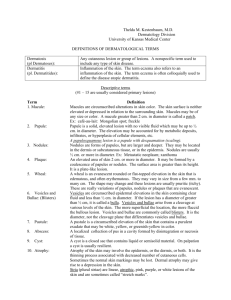
abSTRaCT REviEw Skin changes are common in children. Common concerns are birthmarks (e.g., hemangiomas and port wine stains), atopic and contact dermatitis, acne, and alopecia areata. The authors review advances in common and not so common skin changes in pediatric patients. J Clin Aesthet Dermatol. 2017;10(3 Suppl1):S8–S15 Pediatric Dermatology a LESLIE CASTELO-SOCCIO, MD, PhD, and aPATRICK MCMAHON, MD The Children's Hospital of Philadelphia and University of Pennsylvania Perelman School of Medicine, Philadelphia, Pennsylvania a CUTANEOUS PROBLEMS OCCUR frequently in children; up to 30 percent of pediatric primary care visits involve a skin-related problem.1–4 Common among these problems are atopic dermatitis, seborrheic dermatitis, contact dermatitis, and acne. Yet pediatric dermatology, first recognized in 2000 as a boarded subspecialty of dermatology, is in its infancy.5 Despite the demand, there is a national shortage of pediatric dermatologists, which has made it difficult to impart adequate dermatology training for pediatricians. For this reason, many dermatologists, pediatricians, and primary care physicians manage the pediatric population when it comes to dermatology issues. Education for clinicians is imperative to meet the burden of pediatric dermatology cases, many of which can be highly complex. The aim of this review is to discuss emerging concerns in pediatric dermatology. C Infantile hemangiomas (IH), common tumors in infants with a prevalence around five percent, may be treated in several ways.6 More than half of IH present in the head and neck region (60%).7 It is crucial first to INFANTILE HEMANGIOMAS differentiate between a superficial hemangioma, which may respond to topical therapy, and a deep hemangioma, which is typically treated with oral propranolol. Timolol 0.5%, a gel-forming solution, is the first-line topical treatment for superficial IH.8 Early treatment is highly recommended. Propranolol, a beta-adrenergicblocker, has emerged as a preferred treatment option for complicated IH cases.9,10 As a beta-blocker, propranolol may be associated with changes in the heart rate or rhythm, including symptomatic bradycardia.11 The use of propranolol therapy for IH may vary from institution to institution. In a multiinstitutional survey of treatment practices for IH (n=18 respondents, 15 institutions), respondents at 67 percent of institutions said they routinely consulted with cardiology colleagues before initiating propranolol therapy, and the median dosage of propranolol hydrochloride to start therapy was 2.00mg/kg/d±1.65mg/kg/d (range 0.45– 2.50mg/kg/d). Treatment duration ranged from 4 to 8 months (33%) or 8 to 12 months (67%), and the decision to discontinue therapy was based on clinical response (50%) or patient’s age (43%).12 While guidelines have been Disclosures: The authors have no conflicts of interest relevant to the content of this article. Author correspondence: Dr. Leslie Castelo-Soccio; email: castelosocciol@email.chop.edu S8 JCAD JOURNAL OF CLINICAL AND AESTHETIC DERMATOLOGY March 2017 • Vol. 10 • No. 3 • Supplement 1 REviEw established for the initiation, treatment indications, and clinical monitoring of propranolol therapy for IH, the role of electrocardiography (ECG) testing remains unclear. There is no consensus as to whether it is required for pretreatment evaluation. The use of routine ECG testing was evaluated in a twocenter study of 162 patients who were examined prior to the planned commencement of propranolol treatment for IH.13 In this study, 43 percent of patients who underwent routine ECG monitoring obtained abnormal results. This, in turn, led to 28 formal consultations with pediatric cardiologists, but none of those “abnormal” results were ultimately precluded from propranolol therapy. Moreover, no patient in this study experienced any adverse effects from propranolol therapy that could have been predicted by an ECG. Thus, the role of ECG monitoring