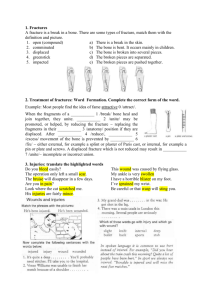
Musculoskeletal system (20100 - 29999) Anatomy Procedures • Manipulation = reduction : returning a fracture or dislocation to it’s normal anatomical position by manually applied forces. • Stabilization = fixation = immbolization. • Sprain = twisting : involves the non contractile tissue (the ligament). • Strain =stretching :involves the contractile tissue (mucle or tendon). • Arthrocentesis :aspiration of fluid from a joint using needle puncture. • Trigger points :points or areas where stimulation by touch,pain or pressure induce a painfull response. • Replantation :after a complete amputation. • Repair :after partial amputation. Fractures Types of fracture Fractures • Def: traumatic or pathological breaking of bone or cartilage • Types of fractures : • • • • Comminuted Fracture—The bone is crushed or splintered into several pieces. Impacted Fracture—One part of a bone is forcefully driven into another. Simple Fracture—The bone is in only one place. Greenstick Fracture—The bone is broken on one surface and bent on the other (think of the way a "green" twig will break when bent too far); this fracture occurs in children before the bones have hardened. • Pathologic Fracture—Caused by disease, such as an infection or a tumor. • Compression Fracture—The bone is compressed onto another bone; caused by trauma or osteoporosis, and common in vertebrae. Treatment of fractures Closed treatment specifically means that the fracture site is not surgically opened (exposed to the external environment and directly visualized). This terminology is used to describe procedures that treat fractures by three methods: (1) without manipulation; (2) with manipulation; or (3) with or without traction. Open treatment is used when the fractured bone is either: (1) surgically opened (exposed to the external environment) and the fracture (bone ends) visualized and internal fixation may be used; or (2) the fractured bone is opened remote from the fracture site in order to insert an intramedullary nail across the fracture site (the fracture site is not opened and visualized). Percutaneous skeletal fixation describes fracture treatment which is neither open nor closed. In this procedure, the fracture fragments are not visualized, but fixation (eg, pins) is placed across the fracture site, usually under X-ray imaging guidance Guideline The type of fracture (eg, open, compound, closed) does not have any coding correlation with the type of treatment (eg, closed, open, or percutaneous) provided A 22-year-old female sustained a dislocation of the right elbow with a medial epicondyle fracture while on vacation. The patient was placed under general anesthesia, and the elbow was reduced and was stable. The medial elbow was held in the appropriate position and was reduced into an acceptable position and elevated to treat non surgically. A long arm splint was applied. The patient is referred to an orthopedist when she returns to her home state in a few days. What is/are the correct CPT@ code(s) reported? A) 24575-54-RT, 24615-54-51-RT B) 24576-54-RT, 24620-54-51-RT C) 24577-54-RT, 24600-54-51-RT D) 24565-54-RT, 24605-54-51-RT • Answer is D Excision Excision of subcutaneous soft connective tissue tumors (including simple or intermediate repair) involves the simple or marginal resection of tumors confined to subcutaneous tissue below the skin but above the deep fascia. These tumors are usually benign and are resected without removing a significant amount of surrounding normal tissue. Code selection is based on the location and size of the tumor. Code selection is determined by measuring the greatest diameter of the tumor plus that margin required for complete excision of the tumor. The margins refer to the most narrow margin required to adequately excise the tumor, based on the physician’s judgment. The measurement of the tumor plus margin is made at the time of the excision. Appreciable vessel exploration and/or neuroplasty should be reported separately. Extensive undermining or other techniques to close a defect created by skin excision may require a complex repair which should be reported separately Excision Excision of fascial or subfascial soft tissue tumors (including simple or intermediate repair) involves the resection of tumors confined to the tissue within or below the deep fascia, but not involving the bone. These tumors are usually benign, are often intramuscular, and are resected without removing a significant amount of surrounding normal tissue. Code selection is based on size and location of the tumor. Code selection is determined by measuring the greatest diameter of the tumor plus that margin required for complete excision of the tumor. The margins refer to the most narrow margin required to adequately excise the tumor, based on individual judgment. The measurement of the tumor plus margin is made at the time of the excision. Appreciable vessel exploration and/or neuroplasty should be reported separately. Extensive undermining or other techniques to close a defect created by skin excision may require a complex repair which should be reported separately. Excision Radical resection of soft connective tissue tumors (including simple or intermediate repair) involves the resection of the tumor with wide margins of normal tissue. Appreciable vessel exploration and/or neuroplasty repair or reconstruction (eg, adjacent tissue transfer[s], flap[s]) should be reported separately. Extensive undermining or other techniques to close a defect created by skin excision may require a complex