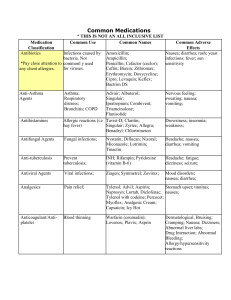
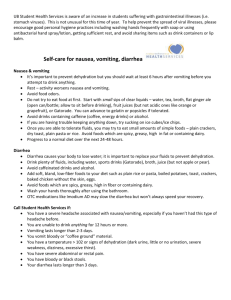
Central nervous system ADHD Pathophysiology: Dysregulation of transmitters, Serotonin, norepinephrine, dopamine Epidemiology: Usually occurs in children before age 7 years, More common in boys Characteristics: Inattentiveness, inability to concentrate, restlessness, hyperactivity, inability to complete tasks, impulsivity Narcolepsy Characteristics: Recurrent attacks of drowsiness and sleep during daytime, Unable to control sleep, Falling asleep while, Driving, Talking, Eating, Standing Methylphenidate (Ritalin) Action: Modulates serotonergic pathways by affecting changes in dopamine transport Use: ADHD, narcolepsy, increase attention span Interactions: Caffeine may increase effects, Increases effects of oral anticoagulants, barbiturates, anticonvulsants, TCAs, MAOIs, Decreased effects of antihypertensive, May alter insulin effects Side effects/adverse reactions: Tachycardia, palpitations, hypertension, dysrhythmias, Restlessness, tremors, irritability, Dizziness, headache, blurred vision, Euphoria, confusion, Anorexia, dry mouth, diarrhea, constipation, weight loss, Seizures, erectile dysfunction Nursing interventions: Teach patient to take the drug before meals. Advise patients to avoid foods that contain caffeine. Report irregular heartbeat. Record height, weight, and growth of children. Avoid alcohol, caffeine. Use sugarless gum to relieve dry mouth. Do not stop abruptly; taper off to avoid withdrawal symptoms. Anorexiants Action: Cause stimulant effect on hypothalamic and limbic areas of brain to suppress appetite – Should not be given to children under 12 Side effects: Nervousness, irritability, insomnia, Tachycardia, hypertension, Palpitations, seizures Medications: • Benzphetamine HCl (Didrex) • Diethylpropion HCl (Tenuate) • Phentermine HCl (Suprenza) • Phentermine-topiramate (Qsymia) • Phendimetrazine (Bontril) • Lorcaserin (Belviq) Doxapram (Dopram) Uses: Respiratory depression caused by overdose, pre- and postanesthetic respiratory depression, and chronic obstructive pulmonary disease (COPD) Onset of action: 20 to 40 seconds, peak within 2 minutes Side effects: Hypertension, tachycardia, trembling, convulsions Theophylline Use: stimulate respiration in newborns Side effects: Restlessness, tremors, twitching, palpitations, insomnia, Diuresis, tinnitus, nausea, diarrhea, Psychological dependence Barbiturates Side effects: Residual drowsiness (hangover) Vivid dreams, nightmares, Drug dependence, Drug tolerance, Excessive depression, Respiratory depression, Hypersensitivity Types – Long-acting – Intermediate-acting – Short-acting – Ultrashort-acting Restricted to short-term use – 2 weeks or less – Because of side effects, including drug tolerance Interactions: Alcohol, opioids, other sedative-hypnotics, Decreases effects of oral anticoagulants, glucocorticoids, tricyclic antidepressants, quinidine Benzodiazepines as hypnotics Action • Interacts with neurotransmitter GABA to reduce neuron excitability Use • Reduce anxiety, treat insomnia Side effects: Residual drowsiness (hangover), Vivid dreams, nightmares, Drug dependence Drug tolerance, Excessive depression, Respiratory depression, Hypersensitivity Medications: Flurazepam (Dalmane), Alprazolam (Xanax), Temazepam (Restoril), Triazolam (Halcion), Estazolam (ProSom), Quazepam (Doral) Butabarbital Side effects: slow heart rate, weak or shallow breathing, extreme drowsiness, feeling light-headed, or fainting, rapid breathing, gasping for breath, confusion, hallucinations, unusual thoughts, nightmares; or, overactive reflexes, feeling restless or irritable, severe agitation or nervous feeling. Contraindicated: high amount of ammonium in the blood, Porphyria, Anemia, decreased blood platelets, low levels of a type of white blood cell called neutrophils, suicidal thoughts, Alcoholism, drug abuse. Epilepsy Patho: abnormal electric discharges from cerebral neurons Characteristics: loss of consciousness, convulsive movements. Cause: Unknown, secondary to trauma, anoxia, infection, fever, electrolyte or acid imbalances. Phenobarbital Action: enhances GABA activity Use: tonic clonic, partial, myoclonic seizures, status epilepticus Therapeutic level 20-40 mcg/ml Risks: sedation