in this context remains unclear, but this evidence suggests that ECG testing may not be necessary.14 For patients with bradycardia or a history of arrhythmias, features of posterior fossa brain malformations (PHACE syndrome), familial history of early cardiac death or congenital heart disease, or maternal history of connective tissue disease, an ECG may still be helpful and appropriate. Thus, the potential benefits of an ECG should be weighed against its cost and potential utility. PORT WINE STAINS AND STURGEWEBER SYNDROME It has long been thought that the JCAD distribution of port wine stains (PWS) follows the trigeminal nerve, but new evidence has found a relation to genetic mosaicism.15 PWS on the face, which appear to follow the embryonic vasculature (rather than the trigeminal nerve), may be an isolated finding or may occur along with Sturge-Weber Syndrome (SWS). Today, it is more useful to consider embryologic segments when discussing PWS rather than the older V1, V2, V3 criteria. SWS may be diagnosed when the patient presents with malformations of the cerebral and ocular vascular systems along with facial PWS. In a study of 192 children with facial PWS, two predictors of adverse outcomes emerged: a PWS involving any part of the forehead (defined by the line joining the outer canthus of the eye to the top of the ear, including the upper eyelid) and an abnormal magnetic resonance imaging (MRI) scan. Thus, it may be important for pediatric patients presenting with PWS on the forehead to undergo an ophthalmology review and a brain MRI.16 PWS and SWS are thought to be somatic mosaic mutations that disrupt vascular development. It has been theorized that the development time at which these mutations occur defines the severity and extent of PWS and SWS. In a study of wholegenome sequencing of DNA, a nonsynonymous single-nucleotide variant in GNAQ was identified in affected tissue samples of 88 percent of participants with SWS and 92 percent of patients with non-SWS PWS, but not in any of the affected tissue of others with unrelated cerebrovascular malformations or control patients. The mutant allele was prevalent in affected tissue at rates of 1.0 to 18.1 percent.17 In a study of 192 pediatric patients with facial PWS, adverse outcomes (defined as seizures, abnormalities in neurodevelopment, glaucoma, and abnormal MRI scans) were calculated. Based on the Fisher’s exact p-value, patients with forehead plaques were significantly more likely to have seizures, abnormal neurodevelopment, and glaucoma (p<0.001 for all) and an abnormal MRI (p=0.002) than patients with PWS without forehead involvement.16 A flowchart based on these experiences is presented in Figure 1. Thus, PWS on the forehead represent the highest risk for SWS, and MRI scans are the test of choice. NOVEL TOPICAL THERAPY FOR PORT WINE STAINS The preferred treatment for PWS remains pulsed dye laser (PDL), although it is thought that as much as 90 percent of PWS are refractory to PDL. This therapeutic resistance is attributed to revascularization post-laser-therapy. Oral sirolimus has been used with some success as adjunctive therapy to help reduce the possibility of revascularization, but it is associated with considerable side effects. A case report in the literature described a 56-year-old man with extensive PWS who was treated with PDL and topical sirolimus (rapamycin) 0.5% ointment. Significant improvement occurred JOURNAL OF CLINICAL AND AESTHETIC DERMATOLOGY March 2017 • Vol. 10 • No. 3 • Supplement 1 S9 REviEw Figure 1. Great Ormond Street Hospital management guidelines for children with facial port wine stains (PwS) on the forehead.16 MRi, magnetic resonance imaging with the combination therapy.18 In a phase II, randomized, double-blind, intra-individual, placebo-controlled trial (N=23) of patients with SWS and facial PWS, patients were randomized into four study arms: placebo, PDL + placebo, sirolimus (rapamycin), and PDL + sirolimus (rapamycin). The best