Physiological effects of high and low barometric pressure Deranged Physiology
advertisement

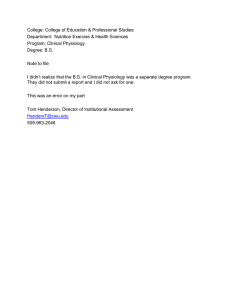
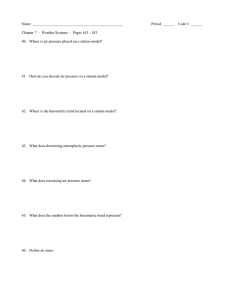
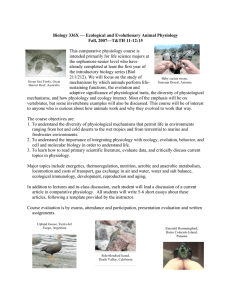
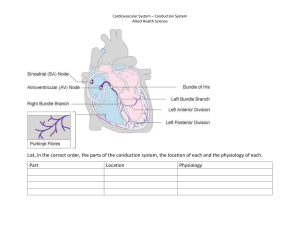
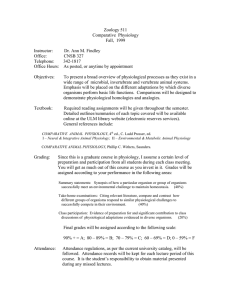
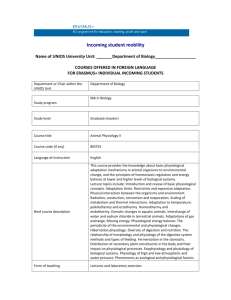
4/13/2021 Physiological effects of high and low barometric pressure | Deranged Physiology Deranged Physiology » CICM Primary Exam » Required Reading » Respiratory system Physiological effects of high and low barometric pressure is chapter is not relevant to any specific Section from the 2017 CICM Primary Syllabus, because there is no specific entry for "describe the physiology of being sucked out of an airlock". However, estion 10 from the second paper of 2009 specifically asked for "the respiratory physiological responses to altitude". e examiners also wanted a discussion of "the changes in inspired and alveolar oxygen partial pressure with increasing altitude", which allows for some fascinating digressions. So that the reader can avoid these, a brief exam-focused summary follows: With altitude: Barometric pressure decreases and is ~ 200 mmHg at 10,000m altitude Saturated vapour pressure remains stable at 37 ºC (47 mmHg) Alveolar PO2 decreases, and is ~ 30 mmHg at 8,000m altitude PaCO2 decreases due to hypoxic drive, and is ~ 10mmHg at 8,000m e physiological responses to altitude are: Acute: Respiratory: Minute volume increases due to hypoxic reaspiratory drive, mediated by peripheral chemoreceptors Cardiovacular: Tachycardia and increased cardiac output due to increased sympathetic drive ere is also a mild blood pressure increase Neurological: Decreased cognitive function With profound hypoxia, delirium can develop Renal and electrolyte: Diuresis Decreased serum bicarbonate (due to hypcapnia) Chronic: Respiratory: Minute volume remains the same Tidal volume may gradually increase due to thoracic remodelling Cardiovascular: Heart rate and stroke volume return to normal values as the haematocrit adapts Haematological: Haematocrit increases over days/weeks, largely due to haemopoiesis and haemoconcentration ough the term "altitude" of course implies "great height", barometric pressure is a continuum which spans in both directions from the impossibly narrow range of physiologically normal values. In this chapter, some effort will be spent to cover both the highs and the lows, as they are equally interesting. Some discussion of the more practical aspects of this is also discussed in a chapter concerning critical illness due to high altitude. A good single reference for adaptation to low barometric pressure is Martin & Windsor (2009), which would be enough for anybody preparing for CICM exams. https://derangedphysiology.com/main/cicm-primary-exam/required-reading/respiratory-system/Chapter 923/physiological-effects-high-and-low-barom… 1/16 4/13/2021 Physiological effects of high and low barometric pressure | Deranged Physiology Atmospheric and alveolar gas content at depth and altitude Atmospheric pressure drops with increasing altitude, such that at around 8000m altitude we encounter what is lovingly known as the "death zone" in mountaineering circles, where survival without supplemental oxygen is impossible. If one were to plug a progression of altitude values into a simple formula, a graph like this could be generated, which appears to agree with empirically measured values. What puts the "death" into "death zone" is, of course, the fall in the concentration of oxygen which occurs with decreasing barometric pressure. To borrow some data from Ortiz-Prado et al (2019), a handy chart can be generated to represent the thin 10km sliver of lowermost troposphere: https://derangedphysiology.com/main/cicm-primary-exam/required-reading/respiratory-system/Chapter 923/physiological-effects-high-and-low-barom… 2/16 4/13/2021 Physiological effects of high and low barometric pressure | Deranged Physiology e gas mixture at this lowish altitude remains relatively stable in its proportion of partial pressures. In other words, at an altitude of 10,000m where the atmospheric pressure is 200mmHg, oxygen still makes up 21% of the gas mixture, which gives it a partial pressure of 42 mmHg. For this reason, "high altitude" for purposes of medical discussion is defined at about 2,700m above sea level, where the partial pressure of oxygen is 60 mmHg, enough to bring about all those interesting physiological phenomena so beloved by CICM examiners. Beyond the relatively thin layer of troposphere, the composition of which is recognisable as a humanbreathable gas mixture, there is a huge diffuse layer which has a very different composition. Here is a graphic borrowed from mrreid.org which is based on