and patient tolerance to the drug. Discontinuance of phenobarbital should be gradual to avoid recurrence of seizures. Succinimide (Zarontin) Action: Decreases calcium influx Use: Absence seizures Therapeutic serum range of ethosuximide is 40 to 100 mcg/mL. Adverse effects: include blood dyscrasias, renal and liver impairment, and systemic lupus erythematosus. Iminostilbene (Carbamazepine) Action: Effective in treating refractory seizure disorders that have not responded to other anticonvulsant therapies Uses: grand mal and partial seizures, psychiatric disorders (e.g., bipolar disorder),trigeminal neuralgia (as an analgesic), and alcohol withdrawal Therapeutic serum range of carbamazepine is 5 to 12 mcg/mL. An interaction may occur when grapefruit juice is taken with carbamazepine (Tegretol), causing possible toxicity Valproate (Valproic acid) Action: Used to treat petit mal, grand mal, and mixed types of seizures Safety and efficacy of this drug has not been established for children younger than 2 years of age. Caution in patients with liver disorders, because hepatotoxicity is one of the possible adverse reactions. Liver enzymes should be monitored. Therapeutic serum range is 50 to 150 mcg/mL. Hydantoins: Phenytoin (Dilantin) Contraindications Pregnancy (teratogenic) Therapeutic serum level 10 to 20 mcg/mL Side effect/adverse reactions Gingival hyperplasia, nystagmus, diplopia Headache, dizziness, slurred speech, alopecia Purple glove syndrome, ventricular fibrillation Depression, suicidal ideation Hyperglycemia, GI distress, urine discoloration Thrombocytopenia, leukopenia Stevens-Johnson syndrome Drug interactions: Increased effects with cimetidine (Tagamet), INH, sulfonamides, Decreased effects with folic acid, antacids, calcium, sucralfate, antineoplastics, antipsychotics, primrose, ginkgo, Decreased effects of anticoagulants, oral contraceptives, antihistamines, dopamine, theophylline Nursing interventions: Shake suspension well for 5 minutes, Monitor serum drug levels, Safety: Protect from environmental hazards, driving, Warn female patients taking oral contraceptives to use additional contraception, Warn patient to avoid certain herbs, alcohol, and other CNS depressants, Warn patient not to discontinue abruptly, Patient will need frequent oral hygiene and dental check-ups, Diabetics must monitor glucose level, Tell each patient to take drug at same time every day, Warn of harmless pinkish red or brown urine, Teach patient to report sore throat, bruising, nosebleeds. Status epilepticus Treatment: Diazepam, Lorazepam, Followed by phenytoin IV, For continued seizures: midazolam, propofol, Slow IV administration to avoid respiratory depression Anticonvulsants and Pregnancy Seizure episodes increase 25% in women with epilepsy who are pregnant. Hypoxia that may occur during seizures places both the pregnant patient and the fetus at risk. Many anticonvulsant drugs have teratogenic properties that increase the risk for fetal malformations. Anticonvulsant drugs tend to act as inhibitors of vitamin K, contributing to hemorrhage in infants shortly after birth. Anticonvulsants also increase the loss of folate (folic acid) in pregnant patients. Anticonvulsants and Febrile Seizures Seizures associated with fever usually occur in children between the ages of 3 months and 5 years. Epilepsy develops in approximately 2.5% of children who have had one or more febrile seizures. Prophylactic anticonvulsant treatment such as phenobarbital or diazepam may be indicated for high-risk patients. Valproic acid should not be given to children younger than 2 years because of its possible hepatotoxicity Anticholinergics Parasympatholytic– Benztropine (Cogentin) Trihexyphenidyl HCl (Artane) Biperiden (Akineton) Action: inhibit the release of acetylcholine Reduce the rigidity and some of the tremors characteristic of parkinsonism, Minimal effect on bradykinesia, Used to treat drug-induced parkinsonism, or pseudoparkinsonism Nursing Interventions: Monitor vital signs, Monitor urine output for early detection of urinary retention, Increase fluid intake, fiber, and exercise to avoid constipation, Observe for involuntary movements, Advise patient to avoid alcohol, cigarettes, caffeine, and aspirin to decrease gastric acidity, Encourage