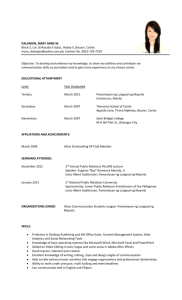
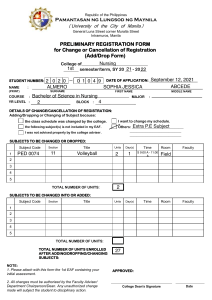
PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA DRUGS FOR LOWER RESPIRATORY DISORDERS LOWER RESPIRATORY SYTEM Lower Respiratory (Trachea, bronchi, bronchioles, alveoli, and alveolar-capillary membrane)Gas exchange Gas-exchange airways- composed of acinus (bronchi, bronchioles, alveoli) o Any problem in tissues interfere with oxygenation. Any distensible organ has compliance. LUNG COMPLIANCE/ EXPANSIBILITY/ DISTENSIBILITY Lung compliance (Expand)- lung volume based on the unit of the pressure in the alveoli o Lung volume is determined by lung’s ability to stretch o Ability of your lungs to expand o Opposite of surface tension (collapse) o Opposite to elasticity (recoil) o Directly proportional to lung volume and inversely proportional to the pressure Factors that affect the lung compliance: o Connective tissues (collagen and elastin) o Surface tension in the alveoli High lung compliance for those who have COPD; Low lung compliance for restrictive diseases 2 Major Categories of Lower Respiratory Tract Disorder o COPD- caused by airway obstruction with increased airway resistance of airflow to lung tissues because it has stretched so much Emphysema, chronic bronchitis, bronchiectasis, frequent and chronic asthma causes irreversible tissue lung damage CAL (Chronic Airflow Limitation)- Emphysema, chronic bronchitis, bronchiectasis, and asthma o 1|Page Restrictive Pulmonary Disease- decrease of total lung capacity due to fluid accumulation or loss of elasticity of the lungs Pulmonary edema Pulmonary fibrosis Pneumonitis Lung tumors Thoracic deformities (i.e., scoliosis) Disorders affecting thoracic muscular wall such as myasthenia gravis PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA COPD (i.e., Emphysema) Restrictive disorders (Cystic Fibrosis) Lung expand Compliance Expansibility Lung Collapse Recoil Elasticity (either or loss) Distensibility Surfactant Elastase Emphysema I can get the air in but I cannot get the air out. Elastic recoil Surface tension Elastin Fibrosis I cannot get the air in but I can get the air out. Obstructed from exhaling Restricted from filling CHRONIC OBSTUCTIVE PULMONARY DISORDER Cigarette smoking accounts as the common risk factor for COPD. According to World Health Organization, Chronic Obstructive Pulmonary Disease (COPD) is the third leading cause of death worldwide, causing 3.23 million deaths in 2019. And, over 80% of these deaths occurred in low- and middle-income countries. Asthma- either reversible or irreversible depending on the case; it occurs in two ways; o Inflammation- it obstructs lumen in the inside o Airway hyperresponsiveness that leads to bronchoconstriction Chronic bronchitis o Progressive lung disease caused by smoking or lung infection o Inflammation and excessive mucous secretion o When alveolar sac is damaged, this may lead to hypercapnia and hypoxemia that will eventually become respiratory acidosis if not treated o Rhonchi may be heard Bronchiectasis o Abnormal dilation of the bronchi and bronchioles secondary to frequent infection and inflammation Emphysema o Progressive lung disease caused by Atmospheric contaminants Cigarette smoking Lack of alpha1-antitrypsin- it inhibits the proteolytic enzymes (released by the bacteria pr phagocytic cells) that causes destruction of the alveoli. When the terminal bronchioles were plugged with mucus it decreases the fibers and elastin which is used for the recoil. Alveolar just expands along with other alveoli until it become destroyed. The overexpanded alveoli have trapped air that causes inadequate gas exchange. 2|Page PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA Bronchodilator drugs Sympathomimetics agents or adrenoreceptor agents Methylxanthines Leukotriene antagonists Glucocorticoids Cromolyn Anticholinergic Mucolytics SYMPATHOMIMETIC DRUGS Sympathomimetics agents or adrenoreceptor agents are best delivered by inhalation because it causes greatest local effect on airway smooth muscle with least systemic toxicity. Drugs that mimic actions of epinephrine and norepinephrine o Different modes; DIRECT INDIRECT Epinephrine Actions are dependent to the release of endogenous catecholamines Norepinephrine Both causes activation of adrenoreceptors o Two principal receptors Alpha Beta Smooth muscle contraction Smooth muscle relaxation Alpha Beta Alpha 1 Alpha 2 Equal affinity Equal affinity for epinephrine epinephrine norepinephrine and norepinephrine Indirect mode, two mechanisms Beta 1 Beta 2 for Equal affinity for Higher affinity for epinephrine