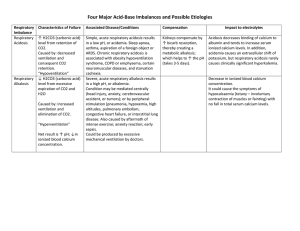
A. Mark K- Acid & Base + Ventilators Rule of the B’s If the pH and the Bicarb are in the same direction, then it is metabolic If the pH and Bicarb are in opposite directions, then it is respiratory pH under 7.35 is acidosis pH above 7.45 is alkalosis pH- 7.35-7.45 HCO3- 22-26 CO2- 35-45 O2-80-100 Ex, 7.25 bicarb 20 (both are down/same direction)- metabolic acidosis Ex, 7.48, bicarb 29 (both up)- metabolic alkalosis Ex, 7.30 bicarb 29 (opposite)- respiratory acidosis Ex, 7.50, bicarb 25 (opposite) (the pH is high, and the bicarb is normal. High and normal are not the same direction, so the rule still works) = respiratory alkalosis - boards don’t do mixed acid/base SIGNS AND SYMPTOMS - they will tell you the patient has respiratory/metabolic/acidosis/alkalosis and ask you what would you see, select all that apply? As the pH goes up so goes my patient except for K o As the pH goes up the patient becomes for restless and agitated/ hyper excited o As the pH goes down the patient shuts down As the pH goes up (alkalosis) the patients goes up Signs you would see are o Irritability o Hyper reflexes- +3, +4 o Tachypnea o Tachycardia o Borborygmi (increased bowel sounds) o Seizure As the pH goes down (acidosis) the patient goes down Signs you would see are o Hypo reflexes o Paralytic ileus o Bradycardia o Lethargy (obtundunt) o Coma Alkalosis you are more likely to seize because when the pH is high you are high People with alkalosis disorders need suction machines at the bed side because they could seize and aspirate Acidosis more likely to have respiratory arrest because when the pH is down you are down People with acidosis disorders need an ambo bag at the bed side Kussmaul Respirations (deep and rapid) - You only see this with metabolic acidosis none of the other ones Ex, pt has respiratory acidosis SATA a) +1 reflexes b) diarrhea c) a dynamic ileus d) spasm e) urinary retention f) paroxysmal g) atrial tachycardia h) type 2 heart block i) hypokalemia CAUSES of acid/base imbalances - they will give you a scenario and be like this is what is happening to your patient, what acid/base disorder is this? DON’T GET CONFUSED WITH SIGNS/SYMPTOMS AND CAUSES- SOME TIMES IT IS OPPOSITE Couple questions you want to ask yourself when they give you a scenario 1. Is it a lung issue? = respiratory problem 2. How do you figure out if it is acidosis/alkalosis for respiratory? a. Is the client over ventilating or under ventilating? i. OVER ventilating(hyperventilating)= alkalosis (think it is OVER the normal range to be alkalosis) ii. UNDER ventilating (hypoventilating)= Acidosis (think UNDER the normal range to be acidosis) Ex, you have a patient that was drowning, are they over or under ventilating? – Under Ex, pt has emphysema what is it?- Under Ex, pt has pneumonia in 4 lobes, breathing really fast at 50/min, and 02 is 70%- Under Ex, pt is on a PCA pump (depress respirations) what acid/base imbalance would make you think they need to come off of it? Respiratory acidosis The respiratory rate is irrelevant for the over/under questions Ventilation is not about the RR rate it is about the gas exchange happening in the lungs (oxygen saturation) 3. What is the issue isn’t a lung issue? = metabolic problem 4. Acidosis/alkalosis for metabolic If the patient has prolonged gastric vomiting or suctioning pick metabolic alkalosis Ex, patient hooked up to suction Patient is morning sickness cause pregnant For everything else that isn’t lung, or vomiting/suction pick metabolic acidosis Patient with morning sickness that is now dehydrated- the main problem isn’t vomiting now it’s dehydration Patient with diarrhea 3rd degree burns over 60% of the body when you don’t know what it is pick metabolic acidosis Ventilation - need to know the different alarm meanings - high pressure alarm is trigged with increased resistance to air flow o in other words, the machine is having to push too hard to get the air into the lungs and when that happens the machine will set off a high pressure alarm this could happen for three reasons (3 obstructions) 1. kinks in the tubing- so unkink the tubing 2. water condensing within the dependent loop- empty the water out 3. mucus secretions in the airway- get them to change positionsturn/cough/deep breath, if that doesn’t work pre oxygenate them and then suction Suctioning airways how often do you suction patients? o only as necessary. So that means you only do it after you have moved them/turned/coughed/deep breath and that didn’t mobilize the secretions o if 02 is low, and high pressure alarm is going off get the patient to turn, and cough before suctioning them THIS IS THE ORDER YOU DO IT WHEN HIGH PRESSURE ALARM GOES OFF 1. check for kinks 2. empty water out of tubing 3. turn/cough/deep breath 4. suction Low pressure alarms the machine is saying it is to easy to push the air into the patients lungs this can happen for two reasons- disconnections 1. Disconnections of the main tubing- reconnect to fix problem 2. Disconnections of the oxygen sensor tubing- it measures the Fi02 and oxygen. So you need to plug the sensor back in High pressure alarms are commonly due to- obstructions Low pressure alarms are commonly due to- disconnections Respiratory alkalosis means the ventilator settings might be to HIGH This is when the patient is over ventilating- ventilator is to high Respiratory acidosis means the ventilator settings might be to LOW This is when the patient is under ventilating- ventilator is to low Ex, doctor says wean off vent in am tomorrow. The 6am ABG show respiratory acidosis, what would you do a) Follow the order b) Call respiratory therapy c) Hold the order call doctor d) Begin to decrease the settings - Call doctor because he is under ventilating, therefore he needs the ventilator so we can’t take him off The acid/base disorder we did want to see at 6am is respiratory alkalosis where he is over ventilating so he can come off the vent #2