patient to relieve dry mouth with ice chips, hard candy, or sugarless chewing gum, Suggest use of sunglasses for photophobia. Dopaminergics Carbidopa-levodopa (Sinemet) Action: converted to dopamine, increases mobility Side effects: Fatigue, insomnia, Dry mouth, Blurred vision, Orthostatic hypotension, palpitations, dysrhythmias, urinary retention, Nausea, vomiting, Dyskinesia, psychosis, severe depression Drug interactions: Decrease levodopa effect with: Anticholinergics, Phenytoin, Tricyclic antidepressants, MAO inhibitors, Benzodiazepines, Phenothiazines, Vitamin B6 Acetylcholinesterase Inhibitors/Cholinesterase Inhibitors: Tacrine (Cognex), donepezil (Aricept), rivastigmine (Exelon), galantamine (Razadyne) Action: Allow more acetylcholine in neuron receptors, Increase cognitive function Use: Mild to moderate Alzheimer’s disease Rivastigimine, Tacrine, donepezil Side effects: Anorexia, nausea, vomiting, diarrhea, constipation, abdominal pain, GI bleeding, dizziness, depression, peripheral edema, dry mouth, dehydration, restless legs syndrome, nystagmus Adverse reactions: seizures, bradycardia, orthostatic hypotension, cataracts, myocardial infarction, heart failure Myasthenia Gravis Patho: Autoimmune disorder, Antibodies attach to acetylcholine receptor sites, obstruct binding of acetylcholine, and destroy receptor sites, Lack of acetylcholine impairs transmission of messages at neuromuscular junctions Characteristics: Muscular weakness and fatigue, Respiratory muscle paralysis, ptosis, difficulty chewing and swallowing Myasthenic crisis Patho: Severe muscle weakness, May involve diaphragm and intercostal muscles Triggers: Inadequate dosing, Infection, Emotional stress, Menses, pregnancy, Surgery, trauma, Hypokalemia, alcohol intake, Medication interactions Treatment: edrophonium (tensilon), and neostigmine (prostigmin) Cholinergic crisis Patho: Usually occurs within 30 to 60 minutes after taking anticholinergic medications Triggers: Triggered by overdosing, Severe muscle weakness (Possible paralysis and arrest, Abnormal purespiratorypil constriction, Excess salivation, Pallor, sweating, vertigo, GI distress Bradycardia, Fasciculations Acetylcholinesterase inhibitors (AChE inhibitors) Neostigmine (Prostigmin): shortacting Edrophonium (Tensilon): ultrashortacting for diagnosing Pyridostigmine (Mestinon): intermediate-acting Ambenonium (Mytelase): long-acting Action: Transmission of neuromuscular impulses by preventing destruction of Ach Use: to treat MG Side effects: GI disturbances (nausea, vomiting, diarrhea, abdominal cramps), Increased salivation, Tearing, Miosis (constricted pupil of the eye), Blurred vision, Bradycardia, Hypotension No response to these medication = Prednisone Nursing Interventions: Administer doses on time. Take drug before meals if possible. Monitor drug effectiveness. Have antidote available for cholinergic crisis (Atropine). Encourage patient to wear medical identification. Multiple Sclerosis Patho: Autoimmune disorder: Attacks myelin sheath of nerve fibers in brain and spinal cord, Causes lesions or plaques Characteristics: Remission and exacerbations, weakness, spasticity in extremities, diplopia Treatment: Immunomodulators ◦ First-line treatment ◦ Slows disease progression and prevents relapses, Immunosuppressants, Sphingosine 1-phosphate receptor modulator, Monoclonal antibody, Corticosteroids (Reduces edema and acute inflammation) Cyclobenzaprine Action: Relax skeletal muscles Use: Relieves muscle spasm Side effects: Anticholinergic effects (blurred vision, dry mouth, tachycardia, urine retention, constipation), Drowsiness, dizziness, headache, nervousness GI distress, unpleasant taste, dysrhythmias Antipsychotics Treat: Mental illness to improve thought processes and behavior Action: Block dopamine receptors in brain When dopamine is blocked, extrapyramidal symptoms (EPS) of parkinsonism occur. • Tremors, masklike facies, rigidity, shuffling gait may develop. Typical antipsychotics • Phenothiazines • Block norepinephrine causing sedative and hypotensive effects early in treatment. • Nonphenothiazines • Block only the neurotransmitter dopamine Atypical antipsychotics • Treats schizophrenia and other psychotic disorders in patients not responding to or intolerant of