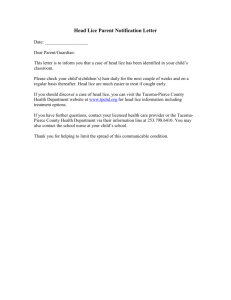
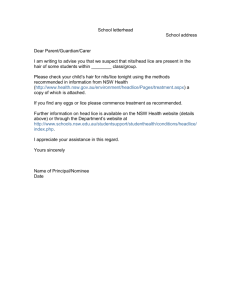
1784 Chapter 55 s P E D I AT R I C I N T E G U M E N TA R Y D I S O R D E R S f. Note scratching and apply age-appropriate interventions. 3. Administer oral antipruritic medications. a. Give medications exactly as prescribed. b. Note the degree of sedation and presence of scratching. Preventing Infection 1. Assess and treat secondary infection. a. Observe the skin for signs of bacterial, viral, or fungal infection (discharge, oozing, crusts, increased redness, fever). Report any positive findings. b. Administer medications, as prescribed. c. Loosen exudate and crusts with water or wet dressings, unless otherwise specified. d. Note changes in the skin in response to therapy. Family Education and Health Maintenance 1. Teach patient and family to avoid potential precipitants, including: Table 55-1 a. Exposure to excessive heat and cold or extremes of humidity. b. Contact with wool and occlusive synthetic fabrics. Soft, lightweight cotton fabrics are preferred. Infants should not be allowed to crawl on wool carpeting. c. Participation in strenuous athletic activities that promote sweating. Activities should be modified according to the needs of the child. Swimming is recommended in chlorinated pools, although bromine in pool water may be irritating. The child should shower afterward and apply a lubricant or other topical medication. NURSING ALERT Advise family that fresh water (pond, lake, river) should be avoided if child has breaks in skin integrity, due to risk of infection. d. Use of irritating soaps, perfumes, detergents, and chemicals. Common Pediatric Skin Problems DISORDER/ORGANISM CLINICAL MANIFESTATIONS Impetigo Bacterial infectious disease affecting the superficial layers of the skin and characterized by the formation of vesicles, honey-colored crusts, or bullae. Etiology and incidence: s Caused by Staphylococcus aureus and Streptococcus pyogenes. Occurs most commonly when personal hygiene is poor. s Common in children younger than age 10. s Spread by close contact—easily conveyed from person to person via hands, nasal discharge, shared towels, toys; plastic wading pools in summer—when water is not replaced and no disinfectant is used; highly contagious. s An abrasion of skin may serve as a portal of entry. Diagnosis: s Usually clinical. s Rarely, a culture of the lesion’s exudate is indicated to confirm the diagnosis. s Incubation period is 1–10 days. s Lesion first appears as pink-red macules that quickly change to vesicles, which, in turn, rupture, develop crusts, and leave a temporary superficial erythematous area. s Bullous (neonate and older child)—large, thin-roofed blisters break to form thin, light-brown crusts. Lesions may occur anywhere on the body but are more common on the face, axillae, and groin. s Crusted (preschool age—seen more commonly in summer on exposed body parts)—lesions appear with thick, yellow crusts; skin around crusts is red and weeping with satellite lesions. s Regional lymphadenopathy is common with secondary infection of insect bites, eczema, poison ivy, and scabies. s Autoinoculation is major cause of spreading. s Pruritus may occur. Ringworm of the Scalp (Tinea Capitis) (See page 1168 for ringworm of the body [Tinea corporis]) A fungal infection of the scalp and hair follicles Etiology and incidence: s Most ringworm of the scalp is caused by Trichophyton tonsurans. Microsporum canis and Microsporum audouinii are also causative agents. s Is seen primarily in children before puberty (usually ages 3–10). s May be spread through child-to-child contact as well as through the common use of towels, pillows, combs, brushes, and hats. Cats and dogs may also be the source of the infection. s The lesions appear on the scalp in a variety of ways: s One or more patchy areas of dandruff like scaling with little or extensive alopecia (hair loss). s One or more discrete areas of alopecia with tiny broken hairs. s Numerous discrete pustules or excoriations with little alopecia. s A kerion or boggy, tender, inflammatory mass that produces edema and pustules. s Pruritus usually occurs in the involved area. (c) 2015 Wolters Kluwer. All Rights Reserved. 1785 D E R M AT O L O G I C D I S O R D E R S 2. 3. 4. 