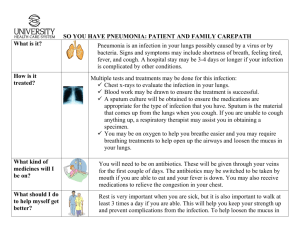
Laboratory Result November 26, 2009 Parameters Result Normal values Clinical significance hemoglobin hematocrit RBC White cell count 139. 5 0.44 4.73 19.3 (15.8) 138-166g/l 0.40-0.48g/l 4.2-6.5m/U 5-10x10g/l normal Normal Normal infection Differential Count basophils segmenters Lymphocytes Monocytes 0.01 0.36(.24) .62(.56) .01 0 - 0.5 .55 - .65 .2 -.6 .2 - .6 normal Platelets count 277 (133) 150-350x10g/l MVP RDW MCV MCHC 7.17 11.52 89.81 32.82 5.83-8.46f/L 11.0-14.0 f/L 80.97f/L 32-36% Aplastic or aplastic bone marrow, leukemia, vit. B12 deficiency immiiiiune disorder. normal normal Normal normal normal normal Microscopic / Chemical Examinations Routine Physical Examination Color: straw Turbidity: clear CHEMICAL ANAYSIS glucose Bilirubin Ketone Specifis gravity bood negative Negative Negative 1.015 negative Ph:8.5 Protein: negative Urobilirubin: normal Nitrite: negative Leukocytes: negative Introduction Pneumonia is acute inflammation of the lungs caused by infection. Initial diagnosis is usually based on chest x-ray. Causes, symptoms, treatment, preventive measures, and prognosis differ depending on whether the infection is bacterial, viral, fungal, or parasitic; whether it is acquired in the community, hospital, or nursing home; and whether it develops in a patient who is immunocompetent or immunocompromised. An estimated 2 to 3 million people in the US develop pneumonia each year, of whom about 45,000 die. Pneumonia is the most common fatal hospital-acquired infection and the most common overall cause of death in developing countries. Bacteria are the most common cause of pneumonia in adults > 30 yr, Streptococcus pneumoniae infection being the most common pathogen across all age groups, settings, and geographic regions. However, pathogens of every sort, from viruses to parasites, cause pneumonia. The airways and lungs are constantly exposed to pathogens in the external environment; the upper airways and oropharynx in particular are colonized with so-called normal flora rendered harmless by host defenses. Infection develops when pathogens that are inhaled or aspirated or reach the lungs via the bloodstream or contiguous spread overcome multiple host defenses. Upper airway defenses include salivary IgA, proteases, and lysozymes; growth inhibitors produced by normal flora; and fibronectin, which coats the mucosa and inhibits adherence. Nonspecific lower airway defenses include cough, mucociliary clearance, and airway angulation preventing infection in airspaces. Specific lower airway defenses include various pathogen-specific immune mechanisms, including IgA and IgG opsonization, anti-inflammatory effects of surfactant, phagocytosis by alveolar macrophages, and T-cell–mediated immune responses. These mechanisms protect most people against infection. But numerous conditions alter normal flora (eg, systemic illness, undernutrition, hospital or nursing home exposure, antibiotic exposure) or impair these defenses (eg, cigarette smoking, nasogastric or endotracheal intubation). Pathogens that then reach airspaces can multiply and cause pneumonia. Specific pathogens causing pneumonia cannot be found in < 50% of patients, even with extensive diagnostic investigation. But because pathogens and outcomes tend to be similar by setting and host risk factors, pneumonias can be categorized as Anatomy and Physiology The main function of the lungs is to provide continuous gas exchange between inspired air and the blood in the pulmonary circulation, supplying oxygen and removing carbon dioxide, which is then cleared from the lungs by subsequent expiration. Survival is dependent upon this process being reliable, sustained and efficient, even when challenged by disease or an unfavourable environment. Evolutionary development has produced many complex mechanisms to achieve this, several of which are compromised by anaesthesia. A good understanding of respiratory physiology is therefore essential to ensure patient safety during anaesthesia. Anatomy The respiratory tract extends from the mouth and nose to the alveoli. The upper airway serves to filter airborne particles, humidify and warm the inspired gases. The patency of the airway in the nose and oral cavity is largely maintained by the bony skeleton, but in the pharynx is dependent upon the tone in the muscles of the tongue, soft palate and pharyngeal walls. Larynx The larynx lies at the level of upper cervical vertebrae, C4-6, and its main structural components are the thyroid and cricoid cartilages, along with the smaller arytenoid cartilages and the epiglottis, which sit over the laryngeal inlet. A series of ligaments and muscles link these structures, which, by a co-ordinated sequence of actions, protect the larynx from solid or liquid material during swallowing as well as regulating vocal cord tension for phonation (speaking). The technique of cricoid pressure is based on the fact that the cricoid cartilage is a complete ring, which is used to compress the oesophagus behind it against the vertebral bodies of C5-6 to prevent regurgitation of gastric contents into the pharynx. The thyroid and cricoid cartilages are linked anteriorly by the cricothyroid membrane, through which access to the airway can be gained in an emergency. Trachea and bronchi The trachea extends from below the cricoid cartilage to the carina, the point where the trachea divides into the left and right main bronchus, with a length of 12-15cm in an adult and an internal diameter of 1.5-2.0cm. The carina lies at the level of T5 (5th thoracic vertebra) at expiration and T6 in inspiration. Most of its circumference is made up of a series of C-shaped cartilages, but the trachealis muscle, which runs vertically, forms the posterior aspect. When the trachea bifurcates, the right main bronchus is less sharply angled from the trachea than the left, making aspirated material more likely to enter the right lung. In addition, the right upper lobe bronchus arises only about 2.5cm from the carina and must be accommodated when designing right-sided endobronchial tubes. Lungs and pleura The right lung is divided into 3 lobes (upper, middle and lower) whereas the left has only 2 (upper and lower), with further division into the