typical antipsychotics • Decreased side effects • Often used as first-line therapy Adverse reactions: • Extrapyramidal syndrome • Stooped posture, masklike facies, rigidity, tremors at rest • Shuffling gait, pill-rolling motion of hands, bradykinesia • Acute dystonia, akathisia, tardive dyskinesia • Neuroleptic malignant syndrome • Excess agitation, altered mental status • Exhaustion, dehydration • Muscle rigidity, hyperthermia, profuse diaphoresis • Blood pressure fluctuations, tachycardia, dysrhythmias • Seizures, rhabdomyolysis • Respiratory and renal failure, coma Extrapyramidal symptoms—four types • Dystonic reactions/acute dystonia • Pseudoparkinsonism (tremor, muscular rigidity, masklike expression, shuffling gait, loss/weakness of motor function) • Akathisia (pacing, rocking, subjective feelings of anxiety and restlessness) • Tardive dyskinesia (hyperkinetic abnormal movements) Fluphenazine (typical) Action: Blocks dopamine receptors in brain Use: Manages symptoms of schizophrenia and psychosis Interactions: Increase depression when taken with alcohol or other CNS depressants; kava kava may increase EPS, Increased effects with MgSO4 , lithium, beta blockers Side effects: Sedation, dizziness, headache, seizures, Dry mouth, nasal congestion, blurred vision, photosensitivity, urinary retention, GI distress, peripheral edema, tachycardia, EPS Haloperidol (typical) Action: Blocks dopamine receptors Use: Treats psychoses, schizophrenia, attention deficit/hyperactivity disorder, Tourette’s syndrome Contraindications: Narrow-angle glaucoma, CNS depression, Severe liver, kidney, and cardiovascular disease, Blood dyscrasias Side effects: Drowsiness, headache, insomnia, Dry mouth, blurred vision, photosensitivity, Tachycardia, orthostatic hypotension, dysrhythmias, Seizures, weight gain, Urinary retention, sexual dysfunction, Blood dyscrasias, EPS, NMS Interactions: Increased sedation with alcohol, CNS depressants, Increased toxicity with anticholinergics, Decreased effects with phenobarbital, carbamazepine, caffeine Clozapine (atypical) Use: Severe schizophrenic patients unresponsive to traditional antipsychotics Side effects: Dizziness, sedation, constipation, tachycardia, orthostatic hypotension, Tremors, occasional rigidity, Seizures, agranulocytosis, Low possibility of EPS Risperidone Use: Manage symptoms of psychosis, Treats positive and negative symptoms of schizophrenia Side effects: Sedation, headaches, photosensitivity, EPS, seizures, Dry mouth, weight gain, Tachycardia, orthostatic hypotension, Urinary retention, sexual dysfunction, Low possibility of EPS and tardive dyskinesia Anxiolytics Lorazepam Action: inhibits GABA neurotransmission by binding to specific benzodiazepam receptors Use: Anxiolytic, antiseizure, sedative-hypnotic, preoperative drug, substance abuse withdrawal Side effects: Drowsiness, dizziness, ataxia, restlessness, weakness, Headache, confusion, amnesia, blurred vision, GI distress, sleep disturbance, hallucinations, Bradycardia, hypotension/hypertension, Seizures, suicidal ideation, NMS, respiratory depression Discontinuation: gradually decrease dose over several days Withdrawal symptoms: Develops slowly, in 2 to 10 days, and may last several weeks • Withdrawal symptoms • Tremor, agitation, nervousness • Sweating, insomnia • Anorexia, muscle cramps Buspirone Action: Binds to serotonin and dopamine receptors, May not be effective until 1 to 2 weeks after continuous use Side effects: Drowsiness, dizziness, Headache, excitement, Nausea, nervousness Interactions: grape juice can lead to toxicity Tricyclic Antidepressants (TCA) Action: Blocks uptake of neurotransmitters norepinephrine and serotonin in brain, Elevates mood, increases interest in ADLs, decreases insomnia, Blocks histamine receptors which leads to sedation, Blocks cholinergic receptors which leads to anticholinergic effects Use: Major depression Side effects: Drowsiness, dizziness, blurred vision, Dry mouth and eyes, GI distress, Urinary retention, sexual dysfunction, Weight gain, seizures, Sleep-related behaviors, suicidal ideation, Orthostatic hypotension, dysrhythmias, Blood dyscrasias, cardiotoxicity, EPS, NMS Interactions: Alcohol and other CNS depressants potentiate CNS depression, MAOIs may lead to toxic