5. e. Avoidance of stressful situations, when possible. f. Foods that are associated with skin reactions (see “Food Allergies,” page 1031). g. Identified other allergens such as pets, live Christmas trees, cigarette smoke, stuffed animals, and objects that harbor dust. Encourage mothers to breast-feed and follow a hypoallergenic diet to decrease the risk of atopic dermatitis. Advise parents and caregivers to follow the American Academy of Pediatrics guidelines of delaying the introduction of solid foods until age 6 months and dairy products until age 12 months for infants at risk for food allergies. Make sure that the family knows the common triggers to avoid, how to prevent dry skin, signs of flares or secondary infection, when to apply topical medications, and the need for routine follow-up appointments. Recommend consultation with dermatology specialist for children with severe or persistent atopic dermatitis. 6. Suggest locating additional information from the following websites: a. American Academy of Dermatology (www.aad.org) b. American Academy of Pediatrics (www.aap.org) c. National Eczema Society (www.eczema.org) 7. Stress the importance of regular health maintenance examinations, immunizations, and preventive practices. Evaluation: Expected Outcomes s s s s Skin intact with minimal erythema and lichenification. Names common triggers and avoidance measures. Verbalizes less itching; less scratching observed. No signs of secondary infection. Other Dermatologic Disorders See Table 55-1. TREATMENT/PREVENTION NURSING CONSIDERATIONS Based on etiology and type of infection. s Gently wash affected area with soap and water three times per day. s Crusts and debris can be removed from the affected area by gentle soaking or wet compresses. Use tap water, normal saline, or 1:20 Burrow’s solution. * If indicated, obtain lipid drainage or debris for culture before antibiotics are provided. s Apply topical antibacterial medication, such as bacitracin or mupirocin ointment or retapamulin. s Systemic antibiotics (cephalosporins, erythromycin, or dicloxacillin) if widespread or recurrent. s Methicillin-resistant S. aureus infection is common. s Prevention—close contact with other children should be avoided until 24 hours after treatment is initiated. s Assess the child’s skin condition and document the location and appearance of lesions. Note new lesions. s Initiate and teach measures to prevent the spread of infection. s Engage in frequent hand washing. Use separate towels. s Daily bathing with soap and water. Regular laundering for contaminated bed linens, towels, and clothing. s Observe drainage and secretion precautions for 24 hours after the start of therapy. s Isolate the child from direct contact with other children (school or day care) until 24 hours after treatment has started. s Trim fingernails and toenails. Apply small amount of bacitracin or mupirocin ointment under the fingernails to prevent the spread of infection. s Engage the child in diversional activities to discourage scratching. s Be aware that the patient with streptococcal impetigo has an increased risk of acute glomerulonephritis. s Micronized griseofulvin—an antifungal antibiotic that is administered orally, 15–20 mg/kg/day (maximum 1 g) in a single dose with a high-fat food for 4–12 weeks. Some children may require higher doses or micronized griseofulvin 20–25 mg/kg/day or ultra-micronized griseofulvin 5– 10 mg/kg/day (maximum 750 mg). s Topical antifungal medicines are not effective. Selenium sulfide lotion 2.5% used twice per week decreases fungal shedding and may curb the spread of infection. s Treatment should be continued for 2 weeks after clinical resolution. s Assess the scalp for characteristic lesions. s Administer or teach the patient and family to administer medications as prescribed. s Be aware of adverse effects, such as headache, heartburn, nausea, epigastric discomfort, diarrhea, urticaria, photosensitivity, and possible granulocytopenia caused by griseofulvin. s Griseofulvin is absorbed more efficiently with a fatty meal. Children can be given the medicine once per day with ice cream or peanut butter. s Liver function monitoring may be required for prolonged treatment (greater than 6 months) or for children with baseline abnormal liver functiion. (continued) (c) 2015 Wolters Kluwer. All Rights Reserved. 1786 Chapter 55 s P E D I AT R I C I N T E G U M E N TA R Y D I S O R D E R S Table 55-1 Common Pediatric Skin Problems (continued ) DISORDER/ORGANISM CLINICAL MANIFESTATIONS Ringworm of the Scalp (Tinea Capitis) (continued ) Diagnosis: s Hair or skin scrapings for microscopic evaluation or fungal culture, obtained by rubbing a swab or toothbrush over the affected area. Differential diagnosis: s Tinea amiantacea, lichen planopilaris, and perifolliculitis capitis abscendens et suffodiens must be ruled out clinically or histologically. Woods lamp inspection has limited benefit. Pediculosis Infestation of humans by lice. Etiology: s Three types of lice affect human beings: s Pediculosis capitis (head lice)—commonly infests