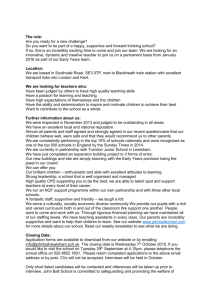
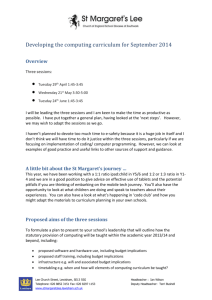
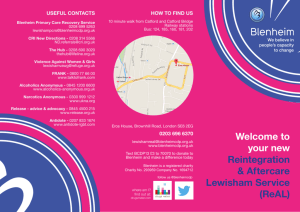
Page:of 17 8 Skin Cancer Skin serv ices have been peer reviewed and Trusts and the network are producing action plans to ensure compliance with the IOG and to meet peer review requirements. Brain and Central Nervous System The National Cancer Action have tasked each MDT to update MDT activi ty and workforce against the IOG for submission by the February 2010 S upportive and Palliative Car e A final Stock take is currently being undert aken for submission to NCAT by March 2010. The Cancer Action Team along with an SHA lead will be visiting networ ks in 2010 to offer further support. The Network along with the majority of other networks will be red lighted on psychological care and rehabilitation where further work and investment is still needed. 3. What is this telling us? L ocal V iews The South East London Cancer Network model for user partnership was established in 2005 . A revised South East London Cancer Network (SELCN) user partnership strategy (2008 2012) has been developed building on the work of the previous strategy. The overall aim of this strategy is to embed user partnership working and user involvement in policy development, service planning and service delivery of high quality, user centered cancer services in SELCN. In addition to this overarching framework there is current activ e user involvement in many but not all of the tumour working groups, supportive care groups and generic working groups. Users are also involved in one off projects, focus groups and in peer review. NHS Lewisham has been recently recognized by the DH and NHS London for the wo rk carried out through the Pace setters programme, working with local women from Black and minority ethnic communities to promote attenda n ce for breast screening. The Healthy Communities Collaborative Cancer Project works with a team of lay volunteers to organise and facilitate cancer awareness workshops, presentations, festival or group meetings ,w hich attract a diverse population in terms of age and ethnicity. Interim results from a Cancer Awareness Survey carried out in a neighbou ring borough in South East London with a similar population profile to Lewisham found that there was: Low knowledge of “persistent cough and hoarseness” and “sore that does not heal” as warning signs of cancer Knowledge of warning signs for cancer lower among non white and economically inactive people Low knowledge of HPV, low intake of fruit and vegetables and low physical activity as risk factors for cancer Underestimation of personal risk of cancer Low knowledge of frequency of bowel cancer Low knowle dge of frequency of lung cancer in women Low knowledge of existence of bowel screening programme 9 Lower knowledge of existence of NHS screening programmes in people who are non white, economically inactive and living in poorer areas. Also particularly low f or the Black African subgroup. National and Local Strategies The Cancer Reform Strategy , published in 2007, builds on the progress made since the publication of Cancer Plan (2000) and strives to close the gap in cancer outcomes between the UK and the r est of Western Europe. The key aims are to : Prevent cancer by tackling the lifestyle factors that increase the risk of developing the disease . Diagnose cancer earlier by increasing coverage of cancer screening and increasing awareness of cancer symptoms . Ensure that patients have access to high quality cancer care . Support and empowering patients through their ‘cancer journey’ Reduce inequalities in cancer incidence, mortality and access to care . Bring cancer care closer to home where appropriate . Healthc are for London: A Framework for Action was published in July 2007. Led by Professor Lord Darzi it made a compelling case for change in health and healthcare services across London. To support the implementation of this policy in cancer services a “Case for Change” was published in March 2010 which provided a set of arguments for the need to improve cancer services in London. This has been followed by the publication of a Model of C are for London cancer services. The South E ast London Cancer N etwork has de vel oped its strategic vision covering all aspects of cancer services prevention, screening, diagnosis, treatment ( s urgery, radiotherap y and systemic therap y) and suppo rtive palliative care which has been published is Collaborative Commissioning Initiative s 2008 09 to 2010 0 13. NHS Lewisham’s Commissioning Strategy Plan (2009 2015) “Improving Health and Well being” has Reducing Premature Mortality from Cancer as one of its seven strategic goals. Current Activity and S ervices Primary P revention Preven tion remains the best form of tackling cancer, reducing the human suffering caused by the disease and improving outcomes. There is also a strong economic case for investing more in prevention, therefore reducing the pressure on services in the long term. Reducing smoking prevalence Smoking is the single largest preventable risk factor for cancer. The key actions of the Lewisham Tobacco Control P lan are: Reducing availability to children vending machines/ supply of tobacco to minors 10 Reducing attractiven ess of tobacco products removal of display/ reducing promotion/ limiting exposure to tobacco use in media/ reducing promot ion through tobacco accessories Taking action on illicit toba cco Counterfeit Tobacco Seizures NHS intervention