and epinephrine and and norepinephrine norepinephrine Displacement of stored catecholamines from the adrenergic nerve ending Amphetamine and tyramine o Inhibition reuptake of catecholamines already released Cocaine and Tricyclic antidepressants Relaxes airway smooth muscle and inhibits the release of broncho constricting mediators from mast cells Prevents mast cell degranulation Inhibit microvascular leakage and increase mucociliary transport by increasing ciliary activity Beta agonists stimulate the adenylyl cyclase that increases intracellular cAMP that induces bronchodilation 3|Page PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA Directly relax airway smooth muscle When beta2 receptors stimulated, relaxation of airway smooth muscles, inhibition of mediator release, tachycardia and skeletal tremor may follow as its side effects It includes o Epinephrine o Ephedrine o Isoproterenol o Albuterol o Beta2-selective agents Isoproterenol Isoetharine Metaproterenol Terbutaline Albuterol (salbutamol) Salmeterol Epinephrine and isoproterenol cause increase of rate and force in cardiac contraction (B1 receptors) and they are reserved for special situations DRUGS INCLUDED Epinephrine o Effective and rapidly acting bronchodilator o Injected or inhaled as a micro aerosol from a pressurized cannister. o Bronchodilation achieved after 15 minutes and lasts for 60-90 minutes o Stimulates Alpha and Beta1 and 2 receptors o Administered during emergency situations to restore circulation and increase the patency of airway o Adverse effects Tachycardia Arrhythmia Worsening angina pectoris o used in treating the acute vasodilation, shock, bronchospasms of anaphylaxis Ephedrine o It has a longer duration compared to epinephrine o Lower potency Isopterenol o Potent bronchodilator o It effects after 5 minutes when inhaled as a micro aerosol from a pressurized canister and lasts for 60-90 minutes. o Adverse effect is cardiac arrythmias that is why it is now rarely used in asthma Beta2 Selective Drugs 4|Page PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA Contains larger substitution on the amino group and in the position amino group and in the position of the hydroxyl groups on the aromatic ring o Albuterol o Terbutaline o Metaproterenol o Pirbuterol metered-dose inhalers Bronchodilation is achieved 15-30 minutes and lasts 3-4 hours Albuterol and terbutaline are available in tablet form. The PO administration has no advantage over the inhaled treatment of its effect only terbutaline is available in subcutaneous injection (0.25mg) Salmeterol and formoterol- new generations of long-acting B2 selective agonists; both drugs are potent and have longer duration of 12 hours due to its high lipid solubility; interacts with inhaled corticosteroids to improve asthma control; Not recommended as the sole therapy PROTOTYPE DRUG: METAPROTERENOL Some beta1 agent are affected but primarily used as beta2 agent. PO or Inhalation Drug class Pharmacokinetics Pharmacodynamics Bronchodilator A: PO; absorbed PO Adrenergic beta2 and some beta1 well Onset: 15-30 mins D: Unknown Peak: 1h Therapeutic effects The drug treats bronchospasm, asthma; Promotes bronchodilation Dosage Contraindication Interactions A/C: >9 y: PO: 20 mg q6-8h Hypersensitivity Cardiac dysrhythmias Narrow-angle glaucoma Cardiac disease Hypertension Increased action with other sympathomimetic drugs Decrease action with beta blockers Decreased sodium potassium Older adults 10 mg q6-8h M: Unknown Alupent Duration: 4h E: Urine Category C C: 6-9 y; 10 mg q6-8h SubQ Onset: 1-5 mins Peak: 1h Duration: 3-4 hrs 5|Page A/C: >12y: MDI 2-3 inhal as single dose; wait 2 mins before second dose, if necessary; use only q3-4h to max: 12 inhal/d Side effects Nervousness Tremors Restlessness Insomnia Headache Nausea Vomiting Hyperglycemia Muscle cramping in extremities Adverse Reactions Tachycardia Palpitation hypertension Cardiac dysrhythmias Cardiac arrest Paradoxical bronchoconstriction PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA Mechanism of Action: Relaxation of smooth muscle of bronchi due to increase of cAMP Nursing Considerations: Assess lung sounds, pulse, and blood pressure before administration and during peak of medication; observe patient for wheezing after administration, if this occurs, call physician; monitor heart rate, respiratory rate, blood pressure, and arterial or capillary blood gases if applicable Do not use solutions for nebulization if they are brown or contain a precipitate; before using, the inhaler must be shaken well PARASYMPATHOLYTICS DRUGS Anticholinergics Also known as