Apply valgus force at knee (tolak ke dalam) 5. Repeat at knee flex 20° 6. Abnormal opening up at the joint on the stressed side (joint line separate abnormally) / distal part go outward = weakness/tear of MEDIAL collateral ligament ii. Varus stress test 1. Supine 2. Knee fully extend 3. Hold ankle & thigh 4. Apply varus force at knee (tolak keluar) 5. Repeat at knee flex 20° 6. Abnormal opening up at the joint on the stressed side (joint line separate abnormally) / distal part go inward = weakness/tear of LATERAL collateral ligament b. ANTERIOR / POSTERIOR DRAWER’S TEST : Anterior / Posterior Cruciate ligament i. Flex both knee 90° ii. Check ankles are at the same level iii. Any sagging of tibia & correct the sagging iv. Stabilize the foot by sitting on it v. Ensure the hamstrings are relaxed vi. Place both thumbs either side of tibial tuberosity vii. Other fingers encircle the proximal tibia viii. PULL tibia forward relative to femur (ANTERIOR). PUSH tibia backward (POSTERIOR) ix. Normal : little movement x. Pathology: abnormal anterior/posterior translation c. LACHMAN’S TEST : ANTERIOR cruciate ligament i. Flex knee 30° (if the patient leg is too heavy, support with your own thigh below his knee) ii. Hold the thigh firmly (secure the femur) iii. Try move tibia forward (anteriorly) on the femur iv. Normal: little movement v. Pathology: move > 5mm THOMAS SPLINT Splintage indication/uses/benefits - Immobilization of hip & thigh injuries in order to minimize the pain - Transportation of patient with lower limb injuries - Example: fracture of shaft of femur after MVA/trauma to be transported to hospital Principles - Support for comfort and prevent sagging - Counter traction provided by ischeal tuberosity - It has a ring & two bars joined distally - The ring is at an angle of 120 degree to the inside bar - The ring size is found by addition of 2 inches to the thigh circumference at the highest point of the groin - The length is the measurement from the highest point on the medial side of the groin up to the heel plus 6 inches. Type of traction = Fixed traction based on technique/mechanism How to apply: 1. Size of the Thomas splint’s ring must be 2 inches more than the circumference 2. Length from Greater trochanter to the foot or measure true length (ASIS – medial malleolus), the Thomas splint must be 6-8 inches longer the leg length 3. Make a cradle using towel or bandage, so that the leg can be placed over there 4. Apply skin traction/skeletal traction 5. Under analgesic, carefully lift the leg, ask an assistant to help inserting slowly & carefully 6. Push up as much as possible, be careful of the scrotum (male patient) 7. Pull the traction/rope, tie/fix at the splint end notch so that it can fix PRINCIPLE MANAGEMENT FOR CLOSED FRACTURE 1. REDUCTION 2. HOLD 3. EXERCISE 1. REDUCTION Aim 1. Adequate apposition 2. Normal alignment of bone fragments (allow bone back to its correct position) *greater contact surface area, more likely healing to occur *articular fracture- need reduction as near to perfection because any irregularity will predispose to degenerative arthritis Reduction 1. When there is little or no displacement UNnecessary 2. When displacement doesn’t matter (eg: some # of clavicle) 3. When reduction is unlikely to succeed (eg: compression # of vertebrae) Challenging Swelling of soft tissues during first 12 hours (so always do CMR before muscle spasm) Method 1: CLOSED REDUCTION Method 2: OPEN REDUCTION Indications: Indications: 1. All minimally displaced fracture 1. Closed reduction failed 2. Most fracture in children -difficult to control the fragments 3. Fracture that likely to be stable after -soft tissues interposed the fragments reduction 2. Large articular fragment that need accurate positioning *Most effective if muscle & periosteum (soft 3. For avulsion fracture tissues) on one side of fracture remain intact; -fragments are held apart by muscle pull -will prevent over-reduction & stabilized 4. Operation needed for associated injuries fracture after it has been reduced -eg: arterial damage *for powerful muscle pull (# femoral shaft)5. Fracture need internal fixation to hold it (ORIFdifficult to reduce by manipulation (need Open Reduction Internal Fixation) mechanical traction) Method to do it: 1. Used anaesthesia & muscle relaxation 2. X-ray before and