result, defined as lowest digital photographic image score and lowest percentage of vessels in histologic analysis, was significantly better for patients in the PDL + sirolimus group.19 It is thought that topical sirolimus (rapamycin) suppresses the regeneration and revascularization of photo-coagulated blood vessels produced by PDL.20 Topical sirolimus (rapamycin) has been used to treat angiofibromas as well.21–23 It is available in 1% or 0.5% cream S10 JCAD and represents a promising new adjunctive treatment. While acne is ubiquitous in the industrialized world, affecting 79 to 95 percent of American adolescents, epidemiological studies suggest that acne rates are very low or nonexistent in some nonwestern societies, such as the Kitavan Islanders of Papua, New Guinea, and the Aché hunter-gathering society of Paraguay, where no cases of acne have been observed.24 These stark differences in the incidence of acne cannot be entirely explained by genetic differences; it is likely that environmental factors, including diet, play a role. Recent evidence suggests that diet affects the proliferation of basal keratinocytes ACNE AND DAIRY INTAKE within the pilosebaceous duct, androgen-mediated sebum production, colonization of the comedo by Propionibacterium acnes, and inflammation in and near the comedo.25 Some evidence has suggested the relationship between diet and acne involved the dietary glycemic load.26,27 More recent studies suggest that dairy products, specifically low-fat dairy products, may induce acne.28 In a case-control study (N=225), young people between the ages of 14 and 19 years with moderate to no acne (based on the Global Acne Assessment Scale) were interviewed three times for dietary recall using the Nutrition Data System for Research software.28 Participants with acne consumed significantly more low-fat milk and skim milk than those without acne (p=0.01), but the study found no difference in total dietary intake, saturated fat or trans-fat intake, or glycemic load. The study did not find any significant differences in total energy intake or body mass index (BMI) with respect to acne. Thus, in this study, full-fat milk was not associated with acne, but low-fat milk and skim milk were. However, in a case-control study of 88 patients aged 18 to 30 years with and without acne, interviews found that patients with acne had a significantly greater dietary glycemic load (175±35 vs. 122±28, p<0.001) and significantly greater consumption of milk and ice cream (p<0.01).29 The intake of refined sugar products has also been associated with acne.30 By contrast, a longitudinal survey-based study of students JOURNAL OF CLINICAL AND AESTHETIC DERMATOLOGY March 2017 • Vol. 10 • No. 3 • Supplement 1 REviEw between the ages of 15 and 19 conducted in Norway found that severe acne had a prevalence rate of about 13.9 percent in this population, and consumption of two or more glasses of full-fat dairy milk per day was associated with moderate-to-severe acne, but there was no association between the consumption of low-fat or skim milk products and acne.31 Thus, the evidence in the literature about dietary links to acne remains equivocal and warrants further study. ATOPIC DERMATITITS, ALLERGIES, AND THE EARLY INTRODUCTION OF PEANUTS Prior to 2008, experts recommended that peanut introduction be delayed in infants at high risk for allergies, although observational studies have suggested that complementary food introduction of high-risk allergens may offer a protective effect. The Learning Early About Peanut Allergy (LEAP) study consolidated this evidence and found that early introduction may indeed be beneficial.32–34 A recent study randomized 640 infants with severe eczema and/or egg allergy to either consume or avoid peanuts until five years of age. In the peanutavoidance group, the prevalence of peanut allergy at 60 months was 13.7 percent, while in the peanutconsumption group, the prevalence was 1.9 percent at five years (p<0.001).35 Thus, early