psychosis, cardiotoxicity, Antithyroid drugs may increase dysrhythmias Selective Serotonin Reuptake Inhibitors (SSRI) Action: block uptake of neurotransmitter serotonin Uses: Major depression, Anxiety disorders, Obsessive-compulsive disorder, Panic disorders, Phobias, Posttraumatic stress disorder, Prevention of migraine headaches, Decrease premenstrual tension syndrome Interactions: Increased sedation with alcohol and other CNS depressants, grapefruit juice can lead to toxicity Side effects: Headache, nervousness, Blurred vision, insomnia, Dry mouth, GI distress, Sexual dysfunction, suicidal ideation, side effects often decrease over 1 to 4 weeks Atypical Antidepressants Action: Affect one or two of the three neurotransmitters: serotonin, norepinephrine, and dopamine. Use: Major depression, reactive depression, anxiety Interaction: Do not take with MAOIs and do not use within 14 days after discontinuing MAOIs, Trazodone may have a potential drug interaction with ketoconazole, ritonavir, and indinavir that may lead to increased trazodone levels and adverse effects Monoamine Oxidase Inhibitors (MAOI’s) Action: Monoamine oxidase enzyme inactivates norepinephrine, dopamine, epinephrine, and serotonin Use: Depression not controlled by TCAs and second-generation antidepressants Interactions: CNS stimulants such as vasoconstrictors and cold medications containing phenylephrine and pseudoephedrine can cause a hypertensive crisis when taken with an MAOI. Food interactions: Foods that contain tyramine, Some cheeses, cream, yogurt, coffee, chocolate, bananas, raisins, Italian green beans, liver, pickled foods, sausage, soy sauce, yeast, beer, and red wines can cause a hypertensive crisis. Side effects: Agitation, restlessness, insomnia, Anticholinergic effects, Orthostatic hypotension, Hypertensive crisis from tyramine interaction Lithium Therapeutic serum range: 1.0 to 1.5 mEq/L Action: Alteration of ion transport in muscle and nerve cells, Increased receptor sensitivity to serotonin Use: Bipolar disorder manic episodes Side effects: Headache, drowsiness, dizziness, blurred vision, Restlessness, tremors, memory impairment, Dry mouth, metallic taste, GI distress ◦ Hypotension, dysrhythmias, Edema of hands and ankles, dehydration, Increased urination, blood dyscrasias, NMS, Serotonin syndrome, nephrotoxicity Interactions: Increased lithium level with ◦ Thiazides, methyldopa, haloperidol, NSAIDs, antidepressants, theophylline, phenothiazines Decreased lithium with caffeine, loop diuretics Gastrointestinal system Antiemetics Dopamine antagonist: Phenothiazine antiemetics: Chlorpromazine (Thorazine) ◦ Prochlorperazine edisylate (Compazine) ◦ Promethazine (Phenergan) Action: Act on CTZ, block dopamine receptors Use: Postoperative nausea, vomiting, Chemotherapy, radiation sickness Side effects: moderate sedation, hypotension, EPS, CNS effects, and mild anticholinergic symptoms Serotonin antagonists: Ondansetron (Zofran), granisetron (Kytril), dolasetron (Anzemet), palonosetron (Aloxi) Side effects: headache, diarrhea, dizziness, and fatigue Action: Block serotonin receptors in CTZ, Block afferent vagal nerve terminals in upper GI tract Use: Nausea and vomiting from chemotherapy, Postoperative nausea and vomiting Cannabinoids Dronabinol (Marinol) Actions: alleviate nausea and vomiting resulting from cancer treatment Use: nausea and vomiting from cancer treatment or chemotherapy Contraindicated: psychiatric disorders Side effects: mood changes, euphoria, drowsiness, dizziness, headaches, depersonalization, nightmares, confusion, incoordination, memory lapse, dry mouth, orthostatic hypotension or hypertension, and tachycardia Metoclopramide (Reglan) Action: Suppress impulses to CTZ Use: in the treatment of postoperative emesis, cancer chemotherapy, and radiation therapy Side effects: High doses can cause sedation and diarrhea, Occurrence of EPS is more prevalent in children than in adults, Contraindicated with GI obstruction, hemorrhage, or perforation Emetics Ipecac (OTC) Action: Stimulates CTZ and acts directly on gastric mucosa Use: Induces vomiting after toxic substance Caution: Avoid vomiting if substance is caustic or petroleum, If vomiting contraindicated, activated charcoal or gastric lavage can be used. Administration: Use ipecac syrup, not ipecac fluid extract, Take with a glass of water, not with milk or carbonated beverage, Vomiting occurs in 15 to 30 minutes, If vomiting does not occur, give activated charcoal, Gastric lavage may be needed if vomiting does not occur Diarrhea Causes: Spoiled food or excessively spicy foods, bacteria, drug reactions, fecal impactions, laxative abuse, malabsorption disorders, bowel tumor, inflammatory bowel disease, stress, anxiety Nonpharmacological measures: Clear liquids, Oral solutions (Gatorade; Pedialyte or Rehydralyte [both for use in children]), IV electrolyte solutions Traveler’s diarrhea Acute diarrhea: Usually caused by E. coli, Fluoroquinolone antibiotics, Loperamide (Imodium) Preventions: Traveler’s diarrhea can be reduced by drinking bottled water, washing fruit, and eating cooked vegetables. Meats should be cooked until well done. Opiates and opiate-related agents: Diphenoxylate with atropine (Lomotil) Opiates decrease GI motility, Opiates may cause respiratory depression, Especially children and older adults, May cause physical dependence, Atropine contraindicated in glaucoma. Adsorbents Colestipol and cholestyramine (Questran) Actions: Colestipol is an oral cholesterol-lowering drug that is not absorbed from the intestine into the body. Rather, it works by binding to bile acids in the intestine and promoting the elimination of bile acids in the stool. Used: diarrhea Side effects: Constipation, stomach/abdominal pain, gas, nausea, and vomiting may occur. Contraindication: Biliary cirrhosis, biliary obstruction, cholelithiasis, Constipation, dysphagia, GI obstruction, hemorrhoids, ileus, Hypertriglyceridemia, Coagulopathy, Hypothyroidism, Renal disease, Phenylketonuria, Pregnancy. Constipation Causes: Bowel obstruction, fecal impaction, Chronic laxative use, ignoring urge to defecate, Neurologic disorders, Side effect of drugs, Lack of exercise, Insufficient consumption of fiber and/or water Nonpharmacologic treatment: Diet (high fiber), Water, Exercise, Routine bowel habits Psyllium (Metamucil) Action: Absorb water into intestines, increase bulk and peristalsis Results: 8- 12 hours Side effects: Abdominal cramps, Excess laxative, Nausea, vomiting, gas, diarrhea Sucralfate (Carafate) Action: Combines with protein to form thick paste covering ulcer, protects from acid and pepsin Side effects: Constipation Nursing interventions: Given 30 minutes before meals and bedtime Bisacodyl (Dulcolax), senna (Senokot) Action: Increase peristalsis by irritating sensory nerve endings in intestinal mucosa Results: orally 6 to 12 hours, rectally 15 to 60 minutes Side effects: Abdominal cramps, weakness, reddish brown urine, diarrhea Docusate sodium (Colace) Action: Lowers surface tension, Promotes water accumulation in intestine, Emulsifies and lubricates feces for easier passage Use: Prevent constipation, Reduce straining postsurgery or myocardial infarction Side effects: Abdominal cramping, nausea, vomiting, diarrhea Polyethylene glycol, Lactulose (Chronulac) Action: Hyperosmolar salts pull water into colon and increase water in feces to increase bulk, which stimulates peristalsis. Side effects: Fluid and electrolyte imbalances, hypotension, weakness Peptic ulcers Symptoms: Gnawing, aching pain after eating Predisposing factors/risk factors: Helicobacter pylori (H. pylori), Mechanical, Genetic, Environmental, Drugs, Stress ulcer following a critical situation GERD Information on gerd: Inflammation of the esophageal mucosa caused by reflux of gastric acid content into the esophagus, Main cause is an incompetent lower esophageal sphincter, Smoking tends to accelerate the disease process, Medical treatment for GERD is similar to the treatment for peptic ulcers. Nonpharmacologic measures for both Peptic ulcers and GERD: Avoid tobacco, Avoid alcohol, Avoid hot, spicy, and greasy foods, Take any NSAIDs, including aspirin and oral glucocorticoids, with food or in decreased dosage, Sit upright, Do not eat before bedtime, Wear loose-fitting clothing. Antiulcer drugs Understanding: Tranquilizers Anticholinergic drugs Antacids H2 blockers Proton pump inhibitors Pepsin inhibitor Prostaglandin E1 analog Tranquilizers: Chlordiazepoxide (Librium), Clidinium bromide (Quarzan), Reduce vagal