muscarinic antagonists blocks muscarinic actions, thus, causing inhibition of muscarinic functions. Muscarinic Receptors These receptors are activated by the ligand acetylcholine Differs in function as ionotropic ligand-gated and G-protein coupled receptors Functions within both the central and peripheral nervous system, as well as the neuromuscular junction. Muscarinic Receptor Location Effect M1, M4, M5 Primarily found in the cerebral cortex, gastric, and salivary glands Affects cognitive process as well as dry mouth M2 Located in the smooth muscle and cardiac tissues Increases heart rate 6|Page Blocked SA and AV nodes affects heart rate (may lead to tachyarrhythmia) PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA M3 Also present in the smooth muscles, GI Tract Gastric motility, Prolonged gastric emptying, and lengthen intestinal transit time. Urinary tract Decrease in bladder contraction Airway Bronchodilation Decrease bronchial secretions Eye Mydriasis- narrowing of the iridocorneal angle Impaired accommodation (abnormalities of the pupil) Blood Pressure minimal effect on vascular tone and BP. Exocrine glands (gastric, and salivary glands) 7|Page Decreases secretions. PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA fig. 1.1, fig. 1.2 Figures 1.1 and 1.2 illustrate how the drug takes effect in producing bronchodilation in our smooth muscles. For the figure 1.1, it indicates a picture of the axon terminals (nerve ending) connected to our smooth muscles. Normally, these axon terminals produce acetylcholine (ACh) that then attaches/binds to our sodium-ion channels. The binding of the ACh and the ligand-gated channels, shown in figure 1.2, results in its opening allowing sodium ions to pass through triggering a muscular action potential. This action potential caused by the sodium ions first travels through the surface of the sarcolemma. After the sarcolemma, it travels along the T Tubules that penetrate in the fiber allowing the release of calcium from the sarcoplasmic reticulum that results in muscle constriction. 8|Page PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA Action Potential > Release of ACh > ACh binding > Sodium ion passess through > Triggers Action Potential > Penetrate the fiber > Release of Calcium ions > Muscle Constriction How does the “Anti” work? First, is the Nondepolarizing Agents ● Basically, these nondepolarizing agents replace the function of the Ach. ○ So, it binds to the receptors but does not induce ion channel opening. ○ As a result, it inhibits sodium ions to enter that essentially leads to an effective prevention for muscle contraction ● These agents are not absorbed very well in the GI tract (IV route is essential) Second, is the Depolarizing Agents ● ACh antagonist that mimics the action of the ACh ○ first, the depolarizing agents attach to the channels that allows sodium to pass through the channel ○ But these agents are acetylcholinesterase inhibitors. In short, they block the sodium-ion channels or the muscarinic receptors. ANTICHOLINERGIC DRUGS Chemical characteristics Drug Quaternary ammonium Ipratropium derivatives (hydrophilic, poor bioavailability and CNS penetration) Brand names: - Atrovent - Combivent - Ipravent Dosage Bronchodilator for COPD: Short-acting muscarinic antagonist. (SAMA) via Inhalation: 2 inhalations 4 times/day Used for treating COPD is required. If necessary, grade 1 and higher 12 inhalations per day would be the maximum. Acute management for asthma exacerbations and refraction Nebulization: 500mg 3-4 times a day. Doses should have a 6-8 9|Page Indication PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA hours gap in between. Asthma Exacerbation via Inhalation: 8 inhalations q20min for up to 3 hours is needed. Nebulization: 500mg q20min for 3 doses Rhinorrhea (Perennial Allergy) via Intranasal: 2 sprays per nostril 2-3 times/day Rhinorrhea (Common Allergy) via Intranasal: 2 sprays per nostril 2-3 times/day for up to 4 days Rhinorrhea (Seasonal Allergy) via Intranasal: 2 sprays per nostril 2-3 times/day for up to 3 weeks Tiotropium 10 | P a g e COPD (maintenance treatment) Longer acting muscarinic antagonists PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA Brand name: - Spiriva Handihalers, Respimat - Stiolto via Inhalation: (LAMAs) 18mcg (1 capsule)/day via HandiHaler device (Spiriva). While 2 inhalations of 2.5 mg once daily is required for Spiriva Respimat Long-term treatment for COPD (grade 2 and above) Inspiolto Respimat Asthma via Inhalation: 2 inhalations of 1.25 mcg once daily. Maximum benefit may take 4-8 weeks of continuous inhalation