Language Processing & Aphasia: Individual Differences & Recovery
advertisement

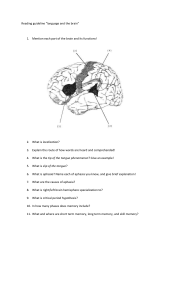
1 Individual differences 1. What individual characteristics may affect the way one processes language? a. education, age, second language proficiency, cognitive resources, socioeconomic status (modulates how much input you get) 2. Sources of language variation a. External to the cognitive system - effects of experience, education and second lang proficiency b. Internal to the cognitive system - each of us are a bit different and have different strengths i. Brain functioning, working memory capacity, and language aptitude 3. Study for education? a. Pakulik & Neville language proficiency differences in English monolinguals impacts syntactic processing in their native language = smarter kids better at grammar 4. Study for age? a. Park et. al.- cognition gets worse as we age (duh) b. Ben-David et. al.- takes longer to recognize spoken words as we get older c. Botezatu-older people slower at spoken-to-written word matching task 5. Study for cognitive resources? a. Color Stroop Test: inhibition is one of the cognitive resources 6. Second language proficiency: both languages are activated all the time a. Intuitively, lower L2 proficiency is associated with slower, more error-prone L2 retrieval. b. Counter-intuitively, lower L2 proficiency is also linked to lexical retrieval difficulties in the stronger native language. 7. What variables predict/modulate recovery from acquired language disorders? a. Severity, motivation, therapy, access to services, family support Aphasia Etiology and Recovery 1. Frontal lobe: a. Executive functions- working memory, planning, memory, motor or social, speaking, reasoning/judgement, voluntary motor activity, b. Individuals with lesions- behavioral problems, apathy, disinhibition/aggressiveness, loss of flexibility with thinking, limited attention to task, mood changes c. Broca's area → spoken area 2. Parietal lobe: a. Sensation of touch, Spatial sense-proprioception/body orientation, reading b. Primary motor and sensory area 2 3. 4. 5. 6. 7. 8. 9. c. Impairment- inability to attend to more than one object at a time, difficulty recognizing left v right, hand eye coordination problems, impaired perception of touch, difficulty drawing objects Temporal lobe: a. Language comprehension, behavior, memory, hearing b. Wernicke’s area-language comprehension c. Primary and secondary auditory areas → auditory perception d. Impairment- difficulties understanding spoken words, poor selective attention, loss of short term memory, persistive talking, increased aggressive behavior Occipital lobe: a. Visual cortex-color shape and emotion distinguishing b. Impair-vision right visual field, blind spots, locating objects, recognizing drawn objects, inability to recognize movement of an object in space, difficulty identifying color, word blindness, difficulty reading/writing Cerebellum: a. Doesn’t integrate motor activity, Coordinates and controls movements of fine motor tasks (speaking), Regulates balance and posture i. Helps provide smooth, coordinated body movement b. Online correction planned movements c. Impairment- lack of coordination, abnormal gait, errors in judgements of movements Brainstem: a. Eye movements, sneezing, gagging, coughing, breathing, body temperature, digestion, alertness/sleep b. (midbrain, pons, medulla) Insula a. Also known as the 5th lobe b. Placed “under” the lobes c. Interception - how we tune into ourselves, feelings, emotions, CVA a. A disturbance in the blood supply to the brain, lasting only seconds, can cause neurological symptoms and irreversible neuronal brain damage, in minutes. b. A CVA occurs when there is a lack of blood flow to any area of the brain including the brainstem. c. CVAs are the 3rd most common cause of death in the U.S. with a mortality rate of about 33%., It is the leading cause of disability in U.S., Approximately 550,000 strokes occur annually. Risk of stroke a. Gender- men 3 b. c. d. e. Race- African American/ asian Age- mortality rate 10% higher for people over age 65, increases Family history of stroke Medical conditions- diabetes, smoking, excessive alcohol consumption, obesity, sedentary lifestyle 10. Symptoms of a Stroke: a. Sudden numbness or weakness of face, arm or leg, especially on one side of the body b. Sudden