introduction of peanuts into the diet of high-risk children was associated with decreased frequency of peanut JCAD allergy development. Thus, for infants with early-onset atopic disease (allergies), early peanut introduction may be beneficial. Skin testing or in-clinic observation of peanut ingestion is recommended because of the sometimes severe nature of such allergic reactions. An initial consultation with an allergist may be appropriate. Peanut introduction may then be carried on at home once the clinician can determine that the patient is not clinically reactive. Disordered sleeping and sleep deficits occur in children with atopic dermatitis and may cause a lower quality of life and negatively impact the child’s neurocognitive development.36 While the discomfort of dermatitis, itching, and scratching in the night may contribute to poor sleep in these children, it is likely that the cause of their sleep problems is more complex. In a randomized, double-blind, placebo-controlled, crossover study of 73 pediatric patients (aged 1–18 years) with atopic dermatitis over at least five percent of the body surface area, patients were treated with either melatonin 3mg/day or placebo for four weeks, followed by a two-week washout period, and then a crossover four-week study.37 Children were evaluated using the Scoring Atopic Dermatitis (SCORAD) index and were also evaluated for sleep-onset latency. SCORAD indices decreased by 9.1 versus placebo from a mean 49.1±24.3 to 40.2±20.9. Sleep-onset latency decreased 21.4 minutes after melatonin treatment compared to placebo (p=0.02). No adverse events were reported during the course of the study, and no patients withdrew from the study because of adverse events. Clinicians treating children with atopic dermatitis should ask them or their parents about their sleep hygiene. Looking ahead in atopic dermatitis, a new topical PDE4inhibitor currently in Phase III trials, crisaborole ointment, may be on the horizon.38 Systemic agents in the pipeline include dupilumab, a human monoclonal antibody against IL-4 (SQ),39,40 and apremilast, an oral PDE4-inhibitor.41 JANUS-KINASE INHIBITORS FOR ALOPECIA AREATA Alopecia areata is an autoimmune disease with strong associations to the genetic loci near immunefunction genes. In murine studies and early human studies, Januskinase (JAK) inhibitors interrupted these immune signaling pathways.42 Two new JAK inhibitors considered for use in alopecia areata in adults are tofacitinib and ruxolitinib.43,44 However, the safety of these drugs for use in pediatric patients remains undetermined. A case report showed the successful treatment of alopecia universalis with topical ruxolitinib (a topical JAK inhibitor).44 In a literature review, oral tofacitinib was found to be effective in the treatment of alopecia areata as well as other conditions, including psoriasis and vitiligo.43 This early evidence suggests that JAK inhibitors may offer an alternative therapeutic option for alopecia areata, and though they should be avoided as first-line therapy, may be considered in JOURNAL OF CLINICAL AND AESTHETIC DERMATOLOGY March 2017 • Vol. 10 • No. 3 • Supplement 1 S11 REviEw limited cases. There is no data on the long term safety of this medication in children..45 Topical JAK inhibitors may also be an appropriate prescribing choice. There is considerable interest at this time in finding a safe, effective, and convenient treatment for alopecia. CONGENITAL LANGERHANS CELL HISTIOCYTOSIS Congenital Langerhans cell histiocytosis (LCH) is a clonal disorder of the histiocytes, which are cells derived from the bone marrow. Morphologically, LCH appears to be a benign proliferation of inflammatory cells that somehow have evaded the body’s regulatory mechanisms, but our current understanding is that there is clonal proliferation of immune-processing cells (Langerhans cells), which suggests a malignant pathology.46 LCH manifests itself most commonly as a solitary lesion on the orbital bone of the