of Spiriva Respimat. Aclidinium Brand name: - Tudorza Pressair inhalation powder (400 mcg/inh) For maintenance treatment of COPD: ● ● Umeclidinium 11 | P a g e Adults—One puff 2 times a day, in the morning and evening, about 12 hours apart. Each puff contains 400 micrograms (mcg) of aclidinium bromide. Children—Use and dose must be determined by your doctor. inhalation powder (62.5 mcg (0.0625 mg)/inh) PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA Brand name: For maintenance treatment of COPD: - Incruse Ellipta ● ● Adults—One inhalation once a day. Do not take more than one inhalation every 24 hours. Children—Use is not recommended. PROTOTYPE DRUG: IPRATROPIUM DRUG CLASS BRAND NAME/S DOSAGE ● ● Pharmacotherapeutic - Anticholinergics Clinical - Bronchodilator ● ● Atrovent Combivent Respimat (albuterol/ipratropium combination) Bronchodilator for COPD: via Inhalation: 2 inhalations 4 times/day is required. If necessary, 12 inhalations per day would be the maximum. Nebulization: 500mg 3-4 times a day. Doses should have a 6-8 hours gap in between. Asthma Exacerbation via Inhalation: 8 inhalations q20min for up to 3 hours is needed. Nebulization: 12 | P a g e PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA 500mg q20min for 3 doses Rhinorrhea (Perennial Allergy) via Intranasal: 2 sprays per nostril 2-3 times/day Rhinorrhea (Common Allergy) via Intranasal: 2 sprays per nostril 2-3 times/day for up to 4 days Rhinorrhea (Seasonal Allergy) via Intranasal: 2 sprays per nostril 2-3 times/day for up to 3 weeks INDICATIONS ● ● ● ● CONTRAINDICATIO NS & CAUTIONS ● ● ● 13 | P a g e Therapeutic actions are bronchodilation Indication for this drug is that anticholinergics like the ipratropium and tiotropium are used for treating asthma exacerbations, COPD, rhinorrhea, and sialorrhea. That also provides prevention of nausea, vomiting, and dizziness from motion sickness. - Children are more sensitive to its adverse effects; while - Adults should be cautioned about the adverse effects from this drug. Also, pregnant women are not allowed to take these type of drug as it can penetrate through the placenta making the fetus susceptible to any adverse effects. Susceptibility to adverse effects also takes place in different age groups. Hence, adjustment in dosage is needed to prevent the side effects. For the contraindication and cautions in using or taking anticholinergic drugs; First, we must be knowledgeable if we are ALLERGIC to any components of the drug. Second, these drugs are contraindicated in patients with glaucoma, especially angle-closure glaucoma PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA ● ● Third, because these drugs are slow gastric emptying, they may increase symptoms of patients with gastric ulcers. Nonselective antimuscarinic agents should NEVER be used to treat patients with acid-peptic disease, Fourth, pregnant women are prohibited in taking these meds as its components goes in the breast milk. PHARMACOKINETIC S Route Onset Peak Duration Inhalation 1-3 minutes 1.5-2 hours Up to 4 hours Nasal 5 minutes 1-4 hours 4-8 hours ● ● ● ● ● ● MECHANISM OF ACTIONS Absorption: minimal systemic absorption after inhalation due to lack of absorption potential in the mucosal surfaces. Volume of Distribution: Highly distributed in the tissues with 4.6 L/kg Protein Binding: Low Metabolism: Systemic absorption=Metabolised in the liver Elimination: urine elimination of the drug says that it remains unchanged; if orally administered, it is primarily excreted in feces. Half Life: 1.5-4 hours (Nasal) “ I can’t S-S-P-P” I can’t SEE I can’t SPIT I can’t PEE I can’t POOP ADVERSE EFFECTS “ABCDs.” A- agitation B- blurred vision C- constipation 14 | P a g e PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA D- dry mouth S- stasis of urine and sweating. Side effects includes the “ABCDs” and: drowsiness sedation hallucinations memory problems nausea headache DRUG TO DRUG INTERACTIONS ● ● ● Antihistamines, antiparkinsonisms, MAOIs, TCAs have cholinergic effects so the incidence of anticholinergic effects increases. Phenothiazines, a psychotic drug, decreases the effectiveness of the anticholinergic effect of the drug. Burdock, rosemary, and turmeric Nursing Considerations Check inhaler technique Assess the presence of contraindications and cautions above to avoid adverse effects. o Auscultate lung sounds Question history of glaucoma, urinary retention, myasthenia gravis Establish physical assessment to monitor for potential risk susceptibility for adverse effect. Monitor laboratory test results to determine any considerations like dosage