confusion, trouble speaking or understanding c. Sudden trouble seeing in one or both eyes d. Sudden trouble walking, dizziness, loss of balance or coordination e. Sudden severe headache with no known cause 11. Ischemic vs. hemorrhagic stroke a. Ischemic strokes are caused by a clot that stops blood supply to an area of the brain i. Accounts for 85% of strokes ii. If the clot is moving = embolism iii. Clot is not moving = thrombus iv. Transient Ischemic Attack (TIAs) 1. Warning stroke that says a bigger one is coming that will have more lasting effects 2. Result of cerebroartery being temporarily blocked 3. Shorter than 5 min but average = 1 min 4. No permanent injury to the brain 5. Should cut down smoking and drinking and increase healthy eating/living habits v. Tissue Plasminogen Activator (tPA) - used to break down/dissolve blood clot and limit extent of lesion 1. Brain needs to be reprofused 2. Only given if suffering from ischemia, if it is a hemorraghic stroke then the damage would be catastrophic if given tPA b. Hemorrhagic strokes are caused by blood leaking into brain tissue i. Account for 15% of strokes ii. Abnormal bleeding causes less blood elsewhere iii. Damage where the blood enters the brain tissue and where blood is not going iv. Emergency surgery may be needed to resolve blood leakage and relieve pressure on the brain v. More dangerous than ischemic → 50% mortality rate 12. Middle cerebral artery (red) damage; aphasia 4 a. Middle - largest of all cerebral arteries b. Yellow - anterior cerebral artery c. Blue - posterior cerebral artery 13. Brain Imaging tools to diagnose stroke a. CT scan or CAT scan b. MRI c. MRA d. Carotid doppler ultrasound (less invasive) 14. Global aphasia: a. Lesion: Large portion of the perisylvian area b. Blood Supply: total occlusion of the left MCA c. Limited to stereotypical utterances (hohohho), song refrains, sequences (days of the week) d. Severe impairment in comprehension, production, reading and writing, severe motor deficits to the right side of body, hemiparesis obvious 15. Broca’s Aphasia a. Lesion: 3rd frontal convolution b. Blood Supply: left MCA c. Effortful speech, nonfluent, produce short phrases or single words, telegraphic speech, communicate using nouns and verbs no function words, preservation of counting, days of week, cursing (Norton), d. Comprehension relatively spared but some difficulty with complex syntactic structures e. Writing also impaired, also naming 5 16. Wernicke’s Aphasia a. Lesion: posterior left perisylvian region b. Blood Supply: left MCA c. Difficulty understanding language, phonemic and semantic paraphasias, utterances are void of meaning, can listen to speech and not understand, no awareness of deficit, cannot monitor output, repeating and naming is impaired 17. Conduction Aphasia a. Lesion: arcuate fasciculus b. Blood Supply: left MCA c. Fibers that connect brocas to wernicke's d. Difficulties repeating what they heard, fluent speech, word finding difficulties, will try to correct themselves, conducite d’approche- phonemic variations (try to say a word like it but often fail phonemic like production error and not semantic like circumlocution) comprehension spared e. Word finding for ALL aphasia types f. Fluent aphasia subtype 18. Anomic Aphasia a. Lesion: varies (little or no localization value) b. Blood Supply: left MCA c. Tip of tongue effect most severe, circumlocution d. The best one/easiest one to have e. Word retrieval issues, aware of deficit f. Aware of nature of object but cannot get it upon request (may be able to say when they aren’t directly trying to find it) g. Aware of name they are trying to say so they will try to do a roundabout way to get there h. Rarely Make phonemic and semantic errors i. Good comp, reading, writing, repetition j. Fluent subtype 19. Transcortical Aphasias a. Results from an isolation of the perisylavian language zone of the left hemisphere from the rest of the cortex. b. Characterized by a disproportionately preserved capacity of repetition. c. Disproportionate capacity to repeat 20. Transcortical Motor Aphasias: a. Lesion: frontal region anterior/superior of Broca’s area. b. Blood Supply: left ACA c. Reading and writing impaired, able to repeat long complex sentences d. Resembles Broca’s aphasia but difficulty with responding 21. Transcortical Sensory Aphasias a. Lesion: posterior to the perisylvian region, in the parietal occipital region b. Blood Supply: left PCA 6 c. Comprehension impaired across the board, fluent but unintelligible and meaningless → word salad d. Can repeat but severe impairment in comprehension of oral and written naming 22. Recovery vs. Compensation a. Recovery is the capacity to perform previous non impaired tasks as they were before injury b. Compensation is the use of a new strategy to perform old tasks -- part of brain cannot perform previous duties so other tissue nearby takes over the some of the function in order to carry through to produce the old ability 7 23. Patterns of Recovery: repair, reorganize, rehabilitate a. Repair - physical repair i. Disrupted physiologic functions improve ii. Scar tissue of dead tissue appear iii. First 3 mo b. Reorganization i. Areas nearby start to take over ii. Many not be nearby iii. 3-12 mo c. Rehabilitation i. Retraining to perform specific tasks ii. Work on building new pathways to perform functions they have lost iii. 1 year post-onset d. Immediately there is a period of shock and functions will appear to be more severe than they will end up having – swelling goes down, other places will try to take on new functions, e. Rapid recovery in hours and days following trauma f. There is steady progress months g. Improvement rates decrease as months and years go by h. Recovery does not end after 1 year – people have been known to make progress years and years after 24. Behavior Mechanisms of Recovery a. Reactivation of temporarily impaired language function – direct simulation, repetition, indirect simulation – cueing strategy that offers supports for retrieval, b. Reorganization – fill in the missing blank of the functional system, phonemic self cueing to overcome word finding difficulties, c. Relearning - reestablish lost rules and info (grapheme-phoneme correspondence d. Facilitation – when difficulty accessing information e. Functional substitution – implies that a function cannot recover in original system so another area substitutes for system loss – think AAC 25. Factors affecting recovery: a. Neurologic i. Etiology of injury (Ischemic vs. hemorrhagic) ii. Size and site of the lesion iii. Aphasia severity/type b. Individual differences i. Age ii. Health status iii. Gender iv. Depression c. Nonfluent aphasia has better prognosis 8 d. Anomic have slower progress but better functional communication Life Quality Approaches to Aphasia 1. Disempowerment a. Intense feelings of frustration and depression b. Less willing to take have the patients to wait for someone to get to where they retrieve what they want to say or get to the point c. What would they want to know about their deficits and treatment → 5 main desires: access to information (therapist fail to explain what aphasia is and what a the long term effects are), to regain control and independence (using the phone, license, learning to use the bus, grocery shopping), lack of respect, loss of worth and career opportunities (strong desire to return to some form of work, reorient to a new career path, contribute to society), Qualitative 1. Health Related Quality of LIfe: medical condition, structure function impairment, task limitations, participation restrictions a. Concern of impact on the health on their quality of life b. This is based on subjective rating of the 4 above c. All have a negative impact socially and personally 2. ICF: Body functions, activities, and participation 3. Framework for outcome measurement 9 4. Emotional Responses to Aphasia a. Those who have a stroke and aphasia are more likely to suffer from emotional distress compared to those who had strokes without aphasia b. Lower quality of life c. Lower levels of engagement d. Harder to make best of rehabilitation opportunities e. These emotional responses will change over time f. The symptoms are more dramatic in acute phases in comparison to subacute g. Constant fatigue and feelings of disoriented 5. Factors predicting depression on those with aphasia a. Outcome factors b. Social factors 6. Purpose of assessing quality of life a. In the acute phase -- assess/screen for depression, if they do then they would be referred for treatment b. In the rehabilitation hospital – need info for the purpose of treatment planning, you wear two hats: clinician and researcher, they have predictive power over outcome Quantitative 1. Dartmouth COOP charts a. Scale of 1-5 that is associated with pictures of stick figures b. EX - during the past four weeks...has your physical and emotional health limited your social activities with family, friends, neighbors or groups? 