after reduction 3. Reduced by 3-fold manoeuver (maybe specific for fracture location & pattern) 1) Traction & counter-traction in line of bone 2) Fragments reposition as they disengage -by reversing original direction of force -manipulation to disimpact fragments 3) Alignment adjusted in each plane -continued manipulation to press the distal fragment into reduced position 4. Correct/restore length, rotation & angulation 5. Immobilize joint above and below (put on splint) Successful reduction indicated by 1. Restoration of normal surface anatomy 2. Rapid improvement in pain & neurovascular deficits *CMR= closed manipulative reduction 2. HOLD Aim ‘immobilization’ avoided- because objective seldom complete immobility ‘Splint the fracture, not the entire limb’ 1. To prevent displacement 2. To restrict movement to reduce pain 3. To promote soft-tissues healing 4. To allow free movement of unaffected parts NON-OPERATIVE Methods OPERATIVE Methods Indication Indication 1. Fracture with intact soft tissues 1. Fracture with severe soft tissues damage 2. Inherently unstable fractures 3. Multiple fractures 4. Fractures in confused or uncooperative Methods patients 1. Sustained traction 2. Cast splintage Methods 3. Functional bracing 1. External fixation 2. Internal fixation NON-OPERATIVE METHODS 1. Sustained traction (continuous traction) Principle Traction applied to distal limb of fracture (exert a continuous pull in long axis of bone) Need counterforce pressure Indication Useful for spiral fractures of long bone shafts (femur/tibia) & displaced by muscle pull Avoided in: elderly & younger patients Advantages & Can move joints- thus able to exercise muscles disadvantages Cannot hold fracture still (hold: not perfect) but traction is safe (provided not excessive) Sustained lower limb keep patient in bed for a long time -↑ likelihood of complications -thromboembolism, RS problems, general weakness Technique 1. Traction by gravity Indicated in fractures of humerus- allowing weight of arm to supply traction Forearm: supported by wrist sling, Upper arm: by sleeve cast or brace Balanced skin traction Russell skin traction Fixed skin traction 2. Balanced traction Counter-traction: supplied by raising foot of bed & relying on opposing patient’s body weight Supported for comfort & prevent sagging (eg: Braun’s frame- for tibia #) 3. Fixed traction Same principle as balanced traction Except no counter-traction Limb held in Thomas’s splint (for femur #) Useful when patient has to be transported Skeletal traction Traction by gravity Skin traction -Adhesive strapping by bandages -Weight: no more than 4-5kg -Complication: Vascular compression *we know when to do the surgery Skeletal traction -Stiff wire or pin through bone distal to # -Weight: 20% of body weight -Complication: Pin infection, nerve & vascular injury *preferred of temporizing long bone, pelvic, acetabular # until operative tx *lagi lama dari untuk tunggu operation dari skin traction (don’t know when to do the surgery *patient y under traction – ya kena mesti pergi surgery Traction pin types & placement Thin wire versus Steinman pin 1) Thin wire more difficult to insert with hand drill & requires tension traction bow 2) Steinman pin maybe either smooth or threaded *smooth: stronger but can slide if angled *threaded: weaker, bend easier with higher weigh but not slide & advance easily during insertion -diameter pin for adult: 5-6mm Traction pin placement 1. Sterile field with limb exposed 2. Local anesthesia + sedation 3. Insert pin from known area of neurovascular structure *Distal femur: Medial Lateral *Proximal Tibial: Lateral Medial *Calcaneus: Medial Lateral 4. Place sterile dressing around pin site 5. Place protective caps over sharp pin ends Common Splinting techniques 1. Sugar-Tong -Acute management of distal radial & ulnar # 2. Humeral Shaft # Coaptation -Medially splint ends in axilla and must be well padded to avoid skin breakdown -Lateral aspect of splint extends over deltoid 3. Fracture Bracing -Allow for early functional ROM and weight bearing -Relief on soft tissues and muscles envelope to maintain alignment & length -Commonly used for humeral shaft & tibial shaft fractures Volar/Dorsal forearm -Soft tissue injuries to hand & wrist -Acute carpal bone # (exclude scaphoid/trapezium) -childhood buckle # distal radius