adjustment for preventing potential toxicity. Monitor rate, depth, rhythm, type of respiration Quality rate of pulse Patient education, teaching Advise patients not to exceed the prescribed dose. Rinse mouth after each use of the inhaler. Frequent drinks and the use of sugar-free gum can help with dry mouth. Seek medical attention if more than the usual dosage is required. Keep delivery devices clean and dry. Take a missed dose as soon as remembered unless it is almost time for the next dose. Do not take a double dose. 15 | P a g e PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA Avoid getting in the eyes. METHYLXANTHINES Methylxanthines are derived from purine base xanthine. That is produced by both plants and animals. These are alkaloids that can be found in high concentrations in tea, coffee, and chocolate. Theophylline, theobromine, and caffeine are the most popular. They can be found in different concentrations in coffee, chocolate, and tea. Mechanism of Action When Beta-2 receptor is being activated, activation of GS coupled protein (receptors) makes our adenylyl cyclase (AC). These AC are the one that converts the ATP into cyclic adenosine monophosphate or the cAMP. Why is cAMP important? decreases release of inflammatory mediators decreases bronchial secretions causes relaxation in smooth muscles ~ bronchodilation 16 | P a g e PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA Normally, cAMP is converted into AMP (adenosine monophosphate) due to the presence of the enzyme called phosphodiesterase (PDE). So, what the methylxanthine does is it inhibits the PDE that causes its degradation, resulting in more/ increasing levels of cAMP that leads to bronchodilation. ADDITIONAL INFO OR GENERATION OF DRUG PROTORYPE DRUG: THEOPHYLLINE DRUG CLASS BRAND NAME/S DOSAGE ● ● Pharmacotherapeutic - Methylxanthine Clinical - Bronchodilator, COPD exacerbation ● ● ● Elixophyllin Uniphyl Theo-24 Intravenous (IV): ● ● for patients with acute bronchospasm 5-7 mg/kg intravenously, followed by a maintenance dose of 0.40.6 mg/kg per hour to maintain serum concentrations at 10-15 mg/L Oral (PO): ● Should be taken consistently with or without food ○ ○ INDICATIONS ● ● 17 | P a g e The 12-hour formulation (twice daily) ■ initiated at the end of every 12-hour dosing The 24-hour formulation (once daily) ■ Taking each morning at a strictly same time frame and avoiding taing at night. ■ Patients that require a higher dose should take the medication less than an hour before a high-fat meal. Therapeutic action - Slightly relax the airways in the lungs ( bronchodilator ). - Improve breathing by increasing the strength of the diaphragm (if it is weakened) and by stimulating the breathing control centers in the brain. - Make it easier to get mucus out of the lungs. Indication PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA - CONTRAINDICATIO NS & CAUTIONS ● ● Treats symptoms and reversible airflow obstruction. Inhibition of proinflammatory mediators Deceleration of fibrotic changes in the lung Relaxation of the bronchial musculature results to bronchodilation Damaged cardiac muscle (e.g., following myocardial infarction) Significant risk of drug interactions (e.g., ciprofloxacin, cimetidine) PHARMACOKINETIC S Route Onset Peak Duration Oral 1-3 minutes 1.5-2 hours N/A IV 15 minutes 15-30 minutes N/A ● ● ● ● ● ● Absorption: rapid and complete absorption after oral administration. Volume of Distribution: 0.3 to 0.7L/kg Protein Binding:40%, primarily to albumin Metabolism: metabolized in the liver and levels are sensitive to stimulation or inhibition of the P450 enzyme system and levels are increased by many drugs such as cimetidine, corticosteroids, macrolide and quinolone antibiotics, and interferon. Elimination: does not undergo any appreciable presystemic elimination, distributes freely into fat-free tissues and is extensively metabolized in the liver. Half Life: ○ 8 hours in adults; ○ 4-5 hours in smokers MECHANISM OF ACTIONS ADVERSE EFFECTS 18 | P a g e ● ● ● ● ● ● ● ● nausea/vomiting, stomach/abdominal pain, headache, trouble sleeping, diarrhea, irritability, restlessness, nervousness, PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA DRUG TO DRUG INTERACTIONS ● ● shaking; or increased urination ● Riociguat (a drug that treats pulmonary hypertension) may react with theophylline. Cigarette/mariuana smoking decreases blood levels of this medication. Caffeine and alcohol intake can increase the medication’s side effects. Do not take medications containing aminophylline or oxtriphylline while using theophylline This medication may interfere