Stop Smoking services Smoking and Pregnancy. Healthier nutrition / increasing physical activity The evidence linking poor diet and obesity to cancer has become much stronger. In Lewisham there is a Prom oting Health Wei ght for Lewisham Children, Young People and their F amilies Strategy and an action plan . The action plan includes the following: Promotion of Healthy Weight for all children, including measuring of children in R and year 6, linking with scho ols nurses, Maternity, Early years, schools (linking with Healthy Schools) Leisure Sports and Environment including the promotion of free swimming, and the adoption of Change for Life to promot e local activities and projects , the development of a Physica l Activity Strategy and action plan in 2010. Lewisham Food Strategy, which includes improving food access through the development of Food Co ops, food growing through Community gardens and allotments , Schools Food Policy and Schools meals Workforce train ing and communications Development of target ed and specialist weight management services for children a nd adults . Alcohol Excessive alcohol consumption is strongly linked to an incre ased risk of several cancers. Lewisham has published an Alcohol Strategy 2009 2012. The strategy aim s to promote sensible drinking and to reduce the impact of alcohol misuse . Priorities for the coming year include the revision and development of the Council and PCT’s workplace alcohol polices, to run seasonal campaigns, to c ontinue and develop the primary care based Directed and Local Enhanced Services and to develop an alcohol prevention pathway as part of the Health Checks programme. Skin Campaign The skin campaign was launched in April 2009 and ran until September 2009 across the six boroughs covered by the South East London Cancer Network. The campaign used innovative evidence based social marketing techniques to produce measured behaviour change amongst residents, who are most at risk of skin cancer. Three ‘behavioura l’ groups were targeted using a range of communication channels including a bespoke website, nightclub posters and on the ground engagement, supplemented with an education programme. The budget for the research and campaign implementation was jointly fun ded by the South East London Cancer Network (SELCN) and six PCTs. The results showed that 22% of South East London residents had remembered seeing the campaign, and of those who had seen it 36% said they had taken action as a result, including checking the ir skin more often and using higher level sun protection. 11 Human Papilloma Virus (HPV) vaccination for cervical cancer Vaccination now presents a further opportunity in cancer prevention, specifically for cervical cancer. The government has introduced a n ational vaccination programme for young girls against the human papillomavirus. This will protect against the strains of the virus which cause around seven out of ten cases of cervical cancer. In the academic year 2008 09 Lewisham achieved an uptake of 72. 6%, lower than the national target of 80%. Increasing awareness and earlier presentation Healthy Communities Collaborative Cancer project A two year community based cancer ini tiative was launched i n Lewisham September 2008 and completed in September 2010 The Healthy Communities Collabor ative aimed to raise awareness and promote the earlier presentation of cancer symptoms. The project was focusing on three wards in Lewisham that have high deprivation with , high mortality and poor survival rates for cancer . These are Evelyn , New Cross and Bellingham and it included working with fourteen general practices in these wards. The focus was on breast, bowel and lung cancer. Earlier diagnosis Increasing the coverage/uptake of cancer screening A key objective for NHS Lewisham and partners in reducing health inequalities is to improve cervical , breast and bowel screening uptake. Central to this is the involvement of primary care to promote screening. A specification for cancer screening and primary care is bei ng developed. Health Equity Audits are currently being carried out on the breast and cervical screening progrmammes to assess issues of access. Cervical cancer screening Uptake rates for cervical screening will be analyzed by practice and poor perfor ming practices will be targeted with support and best practice shared. Breast Screening A breast screening action plan has been developed and submitted to the London S trategic H ealth A uthority . Key actions to implement this include ,v alidation of pract ice lists, supporting and involving primary care to promote breast cancer screening and aw a ren e ss r a ising and health promotion activities to women in the community. Bowel cancer A health promotion specialist has been appointed in South East London by t he Bowel Cancer Screening Programme to promote bowel cancer screening, to work closely with Primary Care Services and to develop strategies to increase the uptake rate . Southwark PCT has developed a ‘bowel screening action pack’ to raise awareness of the p rogramme among GP practices which will be promoted in Lewisham . Training and health promotion sessions have been and will continue to be carried out for health and social care professionals and a wide rang e of community and voluntary groups in Lewisham. An application for NAEDI funding for South E ast London sector to develop an integrated programme of awareness raising of bowel cancer symptoms and the screening programme was submitted at