eye, and can be treated with minimally invasive procedures. Recent studies have suggested that LCH may be a risk marker for central nervous system (CNS) disorders.46 While LCH may be systemic, it often affects only the skin. LCH most commonly presents in pediatric patients who exhibit infiltration of mast cells and Langerhans cells.47 LCH has four known variants: congenital self-healing reticulohistiocytosis (CSHRH, also called Hashimoto-Pritzker disease), Letterer-Siwe disease, HandSchüller-Christian disease, and eosinophilic granuloma.48 CSHRH appears to be a misnomer, because S12 JCAD not all cases resolve spontaneously.49 Infants with CSHRH have a mortality risk of three percent and a 10-percent chance of relapse.49 Infantile LCH may occur in the skin folds. Diagnosing CSHRH requires that the physician first rule out infection and then conduct a physical examination and a biopsy with a complete blood count, a comprehensive metabolic panel, urine assay, prothrombin time/partial thromboplastin time test, a chest Xray, and skeletal history. Timely diagnosis and prompt treatment with systemic agents are important. An oncology consultation may be of value. Kawasaki disease (KD) is a type of medium vessel vasculitis that typically presents in pediatric patients. Infantile KD may exhibit incomplete or atypical forms. Typical infant manifestations of KD include mucosal changes (64%), extremity changes (64%), rash (53%), conjunctival injection (47%), and cervical lymphadenopathy (17%). KD is associated with abnormalities in the coronary arteries. KD typically presents incompletely in infants younger than six months of age; KD should be suspected when a baby presents with unexplained fever extending beyond five days.50 Other types of pediatric vasculitis can be challenging to diagnose because their clinical manifestations, particularly in young children, can be highly variable. The size of the vessels involved, the organs involved, the extent of vascular MEDIUM VESSEL VASCULITIS injury, and underlying pathology all play a role in pediatric vasculitis.51 The signs of medium vessel vasculitis include fixed livedo, nodules, ulcers, and stellate purpura. To arrive at a differential diagnosis, the physician must consider granulomatosis with polyangiitis (previously Wegener’s granulomatosis), polyarteritis nodosa, various vasculopathies (for instance, antiphospholipid antibodies), and calciphylaxis. A blood panel should be ordered (complete blood count, complete metabolic panel, erythrocyte sedimentation rate/C-reactive protein, prothrombin time/partial thromboplastin time test, antiphospholipid antibodies, cryoglobulins, and QuantiFERONGold hepatitis panel).52 Imaging can be of great value.51 A skin biopsy and consultation with a dermatologist or rheumatologist may be warranted. These conditions carry a high morbidity and mortality burden and are characterized by frequent relapse.52 PEDIATRIC DERMATOLOGY: MAINTENANCE AND HOME CARE Dermatology frequently involves strategies aimed at maintaining therapeutic results and thus relies to a great extent on home care and “tips.”Here the authors present several of the latest tips for clinicians and their patients. Perioral irritant dermatitis is a frequent cause for clinic visits. This distressing condition may be triggered by excessive drooling, pacifiers, and the use of wet wipes. Parents of children suffering from JOURNAL OF CLINICAL AND AESTHETIC DERMATOLOGY March 2017 • Vol. 10 • No. 3 • Supplement 1 REviEw perioral irritant dermatitis should avoid putting socks on the hands of these children during sleep and discourage sucking on blankets or other items. This encourages saliva production and, in turn, irritation. Before the child eats or goes to sleep, a thick barrier-type ointment should be applied to the cheeks and chin. While phototherapy and systemic agents such as methotrexate, azathioprine, and mycophenolate may be helpful for children with atopic dermatitis, families can institute many practices