the NASA MSIS-90 atmosphere model: As one can see, by the time we reach an altitude of 800-900 km, the dominant gases in the mixture are now helium and hydrogen. e physiological implications of breathing this sort of gas mixture will not be discussed here any further, as the barometric pressure at 100km is already 0.0008 mmHg, and therefore resembles interplanetary vacuum for the intents and purposes of respiratory physiology. Changes in alveolar gas composition with altitude With altitude, the temperature of the gas mixture also changes, plateauing at around -57 ºC from around 40,000m onwards. Fortunately, the human upper respiratory tract has excellent efficiency as a heater and humidifier, which means that even at such temperatures the gas mixture reaching the lungs would be heated to body temperature and maximally humidified. us, the saturated vapour pressure of water remains a constant 47 mmHg, at least until you hit the Armstrong limit. is is a problem, as the constant partial pressure of water vapour reduces the potential space for oxygen in the gas mixture. e other gas in the alveolar mixture is CO2, which fortunately does not stay at sea level values, mainly because hypoxia produces vigorous hyperventilation. Healthy young anaesthetists at the summit of Everest had PaCO2 values of around 10-15 mmHg as the result of this. So, what are the implications of this for alveolar oxygen? If one were to plot the results of the alveolar gas equation, estimating a relatively linear progression of CO2 decrease (down to a minimum of 10 mmHg) it would look like this: https://derangedphysiology.com/main/cicm-primary-exam/required-reading/respiratory-system/Chapter 923/physiological-effects-high-and-low-barom… 3/16 4/13/2021 Physiological effects of high and low barometric pressure | Deranged Physiology In summary, without supplemental oxygen, the alveolar oxygen content would be zero by about 15,000m altitude (at a total atmospheric pressure of around 86 mmHg). At the summit of Everest, the aforementioned splendid examples of courage were able to survive with a PaO2 of around 30 mmHg on average (an arterial pO2 of ~ 25 mmHg, giving peripheral sats in a range of 34-69%), mainly because they were fit, healthy, and preceded their ascent with a period of acclimatisation. Acute physiological responses to low barometric pressure At risk of trespassing out of respiratory territory and into cardiovascular, the following acute changes occur with a sudden exposure to hypobaric pressure: Respiratory changes: Increased resting minute ventilation due to hypoxic drive (via peripheral chemoreceptors), which is moderated by the response to hypocapnia from central chemoreceptors. Decreased PaCO2 which results from this increased ventilation; the drop can be quite substantial, as illustrated abundantly by the much-quoted example of the Everest mountaineers. Cardiovascular changes: Increased resting heart rate and cardiac output occurs almost immediately, and takes a few days to subside. Vogel & Harris (1967) locked a bunch of healthy young people in a hypobaric chamber and then made them pedal endlessly on cycle ergometers. ey found that total cardiac output increases substantially with increasing altitude: https://derangedphysiology.com/main/cicm-primary-exam/required-reading/respiratory-system/Chapter 923/physiological-effects-high-and-low-barom… 4/16 4/13/2021 Physiological effects of high and low barometric pressure | Deranged Physiology is all appears to be the consequence of increased sympathetic nervous system activity, and tends to return to near-normal levels the end of the first week. Increased blood pressure is modest, and occurs as the result of increased cardiac output; total peripheral resistance is actually decreased. Neurological changes: Decreased cognitive function and delirium are the consequences of acute hypobaric hypoxia. is is a well-known phenomenon, and with an abrupt exposure, it is only a maer of time. Specifically, that time is known as TUC, "Time of Useful Consciousness", the brief panic-filled period of scrambling for your oxygen mask as the cabin suddenly depressurises. Wikipedia produces this helpful table: Altitude TUC (normal ascent) TUC (rapid decompression) 5,500 m 20 to 30 minutes 10 to 15 minutes 6,700 m 10 minutes 5 minutes 7,600 m 3 to 5 minutes 1.5 to 3.5 minutes https://derangedphysiology.com/main/cicm-primary-exam/required-reading/respiratory-system/Chapter 923/physiological-effects-high-and-low-barom… 5/16 4/13/2021 Physiological effects of high and low barometric pressure | Deranged Physiology 8,550 m 2.5 to 3 minutes 1.25 to 1.5 minutes 9,150 m 1 to 2 minutes 30 to 60 seconds 10,650 m 30 secs to 1 minute 15 to 30 seconds 12,200 m 15 to 20 seconds 7 to 10 seconds 13,100 m 9 to 12 seconds 