end of April 2010 and was successful. A campaign to raise 12 awareness of bowel cancer signs and symptoms in the members of the community most at risk and in selected GPs practices is being planned for summer of 2011. Secondary and tertiary care services NHS Lewisham commissions for its patients access to a comprehensive range of diagnostic and treatment services for cancer, including tertiary care, primarily provided in the SELCN area . SELCN Strategic Commissioning Priorities for 2009 2013 Bring cancer mortality in line with National target of 20 % reduction over 10 year s. Increase levels of awareness of cancer and causes . Improve continuously towards meeting National Targets and increase coverage. Breast 70% Minimum 80% Target. Cervical 80 % . Reduce Delays in reporting cervical cancer to 2 weeks. Implement Bow el Cancer Screening programme including age extension. Undertake National Audit in Primary Care for all newly diagnosed patients with cancer. Implement National Chemotherapy and Radiotherapy Guidance to improve access to treatment . Reduce inpatient be d days for cancer patients and increase ambulatory care. Reconfigure services in South London Healthcare, UHL and AHSC to deliver safe services locally where possible and centralise where necessary. Establish clear arrangements for the commissioning and provision of NICE approved drugs. Transform the Cancer Network management into clearly focused support for commissioning. . What is this telling us? What are the key inequalities? There is now a range of evidence about the nature and extent of inequalities which occur in cancer, including: Cancer incidence and mortality are generally higher in deprived groups compared with affluent groups, older compared with younger people and men compared with w omen. Conversely, breast cancer has higher incidence in more affluent groups, but mortality is actually higher in less affluent women. The picture for ethnic minority groups varies according to cancer type and ethnic group. In general, incidence is lower a mongst ethnic minority groups, although there are some important exceptions (incidence of prostate cancer is greater amongst Black African and Black African Caribbean men, liver cancer in South Asians, and mouth cancer in Bangladeshis); Levels of public aw areness of cancer signs and symptoms are generally low, but even lower in some groups, such as deprived communities, some BME groups and men. This may contribute to lower uptake of screening and later presentation when symptoms arise; Lifestyle factors (s uch as smoking, obesity, alcohol consumption and physical inactivity) almost certainly account for most of the variance in cancer incidence between the most and least deprived; Poorer experience of care is reported by black and minority ethnic groups, men with prostate cancer, and people living in London; Part of the variance in mortality rates can be attributed to delayed diagnosis amongst deprived groups, older people (at least for breast cancer) and certain 13 BME groups (at least for breast cancer). The co ntribution of delayed diagnosis to poorer survival rates and higher mortality amongst men th an women is still uncertain; Improvements in mortality have been slower in older people than in younger people. Older people with cancer receive less intensive tre atment than younger people. In many cases this may be clinically appropriate. However, there is increasing evidence that under treatment of older people may occur. Cancer mortality is the third major contributor for both men and women to the gap in life e xpectancy between Lewisham and England. Circulatory disease fo llowed by respiratory disease are the first and second contributors respectively. In 2006 08 c ancer mortality accounted for 19% of the gap in male life expectancy in Lewisham compared to England and 13% of the gap in female life expectancy in Lewisham compared to England. In Lewisham lung cancer deaths for both men and women is the major contributor to the “cancer” gap. Table 8: Causes of death from cancer and their contribution to the gap in life expectancy between Lewisham and England 2006 08 Men Women Oesophageal cancer 4.4% 2.3 % Stomach cancer 2.2 % 1.5% Colorectal cancer .. 0.5 % Lung cancer 8.3 % 8.2 % Breast cancer .. .. Other cancers 4.5% .. Source:http://www.lho.org.uk Age spec ific Death Rates from Cancer The following tables and charts show age specific death rates per 100,000 people for males and females separately, during the period 2005 7, for Lewisham, with comparative data for England, London overall, and the ONS London Co smopolitan comparator group 1 . The charts use a logarithmic scale for ease of readability. Figure 2: Age specific death rates per 100,000 , cancer, Males 2005 7 Age Specific Death Rates 2005-7, Cancer, Males 1 10 100 1000 10000 1-4 5-14 15-34 35-64 65-74 75+ age-band Deaths/100,000 males ENGLAND LONDON LONDON COSMOPOLITAN Lewisham LB Source: NCHOD 1 Source: NCHOD Compendium of Public Health Indicators 14 Figure 3: Age specific death rates, cancer, Females 2005 7 Age Specific Death Rates 2005-7, Cancer, Females 1 10 100 1000 10000 1-4 5-14 15-34 35-64 65-74 75+ age-band Deaths/100,000 females ENGLAND LONDON LONDON COSMOPOLITAN Lewisham LB Source: LHO The f ollowing observations can be made: Lewisham’s cancer death rate for pre school age boys is around three times as high as the England and London rates. This may be a statistical “blip”, as absolute numbers (which are not included in the source data) are