school-age children. s Pediculosis corporis (body lice)—rare in the United States. s Pediculosis pubis (pubic or crab lice)—common in sexually active adolescents or adults—can be found on pubic hair, chest hair, axillary hair, eyebrows, eyelashes, and beards. s Each type of louse generally remains in the area designated by its name. s Lice are transmitted by personal contact with people harboring them or through contact with articles that temporarily harbor them (clothing or bed linens). s Head and pubic lice are not health hazards or signs of uncleanliness. Only body lice can transmit disease. Diagnosis: s Identification of lice or their eggs with the naked eye confirmed by using a hand lens or microscope. s In active infection of head or pubic lice, nits and eggs are found on the hair shaft within 1 cm of the skin and are difficult to remove. s Body lice and their eggs are found in the seams of undergarments. s Itching in the area affected is the primary symptom of pediculosis. Scratch marks may be evident in these areas. However, not all affected people itch. s Other signs of infestation are pillows or clothing that look unusually dirty. s Infested scalp areas may become secondarily infected from scratching. s Crusts, lice, nits, eggs, and dirt may combine to cause a foul odor and matted hair. s Body lice may produce minute red lesions. (c) 2015 Wolters Kluwer. All Rights Reserved. D E R M AT O L O G I C D I S O R D E R S 1787 TREATMENT/PREVENTION NURSING CONSIDERATIONS s Treatment with oral itraconazole, oral terbinafine, or oral fluconazole is effective, but only terbinafine has been approved by the Food and Drug Administration for this disorder. s Teach the child and family methods to prevent further episodes. s Teach general hygiene measures—regular shampooing and bathing. s Advise them to avoid sharing hats, combs, brushes, pillows. s Routine cleaning of heavily contaminated articles, such as pillowcases, sheets, towels, hats, bike helmets, combs, brushes. s All family members and close contacts should be screened for tinea infections. The child’s school should be notified to facilitate the screening of classmates. s Hair loss is usually temporary, except in some cases with a kerion, when the hair follicles may have been destroyed. s Child may attend school after treatment has been initiated. Hats are not necessary. s Pediculosis capitis and Pediculosis pubis may be treated with over-the-counter agents, such as permethrin or natural pyrethrin-based products. Lindane 1% (Rx) is indicated for second-line therapy only. Natural pyrethrin-based products and lindane may be reapplied 7–10 days later. Lindane should be avoided in children younger than age 2, people with known seizures, and pregnant or lactating women. s For infestation of eyelashes by crab lice, petroleum jelly applied twice daily to the eyelashes for 8 to 10 days is effective. s Pediculicides are not necessary for the treatment of Pediculosis corporis. Washing infested clothing and linens, where the lice harbor, in hot water and machine drying (on hot cycle) is adequate. s Because pediculicides kill lice shortly after application, the detection of living lice on scalp inspection 24 hours or more after treatment suggests incorrect use, reinfection, or resistance. Immediate retreatment with a different pediculicide followed by a second application 7 days later is recommended. s A suffocation-based pediculicide (DSP) lotion applied and then blown dry with a hair dryer weekly for up to 3 weeks effectively treats 95% of head lice. The hair can be shampooed 8 hours after application. The lotion is not visible and the hair can be styled. s Studies of the efficacy of suffocation of lice by the application of occlusive agents, such as petroleum jelly, olive oil, or mayonnaise, have not been performed. Cotrimoxazole and ivermectin have been shown to be effective, but neither is approved by the FDA as a pediculicide. s “No nit” policies requiring children to be free from nits for the return to school do not reduce transmission and are not recommended. s Shaving head is not necessary. s Administer or teach administration of antiparasitic as directed. Natural pyrethrin-based products work best on dry hair. Avoid shampoo, cream rinses, and conditioners before application. s Although both pyrethrins and permethrin are quite safe, limit exposure to the skin by rinsing the hair in a sink rather than the shower and use cool water to minimize absorption from vasodilation. s Removal of nits with a fine-tooth comb may be attempted for aesthetic reasons or to decrease diagnostic confusion. However, mechanical removal of nits after treatment does not prevent