5 seconds 15,250 m 9 to 12 seconds 5 seconds Hall (1949), trying to investigate this, asked healthy subjects to perform simple tasks (eg. react to changing images by clicking a selector switch) Presumably, the period of useful consciousness is followed by a period of useless consciousness, during which the subject performs various disorganised tasks which do not appear to have his/her survival as the goal. Beyond that, coma ensues aer several seconds. As one's organ of remembering is the first to starve of oxygen, the descent into purposeless fidgeting oen goes unnoticed, and Hall reports that "most of the subjects disclaimed knowledge of loss of consciousness". Chronic adaptation to low barometric pressure Respiratory changes: Increased resting minute ventilation persists during one's stay at altitude Decreased PaCO2 which results from this increased ventilation; the drop can be quite substantial, as illustrated abundantly by the much-quoted example of the Everest mountaineers. Increased pulmonary arterial pressure and vascular density, which allows for improved pulmonary perfusion, is apparently mild: Naeije (2010) reports a mean PA pressure of only 25 mmHg. e total pulmonary diffusing capacity increases, partly due to increased alveolar surface area and partly due to an increase in pulmonary blood volume associated with larger tidal volumes. Oxygen carrying capacity of the blood changes: increased erythrocyte 2,3-DPG shis the oxygen dissociation curve to the right, facilitating the release of oxygen to the tissues. ere is also an increase in skeletal muscle vascularity and muscle tissue myoglobin Cardiovascular changes: Heart rate remains increased: Naeije (2010), quoting a study of adaptation to an altitude of 3800m, produces this trend of the first eight days: https://derangedphysiology.com/main/cicm-primary-exam/required-reading/respiratory-system/Chapter 923/physiological-effects-high-and-low-barom… 6/16 4/13/2021 Physiological effects of high and low barometric pressure | Deranged Physiology "This situation then remains stable over time", he says. Mountain natives all seem to have a higher resting heart rate as compared to lowlander controls, but the cardiac output in both groups is prey much the same. Increased blood pressure remains increased due to systemic vascular resistance from increased catecholamine secretion at any given workload, and due to increased blood viscosity resulting from increased haematocrit. Electrolyte changes: Serum bicarbonate decreases, which is a totally predictable consequence of chronic hypocapnia. Hannon et al (1971) marched nine healthy young soldiers up to Pikes Peak and found that on average, their serum HCO3- levels decreased by 7 mmol/L. Fluid balance and haematological changes: Haematocrit increases, in part due to a loss of extracellular water, and in part due to the erythropoiesis stimulated by hypoxia. is graph from Zubieta-Calleja et al (2007) demonstrates the sort of timeframe we are talking about: e plasma volume is reduced and the fluid balance is negative, when compared to preacclimatisation values. is "high-altitude diuresis" is thought to be the product of the net action https://derangedphysiology.com/main/cicm-primary-exam/required-reading/respiratory-system/Chapter 923/physiological-effects-high-and-low-barom… 7/16 4/13/2021 Physiological effects of high and low barometric pressure | Deranged Physiology of BNP, renin, aldosterone and decreased circulating levels of vasopressin (Goldfarb-Rumyantzev et al, 2014). Physiological consequences of explosive decompression Unfortunately, in some circumstances, there may be no time to undergo physiological adaptation in any meaningful sense, as hypobaric conditions may arrive suddenly. If this happens and you happen to have a ready supply of 100% oxygen, ongoing (unhappy) survival can be assured at minimum barometric pressures of around 190 mmHg, which corresponds to an altitude of about 10,000m. To go higher than that for any extended period of time would require the use of a pressurised suit. Harry Armstrong, aer whom the Armstrong Limit is named, described the upper limits of even shortterm survival as being around the territory of 18,000-19,000m above sea level, where the boiling point of body fluids is below the boiling point of water at that pressure (47 mmHg). e partial pressure of atmospheric oxygen at this altitude is so low that total anoxia should be assumed, and the conditions are assumed to be rapidly lethal. At this stage, and beyond, survival is unlikely unless urgent repressurisation takes place. As if anoxia were not enough, as pressure drops even more disturbing phenomena take place. For instance, as blood in arteries and veins is relatively pressurised in comparison to the external