broncho-pulmonary segments (10 right, 9 left). In total there are up to 23 airway divisions between trachea and alveoli. The bronchial walls contain smooth muscle and elastic tissue as well as cartilage in the larger airways. Gas movement occurs by tidal flow in the large airways. In the small airways, by contrast, (division 17 and smaller) it results from diffusion only. The pleura is a double layer surrounding the lungs, the visceral pleura enveloping the lung itself and the parietal pleura lining the thoracic cavity. Under normal circumstances the interpleural space between these layers contains only a tiny amount of lubricating fluid. The pleura and lungs extend from just above the clavicle down to the 8th rib anteriorly, the 10th rib laterally and the level of T12 posteriorly. The lungs have a double blood supply, the pulmonary circulation for gas exchange with the alveoli and the bronchial circulation to supply the parenchyma (tissue) of the lung itself. Most of the blood from the bronchial circulation drains into the left side of the heart via the pulmonary veins and this deoxygenated blood makes up part of the normal physiological shunt present in the body. The other component of physiological shunt is from the thebesian veins, which drain some coronary blood directly into the chambers of the heart. The pulmonary circulation is a low-pressure (25/10mmHg), low-resistance system with a capacity to accommodate a substantial increase in blood flowing through it without a major increase in pressure. Vascular distension and recruitment of unperfused capillaries achieve this. The main stimulus which produces a marked increase in pulmonary vascular resistance is hypoxia. Objectives General Objectives: To provide the students a guide line caring for persons with pneumonia using the nursing process. To give information on the readers on the nature and extend of Pneumonia. Lastly, to provide a general public of the new developments in nursing care with regards to treating Pneumonia. Specific Objectives: At the end of this study, the student will able to: Define and identify the probable causative factors of pneumonia trace the anatomy and physiology Assess the nursing history of the patient. Identify the signs and symptoms of pneumonia. Formulate the nursing care plan, to achieve the maximum wellness of the patient as well as awareness on the part of the significant others. 6. to provide health teaching to the patient and significant others to improved the former condition and prevent complication. 1. 2. 3. 4. 5. Nursing History Biographic Data Baby John Timothy Angeles is a 1 month old, a Roman Catholic, residing at Sta. Cruz Manila, His birth Day is on October 13, 2009. He was admitted on November 18, 2009 at 9 am. Chief Complaint: DOB and Cough History of Present illness Two days prior to admission, patient’s mother noticed that john had a fever and cough. Patient showed lack to interest or decrease drink of milk. One day prior to admission, the patient fever and frequent cough, the fever is on and off in the morning and evening. Four hours prior to admission, the patient consulted a pediatrician. He was advised to take erythromycin, salbutamol and piperacilin. Two hours prior to admission, the patient complains DOB to her mother hence patient rushed to PCMC and subsequently admitted. PAST MEDICAL HISTORY Allergies: non No previous hospitalization Immunization: BCG, DPT, hepa B. SOCIO CULTURAL The patient lived with her parents in a medium size of house in bambang Manila. He is the only child; her father is a construction worker, and have own a mini grocery. She take a regular nap in the morning and evening. Gen. Name Band Name salbutamol albuterol Classification Dosage Mechanism of Action Indications Contraindications Side Effects Nursing Implication 8 mg Stimulates beta-2 receptors of bronchioles by increasing level of cAMP which relaxes smooth muscle to produce bronchodilati ns. Also cause CNS stimulation, increase diuresis, skeletal muscle tremors, and increase gastric acid secretion. Longer acting than isoprotenerol relief of bronchospasm in bronchial asthma, chronic bronchitis, emphysema and other reversible, obstructive pulmonary diseases. Also useful for treating bronchospasm in patient with co-existing heart disease of hypertension. Hypersensitivity to salbutamol, also to artropine and its derivatives. Threatened absorption during the 1st and 2nd trimester. Cardiac arrhythmia associated with tachycardia cause by digitalis intoxication. Hypertrophic obstructive cardiomyopathy or tachyarrthmia. Thyrotoxicosis. Prevention of premature labor associated with toxemia of pregnancy or antepartum hemorrhage. Lactation. Use with non selective beta-blockers. Fine skeletal muscle tremor, leg cramps, palpitati on, tachycar dia, hyperten tion, head ache, nausea, vomitin g, dizzines s, hyper activity, insomia, hypoten sion, mouth and throat irritation . -Assess the cardiorespiratory function, BP, heart rate, rhythm and breathe sound. -determine history of previous medication. -monitor for evidence of allergic reaction. Gen. name Erythromyci n Brand Classificatio Name n Dosage Mechanism Indication Of action 100mg/5ml Treatment of infections of respiratory tract, skin and skin structures STD cause by susceptible organism treatment of pertussis, diphtheria, intestinal amebiasis conjunctiviti s of new bornand legionnaire disease. Evaluation Contraindication Side Effect Hypersensitivity to erythromycin or any macrolide antibiotic. Pre existing liver disease, epithelial herpes keratitis. Rash, photosensitivit y diarrhea, nausea. Vomiting, abdominal pain, and vaginitis. Nursing Implication -Assess the patient for previous sensitivity reaction. -Assess the patient for signs and symptoms of infection before and during treatment This case study was able to improve the knowledge of the student nurses by letting gain understanding of the nature of the disease and by letting they formulate appropriate nursing procedures to the client. Not with standing, through their study the student nurses were able to enhance their attitude and skills. The whole case study was also able to adequate information regarding the disease and may serve as a future comparison for the study related to the case.