at home to reduce atopic dermatitis. A diagnosis of atopic dermatitis should, in and of itself, mandate the exclusion of certain common household products: scented detergents, most shampoos, and many so-called “baby” products such as soaps and lotions. Parents should be advised that many seemingly benign products with labels promoting “natural” or “organic” soaps, cleansers, and lotions may be particularly irritating to children with atopic dermatitis due to botanical ingredients. While atopic dermatitis may be treated with topical steroids and calcineurin inhibitors, parents may also find it helpful to administer to their children probiotics or synbiotics every day, to apply coconut oil or shea butter to the skin, and to establish a routine for after-bath moisturizing. Bleach baths can be helpful to stop bacterial infections. Diaper rash is a common complaint and can be treated with a paste, such as Triple Paste®, with every diaper change. Hydrocortisone ointment 2.5% twice a day can JCAD further help treat this uncomfortable condition. In some cases, diaper dermatitis may actually be an allergic reaction to blue dye (“bluedye diaper dermatitis”). In the event that the response is to blue dye, the parents should switch to dye-free diapers (Huggies Natural, 7th Generation, Earth’s Best) and treat the rash with a mid-potency topical steroid ointment. If that ointment is not entirely effective, mupirocin ointment can be added at signs of infection. Likewise, dermatologists may see cases of “car seat dermatitis.” This occurs when the child is irritated by or allergic to the linings of certain car seats. An easy way to manage this condition is to add a cotton cover or some other cover to the car seat so that there is no direct contact between the child’s skin and the liner. Pediatric dermatology is a relatively new subspecialty in medicine, although cutaneous complaints in pediatric patients are extremely common. New breakthroughs in the treatments of hemangiomas, PWS, SWS, and medium vessel vasculitis offer hope for these conditions, which have not responded well to conventional therapies. Topical sirolimus ointment may be a helpful adjunct to PDL therapy for treating PWS. Better understanding of congenital LCH may improve its management outcomes and follow-up. New drugs such as JAK inhibitors may offer broader therapeutic choices for alopecia. Long-standing issues such CONCLUSION as the relationship of diet to acne and the early introduction of allergens to high-risk patients have re-emerged with more data to help guide treatment. Finally, pediatric dermatology requires maintenance efforts, and parents should be counseled on things that they can do at home to help these conditions in their children. 1. Hurwitz S. The history of pediatric dermatology in the United States. Pediatr Dermatol. 1988;5(4):280– 285. Tunnessen WW Jr. A survey of skin disorders seen in pediatric general and dermatology clinics. Pediatr Dermatol. 1984;1(3):219– 222. Hayden GF. Skin diseases encountered in a pediatric clinic. A one-year prospective study. Am J Dis Child. 1985;139(1):36–38. Krowchuk DP, Bradham DD, Fleischer AB Jr. Dermatologic services provided to children and adolescents in primary care and other physicians in the United States. Pediatr Dermatol. 1994;11(3):199–203. Prindaville B, Antaya RJ, Siegfriend EC. Pediatric dermatology: past, present, and future. Pediatr Dermatol. 2015;32(1):1–12. Leaute-Labreze C, Harper JI, Hoeger PH. Infantile haemangioma. Lancet. 2017 Jan 12. Chang EI, Chang EI, Thangarajah H, Hamou C, Gurtner GC. Hypoxia, hormones, and endothelial progenitor cells in hemangioma. Lymphat Res Biol. REFERENCES 2. 3. 4. 5. 6. 7. JOURNAL OF CLINICAL AND AESTHETIC DERMATOLOGY March 2017 • Vol. 10 • No. 3 • Supplement 1 S13 REviEw 8. 9. 10. 11. 12. 13. 