environment, it is not expected to boil at the Armstrong limit, but in complete vacuum that is exactly what might happen. In the so tissues, the extracellular fluid evaporates, creating painful pockets of vapour ("ebullism"); in the intravascular volume the evolution of bubbles produces "vapour lock" of the cardiac chambers, producing a cessation of circulation within 10-15 seconds. As the intrathoracic air content expands, the pressure on mediastinal structures also produces a profound vagal bradycardia."Some degree of consciousness will probably be retained for 9 to 11 seconds", the Bioastronautics Data Book helpfully remarks. Presumably, it would be acceptable to perform compression-only CPR in this scenario. In short, the immediate consequences of explosive decompression are: Pneumothorax and pneumomediastinum, because of the rapid expansion of intrathoracic gas Gas embolism, because of the same Decreased lung volumes because of the displacement of the diaphragm upwards by expanding gas in the abdominal contents Vagally mediated bradycardia, also due to the relative increase in intrathoracic pressure Shock, from multiple mechanisms, not the least of which being: Vapour lock by air emboli Decreased blood pressure and heart rate due to vagal stimulation Decreased venous return due to intrathoracic gas expansion Decreased level of consciousness due to a combination of poor perfusion and poor oxygenation, as well as microscopic gas emboli Expulsion of intestinal contents Most of these data are derived from cruel animal experiments performed by well-meaning villains such as Bancro & Dunn (1965). "A generalized muscle spasticity, a few gasps, momentary convulsive seizures, apnea, and gross swelling of the body and extremities" were reported; in spite of these phenomena all dogs exposed for less than 120 seconds survived, albeit usually with some neurological sequelae (eg. blindness). https://derangedphysiology.com/main/cicm-primary-exam/required-reading/respiratory-system/Chapter 923/physiological-effects-high-and-low-barom… 8/16 4/13/2021 Physiological effects of high and low barometric pressure | Deranged Physiology Human experience of sudden vacuum exposure seems to be thankfully limited; or at least, most of the time the subject is in no position to be rescued and studied. One oen-quoted case is described by Emanuel Roth (1968). A vacuum chamber technician was the victim. At an equivalent altitude of around 40,000m, "the subject decompressed his pressure suit in a vacuum chamber by disrupting a connection on his chamber umbilical hose", the narrative went. "The subject lost consciousness in 12 to 15 seconds after decompression. Clonic and tonic movements of the feet were noted. After only 20 seconds in a vacuum, the suit was recompressed to 3.7 psia. Within a period of 27 seconds the chamber was at 6 psia. He regained consciousness at this time. There was no recollection of chest or abdominal pain in the accident report." Extraterrestrial cases of accidental suit failure are poorly reported. An event oen quoted as "Landis, G.A. Personal communication, 1999" records the recollection of the astronaut Gregory Benne, which was apparently reported via a post he had made on the sci.space Usenet group: "Incidentally, we have had one experience with a suit puncture on the Shuttle flights. On STS-37, during one of my flight experiments, the palm restraint in one of the astronaut’s gloves came loose and migrated until it punched a hole in the pressure bladder between his thumb and forefinger. It was not an explosive decompression, just a little 1/8 inch hole, but it was exciting down here in the swamp because it was the first injury we’ve ever had from a suit incident. Amazingly, the astronaut in question didn’t even know the puncture had occurred; he was so hopped on adrenaline it wasn’t until after he got back in that he even noticed there was a painful red mark on his hand. He figured his glove was chafing and didn’t worry about it…. What happened: when the metal bar punctured the glove, the skin of the astronaut’s hand partially sealed the opening. He bled into space, and at the same time his coagulating blood sealed the opening enough that the bar was retained inside the hole." Any list of poorly reported space accidents must also mention the Soyuz 11 catastrophe, where the return capsule depressurised on reentry, killing the three crew members inside. Georgy Dobrovolskiy, Vladislav Volkov and Viktor Patsaev died as the consequence of what appears to be a valve leak. Communication was lost shortly aer the capsule undocked from the space station, and communication was lost with the crew, who were found lifeless upon their descent. It appeared that at an altitude of approximately 168 km, the cabin depressurised to