2. Stroke Specific Quality of Life Scale a. Scale of 1-5 without pictures 10 3. Stroke and Aphasia Quality of Life Scale a. Scale of 1-5 from definitely yes to definitely no 4. ALA: Assessment for Living with Aphasia a. Picture scale on a spectrum from 1-8 b. Aphasia is a big problem → no problem c. Never → always d. Happy → not happy Cognitive Processes Word Recognition & Production 1. Word recognition a. Cognitive model: concept->lexical->phonological->sound form b. Fewer competitors easier to recognize than lots of competitors c. Aging--you get worse 2. Word production a. Semantic Feature Analysis b. Lexical-Phonological Analysis c. Lexical-Semantic Variable i. Frequency ii. Imageability iii. Word length iv. Lexicality d. Retrieval practice better than imitation: errorless learning not as good Client Centered Approach 1. Empathetic understanding, unconditional positive regard, therapeutic genuineness 2. Counseling → greive what they have lost, coping strategies to get resilience, reintegrate into society 3. Consider relationships that are closest to them and help target strategies to make those social interactions successful Cognitive-Neurophysiological Approaches to Aphasia 1. People associated with the early identification of Aphasia a. Franz Josef Gall: i. Mental functions localized symmetrically on each side of the brain ii. Language is innate -- independent of reason and intelligence iii. Founder of phonology b. Jean Pierre Flourens i. Experimented on birds ii. Says there’s no division of mental capacities into separate locations or functions c. Jean Baptiste Bouillaud 11 i. d. e. f. g. h. i. j. k. l. Identified the connection between the loss of speech and frontal brain damage Paul Broca i. Says “We speak with the left hemisphere” ii. Brain reorganization following damage M. Leborgne (Tan Tan) i. Lost the ability to speak at age 30 - could only speak the syllable “tan” ii. Broca term his disability aphimia or the loss of speech now known as Broca’s aphasia Carl Wernicke i. Described patients whose speech was fluent but had no informational value Adolf Kussmaul i. Individuals with “pure word deafness” can hear, speak, and read but cannot understand speech ii. The lesion isolates Wernicke’s area from the auditory cortex Ludwig Lichtheim (See Wernicke-Lichtheim “House” Model) i. Reported 2 cases: one of a patient who is unable to comprehend and another who was nonfluent, despite preserved repetition in both cases ii. Proposes a modification and extension of Wernicke’s arc by adding a new module that stores concepts (meaning of words) that he calls semantic fields Sigmund Freud i. Rejected the concept of speech centers ii. Emphasized that language deficits should arise from disruption of connecting fibers Constantin von Monakow i. Emphasized the interdependence of different regions of the nervous system ii. Believed that there is a delicate balance between different brain components Kurt Goldstein i. Emphasized that after local injury, the function of more widespread brain regions can be affected because of the interrelatedness of brain components ii. Also focused on how a person reacts after loss of function and described what he called the “catastrophic reaction” Alexander Romanovich Luria i. Emphasized the importance of analyzing syndromes 12 ii. 2. 3. 4. 5. 6. 7. Importance of analyzing the qualitative nature of deficits resulting from brain injury m. Norman Geschwind i. Attempted to explain why particular aspects of language function may break down while others are preserved ii. Parallel systems and alternative pathways Signs and symptoms of Wernicke’s Aphasia a. Speech appears to have not information content b. Preserved function words, impaired content words c. Comprehension impaired d. Associated with left temporal lobe damage e. Patient relatively unaware of deficit Signs and symptoms of Conduction Aphasia a. Damage to arcuate fasciculus b. Fluent speech but containing many paraphasias c. Impaired repetition of words d. Normal language comprehension e. Abnormal word finding / paraphasic Wernicke’s arc hypothesis a. Motor