stimulation, decrease anxiety Anticholinergics: Propantheline (Pro-Banthine), Inhibits release of HCl by blocking acetylcholine and histamine, Take before meals Antacids Sodium bicarbonate (Alka-Seltzer), Calcium carbonate (Tums), Magnesium (Mg) hydroxide/aluminum hydroxide (Maalox), Aluminum (Al) hydroxide (Amphojel) Proton pump inhibitors Omeprazole (Prilosec), Lansoprazole (Prevacid), Rabeprazole (Aciphex), Pantoprazole (Protonix), Esomeprazole (Nexium), Dexlansoprazole (Dexilant), Action: Reduce gastric acid by inhibiting hydrogen/potassium ATPase Side effects: Headache, insomnia, dizziness, dry mouth, flatulence, abdominal pain Histamine2 blockers: Cimetidine (Tagamet), ranitidine (Zantac), famotidine (Pepcid), nizatidine (Axid) Action: Reduce gastric acid by blocking H2 receptors of parietal cells in stomach, Promote healing of ulcer by eliminating cause Side effects: Headaches, dizziness, diarrhea, constipation, reversible impotence, gynecomastia Interactions: Cimetidine interacts with oral anticoagulants, theophylline, caffeine, phenytoin (Dilantin), diazepam (Valium), propranolol (Inderal), phenobarbital, and calcium channel blockers. Cimetidine can cause an increase in blood urea nitrogen (BUN), serum creatinine, and serum alkaline phosphatase. Neither cimetidine nor ranitidine should be taken with antacids. Inflammation Nonspecific immunity First line: Mechanical or chemical barriers, reflexes Second line: Phagocytosis, inflammation, fever, protective proteins, natural killer cells Action second line: Leukocytes go to site of infection (Diapedesis, Chemotaxis), they eat cellular debris and pathogens Interferons are secreted by cells infected by a virus. Interferons protect other cells from viral replication. Complement proteins assist WBCs. Nk cells: A lymphocyte that acts nonspecifically, Effective against many microbes and certain cancer cells Signs: redness, heat, swelling, pain, fever Specific immunity Third line: B and T lymphocytes or B and T cells T cells: Cell-mediated immunity B cells: Antibody-mediated immunity Macrophages: Help activate T and B cells Action of T cells: Macrophage ingests antigen, Antigen presentation: Clone produced, Killer T cell, Helper T cells, Suppressor T cells, Memory T cells Action of B cells: Macrophage ingests antigen, Antigen presentation: B cells and helper T cells activated, Clone formed (Plasma cells, Memory B cells) Antigen, antibody, immunoglobulin: Antigen: Stimulates formation of antibodies Antibody: Secreted by B cells, also called immunoglobulins Antigen: antibody interaction agglutination Types of immunoglobulins: Immunoglobulin G (IgG), Immunoglobulin A (IgA), Immunoglobulin M (IgM), Immunoglobulin E (IgE) Chemical Mediators Released during inflammatory response, Produces vasodilation, Capillaries become leaky, Causes tissue swelling, Responsible for symptoms of anaphylaxis: itching, pain, edema, vasodilation, bronchoconstriction At injury site: Prostaglandins, Histamine, Leukotrienes, Bradykinin, Complement Cox system Cyclooxygenase (COX) enzyme: Converts arachidonic acid into prostaglandins ▪ Has two enzyme forms: ▪ COX-1: protects stomach lining and regulates blood platelets ▪ COX-2: triggers inflammation and pain Signs of inflammation Erythema, Swelling, Pain, Heat, Function loss Non pharmological ways to treat inflammation (RICE) Rest, Ice, Compression, Elevation Aspirin Action: Treats inflammation by inhibiting Cyclooxygenase (COX) Therapeutic levels: Therapeutic serum salicylate level ▪ 15 to 30 mg/dL Side effects: Irritates digestive system, May cause bleeding, Anaphylaxis, Poisoning (toxicity), Tinnitus (hearing loss), dizziness, headache, confusion hepatotoxicity, leukocytosis, thrombocytopenia, Severe: convulsions, coma, Avoid in Children: Reye’s syndrome! Interventions: Obtain health history, Monitor VS, Monitor serum levels, Monitor Renal function, Platelets, coagulation studies, Monitor for abdominal pain, black stools, urine output, tinnitus, Avoid in children under 19 Celecoxib (Celebrex) Action: No inhibition of COX-1, does not cause GI bleeding or ulcers Side effects: Back pain, upset pain, dizziness, headache, Hypertension Acetaminophen Action: reduce fever by direct action at level of hypothalamus and, dilation of peripheral blood