repair which should be reported separately. Dissection or elevation of tissue planes to permit resection of the tumor is included in the excision. Although these tumors may be confined to a specific layer (eg, subcutaneous, subfascial), radical resection may involve removal of tissue from one or more layers. Radical resection of soft tissue tumors is most commonly used for malignant connective tissue tumors or very aggressive benign connective tissue tumors. Example • A 19-year-old male college student bumped his right thigh while playing intramural rugby on the lawn of the Cathedral of Learning. He sustained a lump and bruise. and the pain was so intense he had to be taken to ED for treatment. The ED physician was uncertain and concerned about the lump on the patent's thigh so he asked the dermatologist on call to diagnose the suspicious lump. The dermatologist diagnosed the patient with a 2.5 cm benign tumor of the right thigh. and recommend that he follow up with his dermatologist for treatment. Two weeks later, the patient arrives to the dermatologist for excision of the benign tumor. The patient was prepped, draped. and anesthetized appropriately. The physician makes an incision over the tumor through the skin, subcutaneous tissue, and muscle. The tumor was visualized then removed. The site was flushed with saline. Hemostasis was achieved with electrocautery. The site was closed with sutures in layers. Which procedure code(S) best describe this encounter? • A. 11404 • B. 27328. 12031-51 • C. 11404, 12031-51 • D. 27328 • ANSWER IS D Wound exploration 20100-20103 relate to wound(s) resulting from penetrating trauma These codes describe surgical exploration and enlargement of the wound, extension of dissection (to determine penetration), debridement, removal of foreign body(s), ligation or coagulation of minor subcutaneous and/or muscular blood vessel(s), of the subcutaneous tissue, muscle fascia, and/or muscle, not requiring thoracotomy or laparotomy. If a repair is done to major structure(s) or major blood vessel(s) requiring thoracotomy or laparotomy, then those specific code(s) would supersede the use of codes 2010020103. To report simple, intermediate, or complex repair of wound(s) that do not require enlargement of the wound, extension of dissection, etc, as stated above, use specific Repair code(s) in the Integumentary System section . • ANSWER IS A Introduction /removal • Introduction or removal includes codes for injections, foreign body removal, and placement of catheters for radioelement application. Surgical injections involve direct insertion of a needle into a tendon, muscle, or joint for the aspiration of fluid or the administration of medication. When coding injections, watch for bundled procedures. For example, trigger point injections (20552—20553) are selected based on the number of muscles injected. not the number of injections performed. • Testing Technique • Highlight the number of muscles in the code descriptions for 20552 and 20553. Write a note that states “Select code according to number muscles, not the number of injections”. • An arthrocentesis of a joint include aspiration of fluid or the injection of an anesthetic agent or steroid. • The codes are selected based on the size of the joint and with or without ultrasound guidance. When a joint aspiration and injection are performed on the same joint. only report the procedure once- If the procedures are performed on more than one joint, list each procedure separately . • Injection of a substance does not include the drug itself. the drug supply may be billed separately using a HCPCS Level II code. • Example: • The provider 3 cc of fluid from the left knee. He injects 40 mg of Kenalog into the right knee. The knee • is a major joint. The proper codes are 20610-LT and 20610-RT for the procedures. The Kenalog is reported with HCPCS Level II code J3301 with four units because the code is for 10 mg. Example • A 39-year-old involved in a motor vehicle accident (MVA) a year ago arrives to the pain clinic with complaints of neck pain and left-sided radiculopathy complicated by cervical degenerative disc disease. NSAIDs and physical therapy have been unsuccessful, and the patient requires multiple trigger point injections. The left multifidus , trapezius, and right levator scapular were injected. The area was cleansed and bandage applied. Which procedure code(s) best describe this encounter? • A. 20552 • B. 20553 • C. 20610 • D. 20553x3 • Answer is B Spinal surgery often requires the skills of more than one surgeon. When these surgeons work together as surgeons performing a portion of the same procedure, modifier 62 should be appended to report the service. Each surgeon dictates an operative report for his or her portion of the surgery, and each surgeon reports the same code with modifier 62. Arthrodesis Arthrodesis is the surgical immobilization of a joint, which is intended to result in bone fusion. This procedure is often documented in the operative note as a fusion. A physician may implant pins, plates, screws, wires, or rods to position the together until they fuse. Bone grafts may be needed if there is significant bone Joss. When selecting codes for spinal arthrodesis, you need to know the approach (anterior, posterior, posterolateral, or lateral transverse). You also need to know the vertebral segment (cervical, thoracic, or lumbar). Disarticulation is the separation of two bones at the joint, either traumatically or by surgical amputation. Spinal instrumentation • Spinal instrumentation codes are add-on codes; they