spread. s Inspect the scalp (or have the family inspect the scalp) 24– 48 hours after treatment to see what lice remain. The presence of large lice may mean that the treatment was ineffective or that the lice are resistant. s Provide appropriate teaching for the family to prevent recurrences. s Wash clothing, bed linens, and towels in hot water and machine dry (on hot cycle). Temperature above 128.3° F (53.5° C) for 5 minutes will kill lice and eggs. Dry cleaning or simply storing contaminated articles in a well-sealed plastic bag for 10 days is also effective. s Teach children not to share combs, brushes, head gear or hats. Combs and brushes can be disinfected by soaking in hot water for 10 minutes or washing with a pediculicide shampoo. s Environmental insecticide sprays are not helpful. Vacuuming carpets and car seats is a safe alternative. s Household, other close contacts, and classmates of the child with head lice should be screened for parasites and treated if affected. Prophylactic treatment of head lice is unnecessary and may increase resistance. Notify the child’s school or day care so classmates can be screened. s Children should be allowed back to school or day care the morning after their first treatment. “No nit” policies for the return to school are unnecessary. s Prophylactic treatment of all sexual contacts of adolescents and adults with pubic lice is warranted because of the high co-infection rate. (continued) (c) 2015 Wolters Kluwer. All Rights Reserved. 1788 Chapter 55 s P E D I AT R I C I N T E G U M E N TA R Y D I S O R D E R S Table 55-1 Common Pediatric Skin Problems (continued ) DISORDER/ORGANISM CLINICAL MANIFESTATIONS Scabies A disease of the skin produced by the burrowing action of a parasitic mite in the epidermis, resulting in irritation and the formation of burrows, vesicles, or pustules Etiology: s The mite, Sarcoptes scabiei, is the cause of this disorder. s Occurs in people of all socioeconomic levels, regardless of personal hygiene standards. s Is transmitted by direct skin contact with infected people or by indirect contact through soiled bed linens, clothing. Diagnosis: s Identification of a mite, ova, or feces from skin scrapings. s Often based on clinical presentation. s Itching, particularly at night, is the primary symptom. The onset of itching is usually insidious. s Secondary skin infection is common and may confuse the diagnosis. s Systemic manifestations are absent, unless they result from the secondary infection. s The burrow, a gray or white, tortuous, threadlike line, is seen most commonly in older children and adults between the fingers, in the wrists, in the axillary and buttock folds, along the belt-line, on the male genitalia, on the female breasts, and on the knees, elbows, and ankles. s In infants and small children, the lesions may occur on any part of the body and are usually widespread. Vesicles on the palms and soles are characteristic. s Incubation period in children without previous exposure is 4–6 weeks. Oral Candidiasis (Thrush) Oral candidiasis is a mycotic stomatitis characterized by the appearance of white plaques on the oral mucous membranes, gums, and tongue. (Chronic mucocutaneous candidiasis may be associated with endocrine diseases or immunodeficiency disorders or use of systemic antibiotic or inhaled corticosteroids.) Etiology: s Caused by Candida albicans. s Maternal vulvovaginitis is the primary source of neonatal thrush. Evaluate for endocrine diseases or immunodeficiency disorders if thrush occurs after 6 months of life or is chronic. s Nipples, pacifiers may be reservoirs. s The infant develops small plaques on the oral mucous membranes, tongue, or gums. These plaques look like curds of milk but cannot be wiped out of the mouth. s Most infants with thrush appear to have little pain or discomfort, unless the case is severe and there is erosion and ulceration of the mucosa. s The mouth may be dry. s Occasionally, the infant may appear to have some difficulty swallowing or may eat less vigorously. s Enteric infection is usually associated with oral thrush. Diaper Dermatitis Candidal diaper dermatitis—a rash characterized by bright red, sharply circumscribed but moist patches with pustular satellite lesions Etiology: s 80% of diaper rashes present for 3 or more days are caused by Candida albicans. s Most commonly seen in infants and toddlers who wear diapers. s May be associated with oral candidiasis. s Buttock rash consisting of erythematous maculopapular eruption with perianal distribution. s Generally causes discomfort, especially with wetting and cleanings. Lesions last approximately 2 weeks, desquamate, and resolve without scarring. (c) 