a barometric pressure of 0 mmHg over approximately 100 seconds. An inspection of the ship's interior revealed that the shoulder straps of all the cosmonauts were unfastened, and the commander was tangled in his straps. Telemetery recording of these final moments observed that the respiratory rate of the crew increased to 40-50 in the four seconds following seal failure; death occurred aer 48-49 seconds. Onboard voice tapes reveal that the crew were able to identify the source of the leak within a few seconds, but the remaining TUC was too short. Changes in alveolar and atmospheric gas far below sea level e discussion of atmospheric and alveolar gas in free-range humans are far less informed, because there are more heights on earth than depths, and the depths are less thoroughly plumbed. Tan et al (2008), on trying to create some sort of overview for this topic, found themselves without anything to https://derangedphysiology.com/main/cicm-primary-exam/required-reading/respiratory-system/Chapter 923/physiological-effects-high-and-low-barom… 9/16 4/13/2021 Physiological effects of high and low barometric pressure | Deranged Physiology overview: "the authors emphasise that detailed pressure and density measurements within deep mines could not be found in the literature despite an intensive search, and probably do not exist". However, the change in temperature with depth is known - on average, for every kilometre of crust, the minesha heats up by 10-25 ºC. e deepest mine (currently, the Mponeng gold mine) has a rockface temperature of 66 ºC, and management ends up having to pump thousands of litres of ice slurry down there purely as a means of keeping the miners alive. Unfortunately, nobody seems to care about those miners' alveolar gas content (or their lives in general), and sexy British anaesthetists have never descended into that sha with an ABG machine, so we have no direct data to inform our discussion. Using the same formulae as above, it is possible to construct some intelligent speculations regarding atmospheric pressure, at least: us, theoretically at least, at the boom of a mine sha which penetrates 10km into the Earth's crust, you would be enjoying an atmospheric pressure of 2200 mmHg (2.8 atm), with an atmospheric PO2 of 466mmHg on room air. So; would you be …healthier… down there? Unlikely, given that the temperature would be around 150 ºC. But, let's consider a more plausible scenario, where hyperbaric conditions are experienced occupationally or therapeutically, i.e. with conditions made as pleasant and survivable as possible. Physiological effects of increased barometric gas pressure e most commonly encountered hyperbaric situation in CICM past papers is hyperbaric oxygen and this is discussed in some detail elsewhere. e effects and complications of high oxygen concentrations are described best in the chapter on the pharmacology of oxygen. To summarise here: Hyperbaric hyperoxia has significant toxicity, which manifests as: Tracheobronchitis Acute lung injury https://derangedphysiology.com/main/cicm-primary-exam/required-reading/respiratory-system/Chapter 923/physiological-effects-high-and-low-baro… 10/16 4/13/2021 Physiological effects of high and low barometric pressure | Deranged Physiology Hypertension Seizures If the inspired fraction of oxygen remains unchanged, raised barometric pressure still has undesirable effects, except now the nitrogen becomes harmful. A classic example of this is nitrogen narcosis, which manifests as "certain changes in personality and performance in men subjected to increased pressures of air" It is mainly seen in deep divers breathing compressed nitrogen/oxygen mixtures. ough most authors report "proper" party-level narcotic effects at 10-15 atmospheres of pressure (Pastena et al, 2005, and omas et al, 1976), there is clearly some psychomotor slowing even at 3 atmospheres of air pressure (Kiessling & Maag, 1962). Hyperbaric nitrogen toxicity manifests as: Muscular tremors Loss of coordination Memory deficits Confusion and psychosis So, with seizures on oxygen and delirium on nitrogen, a trend seems to emerge which might suggest that hyperbaric gases cause neurological complications. D'Agostino et al (2009) evolved this concept further in a discussion of hyperbaric gas effects on nervous system function, which can be summarised effectively by borrowing one of their concluding statements: "The neurological consequences of breathing hyperbaric gases are directly related to the gas' partial pressure, lipid solubility, and capacity to alter the physicochemical properties of adjoining membrane nanostructures through oxidation and mechanical perturbation" Following from this, one might surmise that gases which have low lipid solubility would be well tolerated under