vessels enabling sweating and dissipation of heat Side effects: Liver damage, Allergic reactions (angioedema, dyspnea) Interventions: Obtain health history, Monitor VS (Temp), Assess Allergy, Monitor Hepatic Function, LFT’s: ALT, AST, Increase fluid intake, Teach patient to avoid ETOH Prednisone (Meticorten) Action: metabolized to an active form of glucocorticoid Use: to treat inflammation Side effects: Long-term therapy may result in Cushing syndrome Interventions: Obtain health history, Monitor VS (BP & HR), Assess Labs (CBC, Glucose, electrolytes), Daily weight, Monitor signs of infection, osteoporosis, fluid retention/Cushing's, mood changes Gout Patho: Inflammatory disease of joints, tendons, and other tissues, Usually occurs in great toe Defect in purine metabolism leads to uric acid accumulation: Purine-containing foods: organ meats, sardines, salmon, gravy, herring, liver, meat soups, and alcohol (especially beer) Colchicine (Colcrys) Action: Inhibit migration of leukocytes to inflamed site (Acute attacks) Side effects: GI distress (take with food) Allopurinol (Zyloprim) Action: Decreases production of uric acid, Prophylactic to prevent gout attacks Interventions: Monitor CBC, liver enzymes, renal function, Yearly eye examinations for visual changes, Avoid alcohol, caffeine, foods high in purines and thiazide diuretics that increase uric acid level, Advise patient to increase fluid intake to increase uric acid excretion. Pain Types of pain: Acute, Chronic, Cancer, Somatic, Superficial, Vascular, Visceral PCA Pump Medications used: Morphine most often used for PCA, Also fentanyl, hydromorphone Loading dose, predetermined safety limits, Lockout mechanism, Near-constant analgesic level Morphine Action: Morphine binding to opioid receptors blocks transmission of nociceptive signals, signals painmodulating neurons in the spinal cord, and inhibits primary afferent nociceptors to the dorsal horn sensory projection cells. Side effects: Drowsiness, dizziness, euphoria, Confusion, depression, miosis, blurred vision, GI distress, flatulence, constipation, Orthostatic hypotension, weakness, Urinary retention, Psychological dependence, Respiratory depression Assessment: Determine drug history and check for drug allergies. Assess the type of pain, location, and duration before giving opioids Nursing diagnoses: Pain, Acute related to surgical tissue injury. Breathing Pattern, Ineffective related to excess morphine dosage. Planning: The patient’s pain will be reduced or alleviated. Nursing interventions: Administer morphine before pain reaches its peak to maximize drug effectiveness. Monitor vital signs frequently to detect respiratory changes. Check for pupil changes and reaction. Have naloxone available as an antidote to reverse respiratory depression if morphine overdose occurs Hydromorphone Use: Analgesic effect is approximately six times more potent than morphine Side effects and adverse reactions: Drowsiness, dizziness, confusion, Weakness, constipation, Miosis, tolerance, dependence, Respiratory depression, urinary retention, Fewer hypnotic effects and less GI distress than morphine Narcan Use: suspected opioid overdose Side effects: flushing, dizziness, tiredness, weakness, nervousness, restlessness, irritability, body aches Migraine Symptoms: Characteristics Unilateral throbbing pain Nausea, vomiting, photophobia, Triggers: Cheese, chocolate, red wine, aspartame, fatigue, stress, monosodium glutamate, missed meals, odors, light, hormone changes, drugs, weather, too much or too little sleep Cluster headaches Characteristics: Severe unilateral nonthrobbing pain, Usually located around eye, Occur in a series of cluster attacks, One or more attacks every day for several weeks, Not associated with an aura, Does not cause nausea and vomiting, More common in males Prevention for migraine and headaches Prevention: Beta-adrenergic blockers: (Propranolol, Atenolol) Anticonvulsants: (Valproic acid, Gabapentin) Tricyclic antidepressants: (Amitriptyline, Imipramine) Management Analgesics: Aspirin with caffeine, acetaminophen, NSAIDs: ibuprofen, naproxen, Opioid analgesics: Meperidine, butorphanol nasal spray, Ergot alkaloids: Dihydroergotamine mesylate, Selective serotonin1 receptor agonists: Sumatriptan, zolmitriptan