Ulnar gutter -4th & 5th proximal/middle phalangeal shaft # -Boxer’s # (distal 5th metacarpal #) Thumb spica -Injuries to scaphoid/trapezium -Non-displaced non-angulated, extraarticular 1st metacarpal # -Stable thumb # ± CMR Buddy taping (dynamic splinting) -Non-displaced proximal/middle phalangeal shaft # & sprains Mallet finger splint -Extensor tendon avulsion from base of distal phalanx ± avulsion # Patella Tendon Bearing (PTB) -molding around tibia condyles -fx: to lock tibia when patient able to partially weight bearing (after 3days of POP) 2. Cast splintage (conversional cast) Type of plaster of Paris 1. Plaster of Paris (OLC- orthopedic casting lab): calcium sulfate (Gypsum) 1. POP (Gypsum) 2. Lime plaster -Indication: distal limb fracture and for most children’s fracture 3. Cement plaster -Cannot be move & liable to stiffness *Adhesion bind muscle fibers to each other & bone (after swelling & hematoma resolve) *How to minimized complication 1) Delayed splintage- use traction until movement regained apply POP 2) Starting with conventional cast until limb can be handled without too much discomfort replace cast by functional brace which permits joint movement 2. Fiberglass (Orthoglass) -strong & lighter (comfortable to use) -cool, water resistant & radiolucent -expensive & difficult to mold Plaster of Paris (POP) -cost-effective, non allergic, easy to mould -heavy & fragile if contact with water -radio-opaque (occlude # line) Splint (eg: slab) or cast? Type Splint/Slab Definition only a part of limb circumference Indication 1. Definitive mx for selected type of #? 2. Soft tissues injuries (sprains, tendons) 3. Acute mx awaiting orthopedic intervention Advantage 1. Allows for acute swelling 2. Decreased risk of complications 3. Faster and easier application 4. May be static (prevent motion) or dynamic (functional; assisting with control motion) Disadvantage 1. Lack of compliance 2. Increase range of motion at injury site 3. Not useful for definitive care of unstable or potentially unstable # Cast encircle whole circumference of limb 1. Definitive mx for simple, complex, unstable, or potentially unstable # 2. Severe, non-acute soft tissue injuries which unable to be managed by splinting 1. More effective immobilization 1. Higher risk of complications 2. More technically difficult to apply Rules of application of POP cast/slab -(length) from 1 joint above to 1 joint below (posterior aspect) -(depth) for Upper limbs: 12-16 layers; for Lower limbs: 16-20 layers of plaster -(width) for Upper limbs: Size 10; for Lower limbs: Size 15 or 20 -backslab: apply in ‘V’ shaped- proximal part of UL/LL bigger than distal part -immobilized in functional anatomy Functional anatomical Elbow: Elbow in 90° flexion, in supination Wrist: Wrist in 25° extension Hand: Metacarpophalangeal in 70-90° flexion, proximal/distal interphalangeal in 5-10° flexion Thumb: ‘holding a soda can’ Knee: Knee in 5-20° flexion Ankle: Ankle in dorsiflexion (no equinus), knee flexion (to relax the gastroc) *always free the distal fingers and toes Cast application steps: 1. Clean skin & apply dressing if there is wound 2. Adequate padding/ortho bandage (min 2 layers- 50% overlap- extra at fibular head, malleoli, patella & olecranon) 3. Soak plaster in water (room °C) till air bubble ceases 4. Apply plaster by unrolling bandage as it rests on limb. Start from distal to proximal. Make sure not too tight or too loose (just follow the limbs) 5. Mould plaster evenly, rapidly & without intervention (used palm, not fingers) -Mold applied to produce 3 point fixation 6. Assess pulse & capillary refill after application After care of POP casts 1. Come immediately if symptoms develop (numbness, tingling, increase pain) 2. Keep plaster cast dry 3. Mobilize all joints which are not incorporated in the plaster to full range of motion 4. Don’t stick anything down to splint to scratch or itch. May lead to injury & infection Local complications of POP Due to tight cast 1. Vascular compression (complaint of diffuse pain, bluish discolouration of digits) 2. Pressure sore/necrosis (complaint localized pain over pressure spot as early as 2H- bony prominence) 3. Compartment syndromes 4. Peripheral nerve injuries (complaint of inability to move fingers, reduce sensation of digits)- direct compressed by bone end or plaster pressure