high pressures. is is probably true; helium has the lowest solubility in lipid membranes compared with other gases, and truly insane pressures of helium can be tolerated with apparently lile physiological effect. Effect of barometric pressure aside from gas toxicities Enough of the effects of gases, what about the pressure itsel? Dean & D'Agostino also have an excellent chapter on this topic in Neuman & om's Physiology and Medicine of Hyperbaric Oxygen Therapy which is somehow available online. In short, the effects of pressure itself are as far-reaching as one might expect from something which governs the very properties of maer and the rate of chemical reactions which maintain life. At any given constant temperature, the equilibrium constant of all chemical relationships is affected by the pressure variable, causing reactions to go faster or slower. Indeed, deep-sea organisms which live at extreme pressures (eg. 1100 atmospheres, at the boom of the Challenger Deep) have had to make major molecular modifications to their enzymes and lipid bilayers in order to function (Macdonald, 1997). For example, the tidepool snailfish Liparis florae has a version of lactate dehydrogenase which functions optimally at a pressure of around 60 MPa, where the LDH of surface-dwellers suffers from a greatly decreased activity (Gerringer et al, 2017). So, what is the uppermost limit of pressure for the sustained survival of complex organisms? Pradillon & Gaill have an excellent article outlining the challenges of survival at great depth. Under high pressure, delicate protein structures tend to unfold and denature. Deep sea fish have met the need to keep proteins stable under pressure by producing copious amounts of trimethylamine oxide (TMAO), https://derangedphysiology.com/main/cicm-primary-exam/required-reading/respiratory-system/Chapter 923/physiological-effects-high-and-low-baro… 11/16 4/13/2021 Physiological effects of high and low barometric pressure | Deranged Physiology but this is something limited by hyperosomolarity: it is an "idiogenic osmole", and beyond a certain intracellular concentration of this substance, intracellular osmolarity would increase to the point where much ATP would be used to pump water out of the cells. Given the extreme scarcity of metabolic substrate down in the oceanic trenches, this is unlikely to be viewed as a satisfactory solution by the locals. As the result of this, there may be a real biochemical constraint to the survival of vertebrates under extreme pressure, which Yancy et al (2014) put at 8400m, or approximately 840 atmospheres of pressure. at's fragile vertebrates, mind you. Supergiant amphipods look quite healthy as they scurry around in the Mariana Trench, and we have no clear idea as to how much deeper they could get. What about life in general? ere are solid chemical limits to what can be expected from unmodified carbon-based molecules under great pressure. Elo et al (2000) determined that the tertiary strurure of proteins begins to self-dismantle at a pressure of around 5000 atmospheres. At around the same pressure, the DNA strand loses its helical properties. Ultimately, at 15,000 atmospheres, the primary structure of proteins unravels, and they disintegrate into individual amino acids. In case anybody is interested, that's probably the pressure range one encounters under the lowermost cloud layer of Jupiter. One might at this stage point out that human beings are in fact adapted to life at sea level, and the discussion of Hadal crustaceans and gas giants is probably pointless to anyone who might be mainly interested in human physiology. What, then, is the limit of human survival at high pressure? e exact number is unknown, as to test it would require the nonsurvival of some of the subjects. We do know however that trained professionals can tolerate extreme pressure for short periods safely. e current record is held by eo Mavrostomos, who spent about 7 hours at a pressure of 70 atmospheres, equivalent to a depth of 701 metres. He was pressurised over about 18 days, and depressurised over 24 days (Gardee et al, 1992). e gas mixture he was breathing consisted of 99.5% helium and hydrogen in approximately 2:1 fractions. ere was only 0.5% oxygen, to maintain a PAO2 of less than 200 mmHg. No complex biochemical monitoring was undertaken, but the following signs and symptoms were observed, aributed mainly to the pressure effects themselves rather than to helium: Tremor Mild myoclonus Psychometric and intellectual performance were decreased Dyskinesia with mainly proprioceptive problems Decrease in appetite Mild shortness of breath General fatigue (which resolved with depressurisation to 65 atmospheres) Physiological effects of such massively increased barometric pressure include: Increased airway resistance due to increased viscosity of the gas mixture Increased work of breathing due to this, as well as due to the added weight of the gas being moved Hypoventilation results probably from Bradycardia: at pressures of around 5 atmospheres, heart rate decreases, albeit slightly (Linnarsson et al, in 1999, found the heart rate of their divers dropped by about 6 bpm on average). Diuresis is experienced during “exposure to moderate pressure (15 to 50 atmospheres), and is associated with a decrease in urine osmolality from reduced water reabsorption. A decrease in ADH secretion is thought to be the cause. https://derangedphysiology.com/main/cicm-primary-exam/required-reading/respiratory-system/Chapter 923/physiological-effects-high-and-low-baro… 12/16 4/13/2021 Physiological effects of high and low barometric pressure | Deranged Physiology So, 70 atmospheres is the record, and humans have gone no deeper. However, at even higher pressures, on the basis of animal studies, it is theorised that even helium will have a neurotoxic effect. It is not the fault of helium, which is inert as inert can be, but rather the effect of the pressure itself, exerted by aforementioned mechanisms of changing lipid membrane properties and chemical reaction rates. is was elegantly demonstrated by Brauer et al (1982). Rats exposed to helium at pressures in excess of 200 atmospheres were observed to develop incoordination followed by seizures; rats breathing a perfluorocarbon liquid mixture at a similar pressure developed exactly the same clinical features, suggesting that hydrostatic pressure itself was to blame. is probably represents some sort of maximum for multicellular organisms adapted to Earth surface pressures. Previous chapter: Abnormal capnography waveforms and their interpretation Next chapter: Age-related changes in respiratory physiology References Wya, Frank B. "Physiological Responses to Altitude: A Brief Review." Journal of Exercise Physiology Online 17.1 (2014). Brown, James PR, and Michael PW Groco. "Humans at altitude: physiology and pathophysiology." Continuing Education in Anaesthesia, Critical Care & Pain 13.1 (2013): 17-22. Tan, A., T. X. Zhang, and S. T. Wu. "Pressure and density of air in mines." (2008). Ortiz-Prado, Esteban, et al. "Partial pressure of oxygen in the human body: a general review." American journal of blood research 9.1 (2019): 1. Tarver, William J., and Jeffrey S. Cooper. "Aerospace, Pressure Effects Hypobaric." StatPearls [Internet]. StatPearls Publishing, 2018. Conkin, Johnny. "Equivalent air altitude and the alveolar gas equation." Aerospace medicine and human performance 87.1 (2016): 61-64. Groco, Michael PW, et al. "Arterial blood gases and oxygen content in climbers on Mount Everest." New England Journal of Medicine 360.2 (2009): 140-149. Welslau, Wilhelm. "Physiologic effects of increased barometric pressure." Handbook on Hyperbaric Medicine. Springer, Dordrecht, 2006. 31-47. Martin, D., and J. Windsor. "From mountain to bedside: understanding the clinical relevance of human acclimatisation to high-altitude hypoxia." Postgraduate medical journal 84.998 (2008): 622-627. Vogel, James A., and Charles W. Harris. "Cardiopulmonary responses of resting man during early exposure to high altitude." Journal of Applied Physiology 22.6 (1967): 1124-1128. Hall, F. G. "Interval of useful consciousness at various altitudes." Journal of applied physiology 1.7 (1949): 490-495. https://derangedphysiology.com/main/cicm-primary-exam/required-reading/respiratory-system/Chapter 923/physiological-effects-high-and-low-baro… 13/16 4/13/2021 Physiological effects of high and low barometric pressure | Deranged Physiology Naeije, Robert. "Physiological adaptation of the cardiovascular system to high altitude." Progress in cardiovascular diseases 52.6 (2010): 456-466. Ostadal, B., and F. Kolar. "Cardiac adaptation to chronic high-altitude hypoxia: beneficial and adverse effects." Respiratory physiology & neurobiology 158.2-3 (2007): 224-236. León-Velarde, Fabiola, et al. "Consensus statement on chronic and subacute high altitude diseases." High altitude medicine & biology 6.2 (2005): 147-157. Hannon, JOHN P., K. S. Chinn, and J. L. Shields. "Alterations in serum and extracellular electrolytes during high-altitude exposure." Journal of applied physiology 31.2 (1971): 266-273. Zubieta-Calleja, G. R., et al. "Altitude adaptation through hematocrit changes." Journal of physiology and pharmacology 58.5 (2007): 811-818. Greenleaf, J. E., et al. "Fluid-electrolyte shis and VO2max in man at simulated altitude (2,287 m)." Journal of Applied Physiology 44.5 (1978): 652-658. Jaminet, Alphonse. Physical Effects of Compressed Air: And of the Causes of Pathological Symptoms Produced on Man, by Increased