with certain lab tests possibly causing false test results. ● ● ● ● Nursing Considerations Theophylline has a low therapeutic index. ● Dosage is determined by monitoring response, tolerance, pulmonary function, and serum theophylline levels. Target range is 10 to 20 mcg/ml. ● Use cautiously in young children, infants, neonates, and elderly patients. ● Depending on assay used, theophylline levels may be falsely elevated in the presence of furosemide, phenylbutazone, probenecid, theobromine, caffeine, tea, chocolate, cola beverages, and acetaminophen. Falsely elevated serum uric acid as measured by the Bittner or calorimetric method. ● Monitor vital signs and watch for signs and symptoms of toxicity. ● Obtain serum theophylline measurements in patients receiving long-term therapy. Ideal levels are between 10 and 20 mcg/ml, although some patients may respond adequately with lower serum levels. Check every 6 months. If levels are less than 10 mcg/ml, increase dose by about 25% each day. If levels are 20 to 25 mcg/ml, decrease dose by about 10% each day. If levels are 25 to 30 mcg/ml, skip the next dose and decrease by 25% each day. If levels are more than 30 mcg/ml, skip the next two doses and decrease by 50% each day. Repeat serum level determination. Breast-feeding patients ● Drug appears in breast milk and may cause irritability, insomnia, or fretfulness in the breast-fed infant. A decision must be made to stop either breast-feeding or drug. Pediatric patients ● Use cautiously in neonates. Children usually require higher doses (on a mg/kg basis) than adults. Maximum recommended daily doses are 24 mg/kg in children younger than age 9; 20 mg/kg in children age 9 to 12; 18 mg/kg in adolescents ages 12 to 16; 13 mg/kg or 900 mg (whichever is less) in adolescents and adults age 16 and older. Patient education ● ● Tell patients to take drugs with food if GI upset occurs with liquid preparations or non-sustainedrelease forms. Instruct patients to continue to use the same brand of theophylline. 19 | P a g e PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA ● If a patient smokes, tell him to call if he quits because theophylline dose may need to be reduced to avoid toxicity. ○ Advise patients to take drug at regular intervals as instructed, around-the-clock. ○ If a patient misses a dose, tell him to take it as soon as possible but not to double the dose. ○ Inform patients of adverse effects and possible signs of toxicity. INTRANASAL CORTICOSTEROIDS Intranasal Glucocorticoids ● ● ● Intranasal glucocorticoids or steroids are used for treatment of allergic rhinitis. Anti-inflammatory action for allergic rhinitis symptoms of rhinorrhea, sneezing, and congestion. These drugs may be used alone or in combination with an H1 antihistamine. INTRANASAL GLUCOCORTICOIDS GENERIC (BRAND) ROUTE AND DOSAGE USES AND CONSIDERATIONS beclomethasone (Beconase AQ, Qnasl) A: 1-2 puffs/sprays b.i.d budesonide (Pulmicort, Rhinocort) A/C: >6 y: 1-2 sprays b.i.d. or 4 sprays in the morning For seasonal rhinitis in adults and children. Maintenance therapy for asthma. Pregnancy category: C; PB: 90%; t 1 2 : 2.5-3 h dexamethasone (Decadron) A/C: 6-12 y: 1-2 sprays b.i.d. For allergic and inflammatory conditions. Administered orally, intravenously, ophthalmically, topically, and intranasally. A potent steroid used for short-term therapy. May have a systemic effect. Pregnancy category: C; PB: UK; t 1 2 : 23.5 h flunisolide A: 2 sprays b.i.d./t.i.d. 20 | P a g e C: 6-12 y: 1 spray b.i.d. For seasonal or perennial allergic and nonallergic rhinitis. Pregnancy category: C; PB: 87%; t 1 2 : 15 h For seasonal rhinitis in adults and children. May be used for steroid-dependent asthma. C: 6-14 y: 1 spray t.i.d. or Pregnancy category: C; PB: UK; t 1 2 : 1-2 2 sprays b.i.d. h PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA fluticasone (Flonase, A: 2 sprays once daily or Flovent) 1 spray b.i.d. C: >6 y: 1 spray/d mometasone furoate (Nasonex) A: 2 sprays once daily triamcinolone (Nasacort AQ) A/C: 1-2 sprays once daily C: 1 spray once daily For seasonal allergic rhinitis. When symptoms decrease, reduce dose to 1 spray daily. Pregnancy category: C: PB: 91%; t 1 2:8h For seasonal allergic rhinitis. Pregnancy category: C; PB: UK; t 1 2 : UK Note: Direct spray away from nasal septum; gently sniff. For allergic rhinitis. Has many uses, such as an immunosuppressant. Pregnancy category: C; PB: UK; t 1 2 : 2-5 h PROTOTYPE DRUG: BECLOMETHASONE ● ● ● ● ● ● ● ● Brand name ○ Beconase AQ ○ Qnasl Classification ○ adrenocorticosteroid ○ anti-inflammatory, immunosuppressant Mode of action ○ controls or prevents inflammation by altering rate of protein synthesis; depresses migration of polymorphonuclear leukocytes, fibroblasts; reverses capillary permeability. Therapeutic outcome ○ inhalation: inhibits bronchoconstriction, produces smooth muscle relaxation, decreases mucus secretion. ○ intranasal: decreases response to seasonal, perennial rhinitis. Uses ○ Seasonal, perennial allergic/vasomotor rhinitis, nasal polyps, chronic steroid dependent asthma Contraindications ○ Hypersensitivity, status asthmaticus (primary treatment) Precautions ○ Pregnancy C, breastfeeding, child ,12, nasal disease/surgery, nonasthmatic bronchial disease, bacterial, fungal, viral infections of mouth, throat, lungs, HPA suppression, osteoporosis, Cushing’s syndrome, diabetes mellitus, measles, cataracts, corticosteroid hypersensitivity, glaucoma, herpes infection Dosage and routes ○ Adult and child .12 yr: 21 | P a g e PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA ■ ● ● ● ● ● Oral inh 48-80 mcg bid (alone) or 40-160 mcg bid (with inhaled corticosteroids), max 320 bid ○ Child 5-12 yr.: ■ Oral inh 40 mcg bid, max 80 mcg bid ○ Available forms: ■ Inhalation, Oral: 40 mcg/inhalation, 80 mcg/inhalation. ■ Nasal Inhalation: ● (Beconase AQ): 42 mcg/inhalation. ● (QNASL): 40 mcg/actuation, 80 mcg/ actuation. Implementation ○ Oral route ■ give PO, using a spacer device for proper dose ■ shake oral aerosol well, use spacer ■ use after cleaning aerosol top daily with warm water; dry thoroughly ■ store in a cool environment; do not puncture or incinerate container ○ Nasal route ■ Shake inhaler, invert, tilt head backward, insert nozzle into nostril, away from septum; hold other nostril closed and depress activator, inhale through nose, exhale through mouth Adverse effects ○ CNS ■ Headache; psychiatric/behavioral changes (child) ○ EENT ■ Candidal infection of oral cavity, hoarseness, sore throat, dysgeusia, loss of taste/ smell ○ ENDO ■ Hypothalamic-pituitary (HPA) suppression ○ GI ■ Dry mouth, dyspepsia ○ MISC ■ Angioedema, adrenal insufficiency, facial edema, Churg-Strauss syndrome (rare) ○ RESP ■ Bronchospasm, wheezing, cough Pharmacokinetics ○ absorption: locally only ○ distribution: not distributed ○ metabolism: lungs, liver (by CYP3A) ○ excretion: feces, urine ○ half-life: 2.8 hr Pharmacodynamics ○ onset: [inh 1-4 wk] [Nasal 10 min] ○ peak: [inh unknown] [nasal unknown] ○ duration [inh unknown] [nasal unknown] Nursing Considerations ○ Assessment ■ Assess adrenal suppression: 17-KS, plasma cortisol for decreased levels, adrenal function periodically for HPA axis suppression during prolonged therapy; monitor growth and development 22 | P a g e PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA ■ ○ ○ Assess blood studies, neutrophils, decreased platelets; WBC with diff at baseline and q3mo; if neutrophils are ,1000/mm3 , discontinue treatment ■ Check nasal passages during long-term treatment for changes in mucus; check for burning, stinging; assess for glucocorticoid withdrawal: dizziness, hypotension, fatigue, muscle/joint pain; notify prescriber immediately ■ Assess respiratory status: rest, rhythm, characteristics; auscultate lung bilaterally before and throughout treatment ■ Assess for fungal infections in mucous membranes Patient/family education ■ Teach patient to gargle/rinse mouth after each use to prevent oral fungal infections ■ Teach patient that in times of stress, systemic corticosteroids may be needed to prevent adrenal insufficiency; do not discontinue oral product abruptly, taper slowly ■ Teach patient to continue using product even if mild nasal bleeding occurs; is usually transient ■ Teach patient method of administration after providing written instructions from manufacturer ■ Clean inhaler by wiping with dry cloth ■ Teach patient the symptoms of adrenal insufficiency: nausea, anorexia, fatigue, dizziness, dyspnea, weakness, joint pain, depression Evaluate ■ Positive therapeutic outcome: Decrease in runny nose, improved symptoms of bronchial asthma. · CORTICOSTEROIDS ● ● ● Glucocorticoids, members of the corticosteroid family, are used to treat respiratory disorders particularly asthma. These drugs have an anti-inflammatory action and are indicated if asthma is unresponsive to bronchodilator therapy or if the patient has an asthmatic attack while on maximum doses of theophylline or an adrenergic drug. It is thought that glucocorticoids have a synergistic effect when given with agonist. Glucocorticoids can be given using the following methods: ● MDI inhaler ● Tablet ● Intravenous ● Inhaled glucocorticoids are not helpful in treating a severe asthmatic attack, because it may take 1 to 4 weeks for an inhaled steroid to reach its full effect. ● Patients with acute asthma exacerbations are usually given systemic glucocorticoids (i.e., IV) for rapid effectiveness in large doses (20 to 40 mg prednisone for 5 days; 1 to 2 mg/kg/day for children for 3 to 5 days). 