or indirect compressed by oedematous tissue or tourniquet effect or reduced blood flow Due to loose cast (because swelling which occurred after reduction subside) 1. Delay wound healing & produce permanent deformity Due to improper applications 1. Joint stiffness 2. Skin abrasion & laceration (complaint of nipping or pinching during plaster removal) 3. Plaster breakage Systemic complication POP: DVT leading to pulmonary embolism Removing of plaster casts -using plaster shears or electric saw 3. Functional bracing (functional brace) It prevent joint stiffness while still permitting fracture splintage and loading Segmental cast applied to shafts of bone only (leaving joint free) + segmented cast above & below joint connected by metal or plastic hinges (to allow movement in plane) Used for fracture of femur or tibia Brace not very rigid, thus applied only when # begin to unite- after 3-6w of traction or restrictive splintage OPERATIVE METHODS 1. External fixation Principle: Bone is transfixed above and below fracture *with screws or pins or tensioned wires *clamped to frame or connected to each other by rigid bars Applicable to long bones and pelvis but still can be used for fracture of almost any part of skeleton Benefits: 1. Permits adjustment of length and angulation 2. Allow reduction of fracture in all 3 planes Indications: 1. Fractures with severe soft-tissue damage (wound left open for inspection, dressing, definitive coverage) 2. Open fractures (to minimized infection complication with usage of internal fixation) 3. Severe communited & unstable fractures (held out to length until healing commences) 4. Fracture of pelvis (cannot be controlled quickly by any other method) 5. Fracture associated with nerve & vessel damage 6. Ununited fracture (dead or sclerotic fragments can be excised and the remaining ends brought together in the external fixator) Complications: 1. Damage to soft tissue structures (nerves, vessels, tether ligaments, joints) -Crucial to know local anatomy and ‘safe corridors’ for inserting pins 2. Over distraction -If there is no contact between the fragments, union may be delayed or prevented 3. Pin-track infection -Pin-site care is essential + antibiotics immediately if infection occurs 2. Internal fixation Advantage: precise reduction, immediate stability, early movement Disadvantage: sepsis Risk of infection depend upon: 1. Patient- devitalized tissues, a dirty wound, unfit patient 2. Doctor- inadequate training, high degree surgical dexterity, inadequate assistance 3. Facilities- guaranteed aseptic routine, full range implants, staff familiar with use Indications: 1. Fracture that cannot be reduced except through operation (where muscle pull very strong) 2. Fracture that inherently unstable & prone to re-displacement after reduction 3. Fracture that unite poorly and slowly (fracture of femoral neck) 4. Multiple fracture (early fixation reduce risk of general complications) 5. Pathological fractures (malignancy or osteoporosis fractures) Type of internal fixation: (a) Screws Interfragmentary screw (lag screws) For fixating small fragments onto main bone Wires Kirschner wires Often inserted percutaneously without exposing fracture Used in situation where fracture healing is predictably quick External splintage (cast) applied as supplementary support (b) Plates & For treating metaphyseal fractures of long bones & screws For treating diaphyseal fractures of radius & ulna In tubular bones; firm coaptation of fragments achieved by compression devices before tightening the screws Intramedullary For long bone fractures (especially femur & tibia) nails *why not plate? Closed # need to do long incision to skin/muscles - introduce infection delayed union/non-union (bcoz interfere with 1st stage healing & foreign body) A nail (long rod) inserted into medullary canal to splint the fracture ± Locking screws transfix the bone cortices and nail proximal and distal to fracture (resisted the rotational forces) Minimum 2 years: after that may think of taking it out (however Dr Biju said: usually stay forever as it’s not that easy to take it out) (c) Intramedullary nail d) Locked intramedullary nail Complications: (due to poor technique, poor equipment, poor operating condition) 1. Iatrogenic infection- most common cause of chronic osteomyelitis *predispose