Mineralized Tissues & Decalcification: Bone Cells & Methods
advertisement

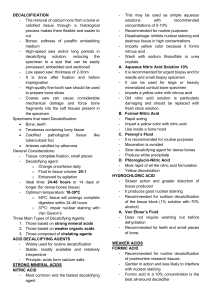
MINERALISED TISSUES AND DECALCIFICATION DR. MASHUD AHMED BONE CELLS • There are three types of active bone cells exclusive of the marrow cells which belong to the haemopoietic system. They include: • Osteoblasts • Osteocytes • Osteoclasts Osteoblasts: • They are immature bone cells but fully differentiated to carry out bone duties. • They are seen at the surfaces of actively forming bones • Contain RNA, glycogen and acid phosphatases which decreases on the onset of calcification. • On completion of the bone-forming activity most osteoblasts revert to undifferentiated cells and rest among the other cell populations. Osteocytes • Trapped osteoblasts within the forming bone turn to mature into mature bone cells (osteocytes). • they rest in small spaces within the bone known as lacunae. Osteoclasts • These are large multinucleated giant cells whose cytoplasm contains numerous mitochondria. • They are seen on bone surfaces that are undergoing erosion or resorption. • One osteoclast is capable of destroying as much bone as 100-1000 osteoblasts can lay within a period. • Osteoclasts are often referred to as bone destroyers. MINERALISATION OF BONE • In the initial stages of mineralisation, calcium is deposited in the form of amorphous calcium phosphate which is then transformed into hydroxyapatite crystals [Ca10(PO4)6(OH)2] by the addition of hydroxyl ions. • Subsequently by inclusion and substitution, carbonate, citrate and fluoride ions as well as magnesium, potassium and strotium may be introduced Pathological forms of calcium depositions Abnormal deposits of calcium can be found under the following conditions: • Necrotic tissue (tuberculosis and dead tissue worms). • Infarction (Gandy-Gamma bodies) • Artheroma in blood vessels • Malakoplakia of the bladder (Michaeli’s Gutman bodies) • Heterotropic calcification in the kidneys (hypercalcinosis) The most common forms of calcium salts found in these abnormal conditions are phosphates and carbonates. INTRODUCTION- 1 • There are a number of options available when the histologist is required to produce sections from bone or other calcified specimens. • In choosing a technique and processing method consideration must be given to the type of investigation required. • For example if a metabolic bone disease is being investigated then it is necessary to differentiate mineralized bone from osteoid (decalcify) INTRODUCTION- 2 • On the other hand if morphometric measurements are required, it may be necessary to retain and demonstrate the mineral content by producing sections of “un-decalcified” bone. • In these cases after fixation the bone can be directly sawn thin and then grounded using abrasive surfaces to produce thin “ground” sections (Figure 1). • Or infiltrate them with acrylic or epoxy resins (Fig 2) Figure 1: An unstained ground section of compact bone. A number of osteons are cut transversely. The osteons consist of concentric layers of bone Osteocytes appear as black structures due to particles of abrasive and air contained within them Figure 2: An un-decalcified section of bone (Von Kossa). The bone was fixed in formalin and processed and embedded in epoxy resin for sectioning. Note that despite the support of polymerized resin, in this case the calcified matrix has cracked during preparation of the section DECALCIFICATION • In suspected tumours or infections it is usually possible to select material with very little mineralization which will be adequate to provide a diagnosis. • These pieces can be processed or subjected to decalcification before sectioning • This can be done by treating the tissue with reagents which react with calcium to make them soluble. CHOICE OF A DECALCIFYING REAGENT This is influenced by several factors: • The urgency of the investigation. • The degree of mineralization. • The scope of the investigation. • The subsequent staining procedure which may be required. DECALCIFYING AGENTS. There are two major types of decalcifying agents which include: • Acids: which forms soluble calcium salts • Chelating agents: take up calcium ions. ACID DECALCIFIERS Are divided into two groups: • Strong acids • Weak acids. STRONG ACIDS • Strong acids include nitric and hydrochloric acids. • They are used as simple aqueous solution of 510%. • They decalcify rapidly but if they are used for longer than 48 hours they cause serious deterioration to the stainability of the decalcified tissue. • Strong acid decalcifiers should only be used for urgent biopsies with little mineralization where decalcification can be complete within a shot period. • They are not suitable for heavily mineralized bone. WEAK ACIDS • Weak acids include formic, acetic and picric acids. • Among them formic acid is the only weak acid extensively used as decalcifier. • Acetic and picric acids are included in some compound fixatives (Carnoy’s, Heidenhain’s “SUSA” and Bouins’). FORMIC ACID • Formic acid is used at 5-10% aqueous solution or with additive such as formalin to fix the bone while it is being decalcified. • Addition of fixatives in decalcifying solutions however increases the time for decalcification. • Formic acid is good for non urgent biopsies and decalcification can take 1-10 days. CHELATING AGENTS-1 • The chelating agent widely employed is EDTA in the form of its disodium salt. • Although regarded as an acid, it does not act like mineral or organic acid but captures the metallic ions (notably calcium). • As it can only bind ionized calcium it can only act on the outer layer of the apatite crystal. • As this layer becomes depleted, it is reformed by ions from within. Thus the crystal becomes progressively smaller as decalcification proceeds. CHELATING AGENTS- 2 • This is a slow process but has little or no effect on other tissue components. • Even some enzymes are still active after decalcification in EDTA. • EDTA is used as a simple solution of up to 14% or with formalin or buffered. In any case decalcification can take as long as 6-8 weeks. FACTORS INFLUENCING THE RATE OF DECALCIFICATION Several factors that can influence the rate of decalcification include: • Concentration of active reagent • Temperature • Agitation • Suspension • Ion exchange resins COMPLETION OF DECALCIFICATION • Tissues should be removed from decalcifying solutions immediately the last traces of mineral have been removed. • This will require constant surveillance • It is acceptable to test for completion of decalcification and renew the fluid at the same time. TESTS FOR COMPLETION/ END POINT OF DECALCIFICATION • The choice of test depends on the decalcifying agent and the equipment available. • The two most reliable types of test: chemical and radiological can be supplemented by physical methods. PHYSICAL METHODS • • • • • • • • Needling Probing Cutting Trimming Palpating Bending Squeezing None of these methods is satisfactory even though exploratory CALCIUM OXALATE TEST 1. Strong ammonia oxalate solution is added to used decalcifying solution drop by drop. • If a precipitate (calcium oxalate) forms, it means that there is a considerable amount of calcium present in the solution. • It is extremely unlikely that there will be no calcium in the next solution. • If there is no precipitate then saturated ammonium oxalate is added and if the solution remains clear after 30 minutes then, it is safe to assume that decalcification is complete. Calcium OXALATE TEST 1 Strong ammonia solution is added to the used decalcifying solution drop by drop 3 It also means that there will be calcium in the tissue and next solution. 2 4 If a precipitate (calcium oxalate) forms, then there is lots of calcium present in the solution. If there is no precipitate then, saturated ammonium oxalate is added and if the solution remains clear after 30 minutes then, decalcification is complete. CARBON DIOXIDE TEST • During treatment of calcified tissues with acid decalcifiers, CO2 is released and form a layer of bubbles on the surface of the tissue. • This will disperse after shaking and reform with fresh decalcification. • The absence of the bubbles means that there is no more decalcification. • Conclusion: The solution has been spent or decalcification is complete RADIOGRAPHY The most efficient test for the detection of calcium in tissue is radiography. PROCEDURE: 1. Remove the tissues from the decal. Solution. 2. Drain excess solution on tissue paper. 3. Place tissues on the envelope containing the X-ray film 4. If many tissues are involved, place radio-opaque labels (a. b, c… or 1, 2, 3….) by each tissue for ID. 5. Transfer (4) to x-ray chamber and expose 6. Put the tissues back in their containers and send the film for development. 7. Check for calcified areas against light. 1 2 3 4 5 6 7 8 WHEN TO TEST FOR END DECALCIFICATION • When using a weak acid decalcifier it is convenient to test daily, • When using EDTA, weekly tests are sufficient • When using strong acids, the first and often the only test can be conducted when it is estimated that decalcification is complete. A transverse section from a long bone optimally decalcified using formic acid (H&E). Numerous osteons with peripheral cement lines are shown A decalcified section of cancellous bone (pink) and hyaline cartilage (blue) from the epiphysis of a long bone (H&E). The delicate trabeculae of the bone are well preserved as is the fine structure of the bone marrow and associated adipocytes.