Atmospheric Pressure Employed for the Sinking of Piers, in the Construction of the Illinois and St. Louis Bridge Over the Mississippi River at St. Louis, Missouri. R. & TA Ennis, stationers and printers, 1871. Armstrong, Harry G., and J. W. Heim. "Medical problems of high altitude flying." e Journal of Laboratory and Clinical Medicine 26.1 (1940): 263-271. Charles E. Billings, "Barometric Pressure," in Bioastronautics Data Book, Second edition, NASA SP3006, edited by James F. Parker and Vita R. West, 1973. Murray, Daniel H., et al. "Pathophysiology, prevention, and treatment of ebullism." Aviation, space, and environmental medicine 84.2 (2013): 89-96. Kolesari, G. L., and E. P. Kindwall. "Survival following accidental decompression to an altitude greater than 74,000 feet (22,555 m)." Aviation, space, and environmental medicine 53.12 (1982): 1211-1214. Bancro, Richard W., and James E. Dunn. "Experimental animal decompressions to a near-vacuum environment." (1965). Roth, Emanuel M. "Rapid/explosive/decompression emergencies in pressure-suited subjects." (1968). Hendrickx, Bart. "e Kamanin Diaries 1960-1963." Journal of the British Interplanetary Society 50.1 (1997): 33. Kiessling, Ralph J., and Clinton H. Maag. "Performance impairment as a function of nitrogen narcosis." Journal of Applied Psychology 46.2 (1962): 91. Pastena, Lucio, et al. "EEG paerns associated with nitrogen narcosis (breathing air at 9 ATA)." Aviation, space, and environmental medicine 76.11 (2005): 1031-1036. omas, J. R., L. S. Burch, and R. A. Banvard. "Interaction of hyperbaric nitrogen and oxygen effects on behavior." Aviation, space, and environmental medicine 47.9 (1976): 965-968. https://derangedphysiology.com/main/cicm-primary-exam/required-reading/respiratory-system/Chapter 923/physiological-effects-high-and-low-baro… 14/16 4/13/2021 Physiological effects of high and low barometric pressure | Deranged Physiology D'Agostino, Dominic P., Denis G. Colomb Jr, and Jay B. Dean. "Effects of hyperbaric gases on membrane nanostructure and function in neurons." Journal of applied physiology 106.3 (2009): 9961003. Dean, Jay B., and Dominic P. D’Agostino. "Pressure effects on human physiology." Physiology and Medicine of Hyperbaric Oxygen erapy (2008): 189-202. Macdonald, A. G. "Hydrostatic pressure as an environmental factor in life processes." Comparative Biochemistry and Physiology Part A: Physiology 116.4 (1997): 291-297. Yancey, Paul H., Wendy R. Blake, and James Conley. "Unusual organic osmolytes in deep-sea animals: adaptations to hydrostatic pressure and other perturbants." Comparative Biochemistry and Physiology Part A: Molecular & Integrative Physiology 133.3 (2002): 667-676. Benne, Peter B. "Inert gas narcosis and high-pressure nervous syndrome." Bove and Davis' Diving Medicine. WB Saunders, 2004. 225-239. Gardee, B., et al. "Hydra 10: a 701 msw onshore record dive using “Hydreliox.”." XIXth annual meeting of European undersea biomedical society on diving and hyperbaric medicine. Trondheim: SINTEF UNIMED. 1993. Dean, Jay B., et al. "Neuronal sensitivity to hyperoxia, hypercapnia, and inert gases at hyperbaric pressures." Journal of Applied Physiology 95.3 (2003): 883-909. Brauer, R. W., et al. "Paerns of interaction of effects of light metabolically inert gases with those of hydrostatic pressure as such--a review." Undersea biomedical research 9.4 (1982): 353-396. Linnarsson, Dag, et al. "Hyperbaric bradycardia and hypoventilation in exercising men: effects of ambient pressure and breathing gas." Journal of Applied Physiology 87.4 (1999): 1428-1432. Gerringer, M. E., J. C. Drazen, and P. H. Yancey. "Metabolic enzyme activities of abyssal and hadal fishes: pressure effects and a re-evaluation of depth-related changes." Deep Sea Research Part I: Oceanographic Research Papers 125 (2017): 135-146. Yancey, Paul H., et al. "Marine fish may be biochemically constrained from inhabiting the deepest ocean depths." Proceedings of the National Academy of Sciences 111.12 (2014): 4461-4465. Pradillon, Florence, and Françoise Gaill. "Pressure and life: some biological strategies." Life in Extreme Environments. Springer, Dordrecht, 2006. 341-355. Elo, Mika A., et al. "Differential regulation of stress proteins by high hydrostatic pressure, heat shock, and unbalanced calcium homeostasis in chondrocytic cells." Journal of cellular biochemistry 79.4 (2000): 610-619. https://derangedphysiology.com/main/cicm-primary-exam/required-reading/respiratory-system/Chapter 923/physiological-effects-high-and-low-baro… 15/16 4/13/2021 Physiological effects of high and low barometric pressure | Deranged Physiology https://derangedphysiology.com/main/cicm-primary-exam/required-reading/respiratory-system/Chapter 923/physiological-effects-high-and-low-baro… 16/16