2015 Wolters Kluwer. All Rights Reserved. D E R M AT O L O G I C D I S O R D E R S 1789 TREATMENT/PREVENTION NURSING CONSIDERATIONS s Application of a scabicide to the skin: s The drug of choice is 5% permethrin. Alternative drugs are lindane 1% and crotamiton. Permethrin should be removed after 8–14 hours by bathing, lindane after 8–12 hours, and crotamiton after 48 hours. s Lindane can cause neurotoxicity from absorption through the skin. It should be avoided in children younger than age 2, people with known seizures, pregnant and lactating women, and people with extensive dermatitis. s Infected children and adults should apply the scabicidal lotion or cream on the entire body from the neck down. The entire head, neck, and body of infants and young children should be treated. Bathing immediately before treatment should be avoided. s Oral ivermectin at 200 mcg/kg/dose is not FDAapproved, but has been shown to be effective. s People caring for affected children should wear gloves. s Contagion is unlikely 24 hours after treatment. Children may return to school or day care. s Teach the patient and family to launder all clothing, bed linens, and towels used by the patient during the 4 days prior to therapy with hot water and hot drying cycle to kill mites. Clothing that cannot be laundered can be stored in a plastic bag for 1 week. Further environmental disinfection is rarely necessary. s Itching may continue 2–3 weeks after successful therapy due to a hypersensitivity reaction to the mites. The use of oral antihistamines and topical corticosteroids can help relieve symptoms. s All household and close contacts should be treated prophylactically and at the same time to prevent reinfection. Caretakers with prolonged skin-to-skin contact with infected patients may also benefit from prophylactic treatment. Manifestations of scabies can occur as late as 2 months after exposure. s Topical administration of nystatin in suspension three to four times daily is the treatment of choice. Apply ½ doses to each side of the mouth after feeding. s Retain in mouth as long as possible before swallowing. Allow the child to swallow any medication to treat any lesions along the GI tract. s Clotrimazole troches can be used in children older than age 3. s Amphotericin B, clotrimazole, ketoconazole, fluconazole, and newer antifungal agents are used for candidiasis resistant to nystatin. Not all of these drugs are approved for use in infants and children. s Recognize the appearance of thrush. s Be aware of the infant or child who is particularly susceptible to the development of this condition, especially normal infants younger than age 6 months, low-birth-weight infants, immunocompromised or debilitated hosts, and people on prolonged, broad-spectrum antibiotics. s Teach parents to inspect the child’s mouth before every feeding for presence of thrush and report the appearance of thrush. s Keep the affected area clean and dry by frequent diaper changes. s Clean the skin with water-based, alcohol-free baby wipes with a pH of 5.5 or with water. s Use disposable diapers with sodium polyacrylate polymers in the diaper core that form a gel when hydrated to keep liquid away from the skin or a breathable diaper. s Topical application of nystatin, clotrimazole, or miconazole cream or ointment after gentle cleaning of the affected area. If no improvement in 2 days, consider nonadherence, failure to relieve aggravating factors, or need for a different drug. s Nystatin may be given orally if rash is persistent. s Burrow’s solution compresses for severe inflammation or vesiculation. s Low-potency topical corticosteroids for short-term use may be added. s Teach parents the general principles of prevention. s Change diaper as soon as possible after wetting or soiling. Prolonged contact of feces with the skin promotes the development of candidal diaper dermatitis. Check diaper frequently (every 3–4 hours). Encourage use of disposable diapers. s Wash entire diaper area with warm water or use water-based, alcohol-free baby wipes. s If using cloth diapers, use a second hot rinse when washing diapers to neutralize ammonia produced when infant urinates; use vinegar, Borax, or Diaparene in wash. s Avoid powder and oil, which tend to clog pores and cake on skin, retaining bacteria. s Avoid occlusive plastic coverings, and tightly pinned or double diapers, all of which tend to increase production and retention of body heat and moisture. s Allow the infant to go without a diaper for short periods to leave area open to air. s Diaper rashes present for 3 or more days should be evaluated by a health care provider. (c) 2015 Wolters Kluwer. All Rights Reserved.