14. S14 2007;5(4):237–243. Yu L, Li S, Su B, et al. Treatment of superficial infantile hemangiomas with timolol: evaluation of short-term efficacy and safety in infants. Exp Ther Med. 2013;6(2):388–390. Sendrasoa FA, Ranaivo IM, Razanakoto NH, Andrianarison M, Ramarozatovo LS, Rapelanoro Rabenja F. Excellent response of infantile orbital hemangioma to propranolol. Int Med Case Rep J. 2016;9:369–371. Varrasso G, Schiavetti A, Lanciotti S, et al. Propranolol as first line treatment for life-threatening diffuse infantile hepatic hemangioma: a case report. Hepatology. 2017 Jan 5. Leaute-Labreze C, Boccara O, Degrugillier-Chopinet C, et al. Safety of oral propranolol for the treatment of infantile hemangioma: a systematic review. Pediatrics. 2016;138(4). Parikh SR, Darrow DH, Grimmer JF, Manning SC, Richter GT, Perkins JA. Propranolol use for infantile hemangiomas: American Society of Pediatric Otolaryngology Vascular Anomalies Task Force practice patterns. JAMA Otolaryngol Head Neck Surg. 2013;139(2):153–156. Yarbrough KB, Tollefson MM, Krol AL, Leitenberger SL, Mann JA, MacArthur CJ. Is routine electrocardiography necessary before initiation of propranolol for treatment of infantile hemangiomas? Pediatr Dermatol. 2016;33(6):615–620. Streicher JL, Riley EB, CasteloSoccio LA. Reevaluating the need JCAD 15. 16. 17. 18. 19. 20. for electrocardiograms prior to initiation of treatment with propranolol for infantile hemangiomas. JAMA Pediatr. 2016;170(9):906–907. Dutkiewicz AS, Ezzedine K, Mazereeuw-Hautier J, et al. A prospective study of risk for Sturge-Weber syndrome in children with upper facial portwine stain. J Am Acad Dermatol. 2015;72(3):473–480. Waelchli R, Aylett SE, Robinson K, Chong WK, Martinez AE, Kinsler VA. New vascular classification of port-wine stains: improving prediction of SturgeWeber risk. Br J Dermatol. 2014;171(4):861–867. Shirley MD, Tang H, Gallione CJ, et al. Sturge-Weber syndrome and port-wine stains caused by somatic mutation in GNAQ. N Engl J Med. 2013;368(21):1971–1979. Griffin TD Jr, Foshee JP, Finney R, Saedi N. Port wine stain treated with a combination of pulsed dye laser and topical rapamycin ointment. Lasers Surg Med. 2016;48(2):193–196. Marques L, Nunez-Cordoba JM, Aguado L, et al. Topical rapamycin combined with pulsed dye laser in the treatment of capillary vascular malformations in Sturge-Weber syndrome: phase II, randomized, double-blind, intraindividual placebo-controlled clinical trial. J Am Acad Dermatol. 2015;72(1):151–158.e151. Gao L, Phan S, Nadora DM, et al. Topical rapamycin systematically suppresses the early stages of pulsed dye laser-induced angiogenesis pathways. Lasers 21. 22. 23. 24. 25. 26. 27. 28. Surg Med. 2014;46(9):679–688. Cinar SL, Kartal D, Bayram AK, et al. Topical sirolimus for the treatment of angiofibromas in tuberous sclerosis. Indian J Dermatol Venereol Leprol. 2017;83(1):27–32. Balestri R, Neri I, Patrizi A, Angileri L, Ricci L, Magnano M. Analysis of current data on the use of topical rapamycin in the treatment of facial angiofibromas in tuberous sclerosis complex. J Eur Acad Dermatol Venereol. 2015;29(1):14–20. Park J, Yun SK, Cho YS, Song KH, Kim HU. Treatment of angiofibromas in tuberous sclerosis complex: the effect of topical rapamycin and concomitant laser therapy. Dermatology. 2014;228(1):37–41. Cordain L, Lindeberg S, Hurtado M, Hill K, Eaton SB, Brand-Miller J. Acne vulgaris: a disease of Western civilization. Arch Dermatol. 2002;138(12):1584– 1590. Cordain L. Implications for the role of diet in acne. Semin Cutan Med Surg. 2005;24(2):84–91. Burris J, Rietkerk W, Woolf K. Acne: the role of medical nutrition therapy. J Acad Nutr Diet. 2013;113(3):416–430. Smith RN, Mann NJ, Braue A, Makelainen H, Varigos GA. A lowglycemic-load diet improves symptoms in acne vulgaris patients: a randomized controlled trial. Am J Clin Nutr. 2007;86(1):107–115. LaRosa CL, Quach KA, Koons K, et al. Consumption of dairy in teenagers with and without acne. J JOURNAL OF CLINICAL AND AESTHETIC DERMATOLOGY March 2017 • Vol. 10 • No. 3 • Supplement 1 REviEw 29. 30. 31. 32. 33. 34. 35. 36. Am Acad Dermatol. 