causes: quality of patient’s tissues & open operation (metal doesn’t predispose infection) 2. Non-union *causes: excessive stripping of soft tissues, unnecessary damage to blood supply, rigid fixation with a gap between fragments 3. Implant failure *due to excessive stress at the fracture site before fracture united (metal subject to fatigue) 4. Refracture *causes: early removal of metal implants & early full weight bearing (several weeks) *removal minimum time= 1 year (safer after 18-24months) 3. EXERCISE ‘Restore function’ Objectives: 1. Reduce oedema (swelling) tissue tension, blistering, joint stiffness 2. Preserve joint movement 3. Restore muscle power SOFT TISSUES CARE 4. Guide patient back to normal activity PRINCIPLE: Elevate & Exercise; Never dangle, Never force Suggested activity: 1. Active exercise 2. Assisted movement (continuous passive motion) 3. Functional activity (everyday tasks) PRINCIPLE MANAGEMENT FOR OPEN FRACTURE Initial management At scene of accident In hospital 1. Splinting the limb 1. Address any life-threatening conditions 2. Cover the wound & left undisturbed 2. Wound inspection -size, shape, tidy or *to reduce risk of further contamination & ragged, clean or dirty, communicate with wound desiccation fracture 3. Assess soft tissues, circulation & nerve supply Gustilo’s classification for open fracture Type I Type II Type III III A III B Puncture wound (<1cm long) Skin damage (>1cm long) Severe, big wound (>10cm) Soft tissue enough to cover wound Soft tissue not enough to cover wound + bone being exposed III C Vascular damage Risk of infection: -Type I: >2% -Type III: >10% -↑ with delay soft tissue coverage *in open # always assume to be contaminated; aim of treatment to prevent from becoming infected Contaminated Infected Passage of bacteria from injury site Bacteria multiply & cause inflammation -early debridement & early antibiotics (Present of body reaction) Principle of treatment of OPEN fracture 1. Urgent wound & fracture debridement -under GA, remove pt’s clothing while maintaining traction on injured limbs -any dressing replaced by sterile pad and surrounding skin cleaned & shaved -pad taken off and wound irrigated thoroughly- using copious amounts of warm normal saline -wound extended and ragged margins excised to leave healthy skin edges -remove all foreign materials and tissue debris -wash wound again (6-12L warm normal saline may needed for irrigation & clean # of long bone) -recognized devitalized tissues, dead muscles and excised them Dead muscles signs: -leave traumatic nerves and tendons (suture if expertise available) 1. Purplish colour 2. Failure to contract 2. Antibiotics prophylaxis (stimulate) Benzylpenicillin + Flucloxacillin or second generation cephalosporin 3. Failure to bleed (when cut) -given 6 hourly for 48 hours Heavily contaminated (cover gram negative & anaerobes) -adding gentamicin or metronidazole and continue treatment for 4-5 days 3. Stabilization of the fracture Method of fixation: 1)degree of contamination 2)length of time from injury to operation 3)amount soft tissue damage Open fracture up to grade IIIA + Treatment same for closed injuries (cast splintage, no obvious contamination + intramedullary nail, plating, external fixation) time lapse <8 Hours (Gustilo classification) More severe injuries Require combine approach by experienced plastic & orthopaedic surgeons 4. Early definitive wound closure Uncontaminated sutured within a few hours of injury (after debridement & incision) wound type I & II Contaminated Left open, lightly packed with moist, sterile gauze inspect again after wound 24-48H *if clean & tidy- can be sutured or skin-graft (delayed primary closure) Wound type III need debridement more than once & need for plastic surgery (for skin closure) Extensive skin Loco-regional fasciocutaneous or musculocutaneous flap loss over Free flap- if blood vessels preserved fracture or blood supply suspected Post-operative treatments 1. Elevated the limbs 2. Careful circulation charting 3. Antibiotics cover is continued 4. If wound left open: inspect again after 2-3days (if much skin loss- need for plastic surgery) IMAGING IN ORTHO- LOWER LIMB HIP JOINT Shenton’s line is formed by the medial edge of the femoral neck and the inferior edge of the superior pubic ramus. Loss of contour of the Shenton's line is