are to be coded in addition to the primary surgery (eg, arthrodesis 22800—22812). Add-on insertion codes 22840—22848 are not to be reported with reinsertion code 22849 or removal code 22850. Add-on insertion codes are reported when new hardware is put in for the first time or when new hardware is put in which exceeds the previously placed hardware and includes removal of the old hardware. • Reinsertion (22849) is reported when the hardware is going back in the same spinal levels as • the previous placed hardware and includes the removal of the old hardware. • Removal codes (22850, 22852, and 22855) are reported when only the hardware is taken out. Grafts • Grafts (or implant) codes are used when obtaining bone, cartilage, tendon or fascia Iata grafts, or other tissue. An autograft is a graft of tissue or bone harvested from the patient. In coding orthopedic surgery, an autograft can be bone, cartilage, muscle or tendon. If the material being grafted is from a donor, it is known as an allograft. Bone grafting to stabilize the spine is common. Codes 20930—20938 report the grafting procedures, are add-on codes listed separately in addition to the code for the primary procedure. • Testing Technique • If the procedure code description includes the harvesting of the graft, do not report the graft code separately. Add a notation in this section to indicate graft is only reported If not included in the procedure note description. For example, 21194 includes obtaining the graft. 21193 Reconstruction of mandibular rami, horizontal, vertical, C, or L osteotomy; without bone graft 21194 with bone graft (includes obtaining graft) Example Within the spine section, bone grafting procedures are reported separately and in addition to arthrodesis. For bone grafts in other Musculoskeletal sections, see specific code(s) descriptor(s) and/or accompanying guidelines. To report bone grafts performed after arthrodesis, see 2093020938. Do not append modifier 62 to bone graft codes 2090020938. Example: Posterior arthrodesis of L5-S1 for degenerative disc disease utilizing morselized autogenous iliac bone graft harvested through a separate fascial incision. Report as 22612 and 20937. Example Within the spine section, instrumentation is reported separately and in addition to arthrodesis. To report instrumentation procedures performed with definitive vertebral procedure(s), see 22840-22855, 22859. Instrumentation procedure codes 22840-22848, 22853, 22854, 22859 are reported in addition to the definitive procedure(s). Modifier 62 may not be appended to the definitive or add-on spinal instrumentation procedure code(s) 22840-22848, 22850, 22852, 22853, 22854, 22859. Example: Posterior arthrodesis of L4-S1, utilizing morselized autogenous iliac bone graft harvested through separate fascial incision, and pedicle screw fixation. Report as 22612, 22614, 22842, and 20937. Example Vertebral procedures are sometimes followed by arthrodesis and in addition may include bone grafts and instrumentation. When arthrodesis is performed in addition to another procedure, the arthrodesis should be reported in addition to the original procedure with modifier 51 (multiple procedures). Examples are after osteotomy, fracture care, vertebral corpectomy, and laminectomy. Bone grafts and instrumentation are never performed without arthrodesis. Example: Treatment of a burst fracture of L2 by corpectomy followed by arthrodesis of L1-L3, utilizing anterior instrumentation L1-L3 and structural allograft. Report as 63090, 22558-51, 22585, 22845, and 20931 The surgeon performs the spine procedure for an anterior thoracic two-level arthrodesis, anterior single level discectomy, anterior plate instrumentation, and structural, autograft iliac crest bone graft. What code(s) would be reported? A) 63077, 22556-51, 22845, 20938 B) 63077, 22556, 22585, 22845,20930 C) 63077, 22556-51, 22585, 22845, 20938 D) 63077, 22610, 22556, 22845-51, 20938-51 Example • A 37-year-old male with a history of neck pain and radiculopathy with failed physical therapy. CT, MRI, and Myelogram all confirm C6-C7 spondylosis and right disc protrusion. The patient will have to have his disc removed. The patient is prepped and draped in sterile fashion. After administration of anesthesia, a transverse incision is made anteriorly. The muscles are excised for access to the target disc. The disc between C6-C7 is identified and removed. The posterior longitudinal ligament was removed to provide access to excise the osteophytes, and decompression is achieved. The disc space was prepared utilizing a burr drill, homogenous structural bone grafting was inserted. and segmented instrumentation with endplates were applied anteriorly to achieve arthrodesis. • A. 63075, 22551-51, 22845, 20931 • B. 22551, 22840, 20930 • C. 22551, 22845, 20931 • D. 63075, 22551-51, 22840, 20930 • Answer is c Cast / strapping • When a physician reports a treatment of a fracture and then applies a cast or strapping, the cast or strapping is included in the procedure. A physician may code for a cast or strapping when the cast or strapping is the only treatment given at the first visit and no surgical treatment is planned. Each replacement cast or strapping can be reported. • Modifier 58 is reported with a cast or strapping procedure performed in the postoperative period. The removal of a cast or strapping is not reported separately unless the service is provided by a physician who did not apply the cast CPT modifiers CPT modifiers Example • Answer is c Example • ANSWER IS A Example • Answer is c Example • Answer is d