2016;75(2):318–322. Ismail NH, Manaf ZA, Azizan NZ. High glycemic load diet, milk and ice cream consumption are related to acne vulgaris in Malaysian young adults: a case control study. BMC Dermatol. 2012;12:13. Veith WB, Silverberg NB. The association of acne vulgaris with diet. Cutis. 2011;88(2):84–91. Ulvestad M, Bjertness E, Dalgard F, Halvorsen JA. Acne and dairy products in adolescence: results from a Norwegian longitudinal study. J Eur Acad Dermatol Venereol. 2016 Jul 16. Symon B, Crichton G. Urgent information on peanut allergy: New evidence from the LEAP study. Aust Fam Physician. 2015;44(9):618. Greenhawt M. The Learning Early About Peanut Allergy study: the benefits of early peanut introduction, and a new horizon in fighting the food allergy epidemic. Pediatr Clin North Am. 2015;62(6):1509–1521. Fleischer DM, Sicherer S, Greenhawt M, et al. Consensus communication on early peanut introduction and the prevention of peanut allergy in high-risk infants. Pediatrics. 2015 Aug 31. Du Toit G, Roberts G, Sayre PH, et al. Randomized trial of peanut consumption in infants at risk for peanut allergy. N Engl J Med. 2015;372(9):803–813. Chang YS, Lin MH, Lee JH, et al. Melatonin supplementation for children with atopic dermatitis and sleep disturbance: a randomized clinical trial. JAMA Pediatr. JCAD 37. 38. 39. 40. 41. 42. 43. 44. 2016;170(1):35–42. Chang YS, Chiang BL. Mechanism of sleep disturbance in children with atopic dermatitis and the role of the circadian rhythm and melatonin. Int J Mol Sci. 2016;17(4):462. Paller AS, Tom WL, Lebwohl MG, et al. Efficacy and safety of crisaborole ointment, a novel, nonsteroidal phosphodiesterase 4 (PDE4) inhibitor for the topical treatment of atopic dermatitis (AD) in children and adults. J Am Acad Dermatol. 2016;75(3):494– 503.e494. Simpson EL, Bieber T, GuttmanYassky E, et al. Two phase 3 trials of dupilumab versus placebo in atopic dermatitis. N Engl J Med. 2016;375(24):2335–2348. Lauffer F, Ring J. Target-oriented therapy: emerging drugs for atopic dermatitis. Expert Opin Emerg Drugs. 2016;21(1):81–89. Saporito RC, Cohen DJ. Apremilast use for moderate-tosevere atopic dermatitis in pediatric patients. Case Rep Dermatol. 2016;8(2):179–184. Samadi A, Ahmad Nasrollahi S, Hashemi A, Nassiri Kashani M, Firooz A. Janus kinase (JAK) inhibitors for the treatment of skin and hair disorders: a review of literature. J Dermatolog Treat. 2017 Jan 22:1–11. Kostovic K, Gulin SJ, Mokos ZB, Ceovic R. Tofacitinib, an oral Janus kinase inhibitor: perspectives in dermatology. Curr Medi Chem. 2017 Jan 12. Craiglow BG, Tavares D, King BA. Topical ruxolitinib for the treatment of alopecia universalis. 45. 46. 47. 48. 49. 50. 51. 52. JAMA Dermatol. 2016;152(4):490–491. Kennedy Crispin M, Ko JM, Craiglow BG, et al. Safety and efficacy of the JAK inhibitor tofacitinib citrate in patients with alopecia areata. JCI Insight. 2016;1(15):e89776. Margo CE, Goldman DR. Langerhans cell histiocytosis. Surv Ophthalmol. 2008;53(4):332–358. Lozano Masdemont B, Campos Dominguez M, Gomez-Recuero Munoz L, et al. Congenital cutaneous Langerhans cell histiocytosis and cutaneous mastocytoma in a child. Dermatol Online J. 2016;22(4). Kassardjian M, Patel M, Shitabata P, Horowitz D. Congenital selfhealing reticulohistiocytosis: an underreported entity. Cutis. 2016;97(4):296–300. Larsen L, Merin MR, Konia T, Armstrong AW. Congenital selfhealing reticulohistiocytosis: concern for a poor prognosis. Dermatol Online J. 2012;18(10):2. Singh S, Agarwal S, Bhattad S, et al. Kawasaki disease in infants below 6 months: a clinical conundrum? Int J Rheum Dis. 2016;19(9):924–928. Khanna G, Sargar K, Baszis KW. Pediatric vasculitis: recognizing multisystemic manifestations at body imaging. Radiographics. 2015;35(3):849–865. Sacri AS, Chambaraud T, Ranchin B, et al. Clinical characteristics and outcomes of childhood-onset ANCA-associated vasculitis: a French nationwide study. Nephrol Dial Transplant. 2015;30 Suppl 1:i104–112. JOURNAL OF CLINICAL AND AESTHETIC DERMATOLOGY March 2017 • Vol. 10 • No. 3 • Supplement 1 S15