v ery small. Lewisham’s rates in school age children are low for both sexes (again, absolute values will be low). Lewisham death rates from cancer in younger working age people of both sexes are less than half the national rates. Lewisham’s cancer death rate s in older working age people of both sexes are below national rates, and closely comparable to the other comparators. In males aged 65 74, Lewisham’s cancer death rates are 29% higher than England’s. In males aged over 75 and over, Lewisham’s death rate f rom cancer are 6% higher than the national rate. In females age 65 74, Lewisham’s death rate from cancer is 12% higher than England’s. In females aged 75 and over, Lewisham’s death rate from cancer is 3% higher than the national rate. Deprivation There a re significant inequalities in cancer mortality within Lewisham. Bellingham and New Cross wards have the highest mortality rates for 2003 07. These wards are the second and fourth most deprived in the Borough respectively. 15 Figure 4: Standardised Mortalit y Ratios for Cancer, Lewisham Wards, Aged <75, 2003 2007 Mortality from all cancers: persons, less than 75 years, indirectly standardised ratios (SMR, 100 = England) with 95% confidence intervals by ward, 5 year average, 2003-07 50 70 90 110 130 150 170 190 210 230 Bellingham Blackheath Brockley Catford South Crofton Park Downham Evelyn Forest Hill Grove Park Ladywell Lee Green Lewisham Central New Cross Perry Vale Rushey Green Sydenham Telegraph Hill Whitefoot SMR (100 = England) Source: LHO What are the key gaps in knowledge/services? Further detailed information analysis to understand the excess cancer mortality in older people in Lewisham compared to England. Further detailed analysis to understand 1 – year survival for colon cancer. Roll out the learning from the HCC cancer project across Lewisham practices. Effective interventions to increase uptake of screening services and awareness of symptoms and signs of canc er in the population as a whole and in specific population groups . The need to increase the scale of primary prevention interventions to reducing smoking prevalence, the promotion of healthy eating and physical activity, promote sensible drinking and to sustain the skin campaign. What are the risks of not delivering our targets? The primary target for cancer is a minimum 20% reduction in cancer mortality by 2010 from the 1995/97 rate and that fewer people will die prematurely from cancer, heart disease and stroke before the age of 75. Thus the risks of not delivering in other areas, such as smoking and physical activity and diet obesity, will have an impact on cancer outcomes. In particular, Smoking prevalence remains higher than the national average – reflecting Lewisham’s socioeconomic landscape; The socioeconomic and ethnic diversity of Lewisham population impacts on late presentation of cancer and uptake of screening programmes. Innovati ve social 16 marketing combined with community engagement approaches are required otherwise this will impact on early diagnosis; Is what we are doing working? Deaths from cancer are affected by a wide range of factors including all aspects of cancer care; prevention, screening, diagnosis, and treatment. Considerab le progress has been made both nationally and locally. There has been a decline in cancer mortality both nationally and locally , nationally cancer survival rates for breast, colon, rectum and pro s t ate cancer has improved since 2000. The HPV vaccination programme has been implemented. The bowel cancer screening programme has been rolled out . Lewisham NHS successfully complied with the original waiting standards and is making good progress with th e extended waiting time standards. What is coming on the horizon? Greater demand from health services related to cancer due to Improved detection through screening programmes, which will increase screening activity and the proportion of cancers requ iring active, curative and intensive treatment. Increased demand for adjuvant therapy Improved survival rates will lead to increased workload in monitoring and treatment of recurrence Increased demand for emotional support. Greater focus on Awareness and early diagnosis requiring the development of skills and knowledge in primary care. Shift in the focus of care from a hospital setting to a community based setting where appropriate . The implementation of the Healthcare for London “Case for change” and the Cancer model of care. What should we be doing next? Increase the scale of primary prevention interventions to reducing smoking prevalence, the promotion of healthy eating and physical activity, promote sensible drinking and to sustain the skin campaig n. Role out the learning from the Health Community Collaborative Cancer Project across Lewisham. There is a need to have a greater focus on raising awareness and early diagnosis across GP practices in Lewisham. This will require support and training in pr imary care. Consider what are the most effective interventions to promote awareness of cancer symptoms and the benefits of screening to the diverse populations in Lewisham. Negotiate and implement a Cancer screening specification in primary care to incre ase the uptake of cancer screening programmes. Spread best practice in cervical screening across all practices in Lewisham to reduce variability in coverage. 17 Further analysis to understand excess cancer mortality in older age population compared to Engl and and the 1 year colon cancer survival rates.