a sign of a fractured neck of femur IMPORTANT NOTE: # of femoral neck do not always cause loss of Shenton's line Hip X-ray anatomy - Normal Lateral •The cortex of the proximal femur is intact •The Lateral view is often not so clear because those with • hip pain find the positioning required difficult # proximal of femur Intracapsular a.k.a neck of femur Extracapsular 1. subcapital (below the femoral head) 1. Intertrochateric # 2. transcervical (across the mid-femoral neck) 2. Subtrochanteric # 3. basic cervical (across the base of the femoral neck) Intracapsular # severity :GARDEN CLASSIFICATION I - Incomplete or impacted bone injury with valgus angulation ofthe distal component II - Complete (across whole neck) - undisplaced III - Complete - partially displaced IV - Complete - totally displaced Intertrochanteric # •A fracture line runs between the trochanters •There is comminution with separation of the lessertrochanter •Note the fracture does not involve the femoral neck Describe the xray: X-Ray of pelvis and both hip, AP view Look for shenton line (to look any DDH or # NOF) – imaginary line from inferior part of superior pubic ramus & and along the inferomedial border of neck of femur Look any fracture at the bone – ilium, ischium and pubis (acetabulum), Sacrum, head & neck femur Superior pubic ramus &inferior pubic ramus prone to have # in elderly, complained of pain in the pubic region. Treatment painkillers, & immobilise. Any external or internal rotation, look at lesser trochanter - no LT – internal rotation - show LT – external rotation Look for neck and shaft angle – to look any coxa varus or coxa valgus If <125o = varus If >1350 = valgus Management 1. Open reduction + PFN 2. DHS 3. Skin/skeletal traction can be done 4. >60 = rep;acement surgery HIP DISLOCATION A traumatic hip dislocation occurs when the head of the femur is forced out of its socket. It typically takes a major force to dislocate the hip. Car collisions and falls from significant heights are common causes and, as a result, other injuries like broken bones often occur with the dislocation. 2 types: 1. Posterior dislocation(90% of hip dislocation) Femur head is pushed out of the socket in a backwards direction. Leaves the lower leg in a fixed position, with the knee and foot internally rotated 2. Anterior dislocation. Femur head slips out of its socket in a forward direction The hip will be slightly flexed, and the leg will externally rotated and away from the middle of the body. Complication: 1. Nerve injury. The sciatic nerve, which extends from the lower back down the back of the legs, is the nerve most commonly affected. May cause weakness in the lower leg and affect the ability to move the knee, ankle and foot normally. Sciatic nerve injury occurs in approximately 10% of hip dislocation patients. The majority of these patients will experience some nerve recovery. 2. Osteonecrosis. It can tear blood vessels and nerves. Resulting in osteonecrosis (also called avascular necrosis). This is a painful condition that can ultimately lead to the destruction of the hip joint and arthritis. 3. Arthritis. Posterior dislocation of right total hip arthroplasty EWING SARCOMA Second most common malignant bone tumor in children (after osteosarcoma) Location Arise in medullary cavity, usually of long bones in lower extremities Most occur in pelvis and long bones; femur, tibia, and humerus But they can occur in virtually any bone Commonly involves metadiaphysis of long bones Frontal radiograph and lateral radiographs of the femur mottled, osteolytic lesion (blue circle) with poorly marginated edges in the diaphysis of the bone sunburst periosteal reaction (red circle) and lamellated periosteal reaction (white arrows) degrees better evaluated with MRI Permeative (small holes) or moth-eaten (mottled) appearance Rarely, they can be sclerotic Soft tissue mass may occur without destruction of cortex and may produce saucerization (scalloped depression in cortex) Lamellated - onion-skinning due to successive layers of periosteal development Sunburst or spiculated - hair-on-end appearance when new bone is laid down perpendicular to cortex along Sharpey’s fibers Codman’s triangle - formed between elevated periosteum with central destruction of cortex Osteosclerosis may be present secondary to reactive bone formation