word images are stored in Broca’s area b. Auditory word images are stored in Wernicke’s area Wernicke-Lichtheim “House” Model a. Proposed specific information processing centers each of which was specialized in a specific function b. Each normal higher function is explained in terms of an underlying neural pathway that includes the input/output systems, related functions employ portions of the pathways used for other functions, pathological syndromes are explained by reference to where in the pathway damage occurred, and previously unobserved pathological syndromes can be predicted. What errors might one make when attempting to formulate single words? a. Semantic paraphasia: Cat -> Dog b. Phonemic paraphasia: Cat -> Cap c. Mixed: Cat -> Rat some semantic, some phonemic d. Formal errors: Cat -> gad e. Unrelated errors: Cat -> Mop f. Language production is a semantically driven task g. Language production → word meaning (conceptual preparation) → word retrieval (lexical selection) → word sound (phonemic encoding) Connectionist model: 13 a. Language production is a combination of conceptual preparation, lexical selection, phonological encoding, and motor programming and articulation b. Two stage process: i. Stage 1: lexical selection 1. Semantic description of item to be produced 2. Word that best matches semantic description ii. Stage 2: Phonological retrieval 1. Phonological representation of word c. Start with a concept d. Activate the semantic features in relation to the concept and some features are shared with other concepts e. Select lemma based off of a set of words in which your target will be, the target will have the strongest lemma which means it will win the competition f. Phonological retrieval kicks in to retrieve the phonemes that make up the target words and again wins the competition g. If it fails→ it could happen at all levels h. Strength of connections is important to win out at each step i. j. Bidirectional activation flow i. Semantic features are described/seen ii. Lexical selection iii. Phonological retrieval iv. Even before you make the selection of cat, the phonological retrieval will occur for al the competing words v. The bidirectional flow helps increase cat activation in comparison to others 14 My notes: In all the time it took to make these graphics she could have learned something useful to teach us - lol 8. Cohort vs. Rhyme neighborhood a. Cohort - words that begin with the same onset b. Rhyme - words that end in the same rhyme 9. What types of brain injury can cause pure word deafness? a. Disruption of auditory input to Wernicke’s area b. Damage to Wernicke’s area itself 10. How can you assess pure word deafness? a. Auditory word and non-word repetition tasks b. Auditory discrimination i. Minimal pairs ii. Maximal pairs c. Hearing acuity information 11. How to treat pure word deafness? a. Use lip reading information and mouth drawings to provide additional information about differences between phonemes to improve the client’s ability to discriminate between similar-sounding words 12. Word level errors: Semantic a. You activate semantic features which should boost the lemma selection meaning cat should be a stronger activation b. If the activation of lemma decays before one is able to retrieve phonology then you have a problem c. Not only the strength of connection at the level but the activation of phonemic features to retrieve the word d. Activation of a particular lemma should die down after a while, you should not maintain activation of everything so once phonology is reached you let that shit go àactivation of target and competitors all die out 15 e. Strength between stage 1 can be weakened and you are more likely to make an error 13. Models of spoken word production Disorders of Auditory Comprehension -- needs to be added Disorders of Word production -- needs to be added 1. Lexical-phonological variable: Word length a. Longer words are harder to produce and to repeat than shorter words. Errors will be phonological. 2. Lexical-phonological variable: lexicality a. Comparison of word and nonword repetition can provide information about the route being used 3. Describe errorless learning a. Presenting trails in a way that the learner does not have the opportunity to give or choose a wrong answer through repeated exposure to the correct answer and use of prompting