23 | P a g e PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA ● When severe asthma requires prolonged glucocorticoid therapy, weaning or tapering of the dose may be necessary to prevent an exacerbation of asthma symptoms and suppression of adrenal function. ● Side effects associated with orally inhaled glucocorticoids are generally local (e.g., throat irritation, hoarseness, dry mouth, coughing) rather than systemic. ● Oral and injectable glucocorticoids have many side effects when used long-term, but short-term use usually causes no significant side effects PROTOTYPE DRUG: BUDENOSINE DRUG CLASS ● ● Pharmacotherapeutic - Glucocorticoid Clinical - Anti-inflammatory, anti-allergy BRAND NAME ● ● Pulmicort Rhinicort Aqua DOSAGE ● Adult and pediatric (>6 y): 200–400 mcg b.i.d. (two inhalations), maximum dose 800 mcg b.i.d. INDICATIONS ● Prevention and treatment of asthma; treatment of chronic steroid-dependent bronchial asthma; used as adjunctive therapy for asthma patients who do not respond to traditional bronchodilators CONTRAINDICATIONS & CAUTIONS ● Hypersensitivity to budesonide (nebulization/inhalation) Primary treatment of status asthmaticus, acute episodes of asthma. Not for relief of acute bronchospasms. ● PHARMACOKINETICS ● These drugs are rapidly absorbed from the respiratory tract, but they take from 2 to 3 weeks to reach effective levels, and so patients must be encouraged to take them to reach and then maintain the effective levels. They are metabolized by natural systems, mostly within the liver, and are excreted in urine. PHARMACODYNAMICS ● Onset - Slow 24 | P a g e PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA ● ● ● ● MODE OF ACTION ● ● ADVERSE EFFECTS Peak - Rapid Duration - 8-12 hours Half-life - 2 to 3 hours; metabolized in the liver and excreted in urine. Decreases the inflammatory response in the airway This action will increase airflow and facilitate respiration in an airway narrowed by inflammation. Irritability, headache, rebound congestion, epistaxis, local infection. Nursing Considerations ASSESSMENT ● ● ● ● DIAGNOSIS Assess for possible contraindications or cautions: acute asthmatic attacks and allergy to the drugs, which are contraindications, and systemic infections, pregnancy, or lactation, which require cautious use. Perform a physical examination to establish baseline data for assessing the effectiveness of the drug and the occurrence of any adverse effects associated with drug therapy. Monitor blood pressure, pulse, and auscultation to evaluate cardiovascular response. Assess respirations and adventitious sounds to monitor drug effectiveness. Nursing diagnoses related to drug therapy might include the following: IMPLEMENTATION ● ● ● Risk for Injury related to immunosuppression Acute Pain related to local effects of the drug Deficient knowledge regarding drug therapy ● Do not administer the drug to treat an acute asthma attack or status asthmaticus because these drugs are not intended for treatment of acute attack and will not provide the immediate relief that is needed. Taper systemic steroids carefully during the transfer to inhaled steroids; deaths have occurred from adrenal insufficiency with sudden withdrawal. Have the patient use decongestant drops before using the ● ● 25 | P a g e PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA inhaled steroid to facilitate penetration of the drug if nasal congestion is a problem. EVALUATION ● ● ● ● Monitor patient response to the drug (improved breathing). Monitor for adverse effects (nasal irritation, fever, GI upset). Evaluate the effectiveness of the teaching plan (patient can name drug, dosage, adverse effects to watch for, specific measures to avoid them, and measures to take to increase the effectiveness of the drug). Monitor the effectiveness of other measures to ease breathing. MUCOLYTICS Increase or liquefy respiratory secretions to aid the clearing of the airways in high-risk respiratory patients who are coughing up thick, tenacious secretions. Patients may be suffering from conditions such as chronic obstructive pulmonary disease (COPD), cystic fibrosis, pneumonia, or tuberculosis. PROTOTYPE DRUG: ACETYLCYSTEINE DRUG CLASS ● ● Pharmacotherapeutic - Respiratory inhalant Clinical - Mucolytic BRAND NAME ● ● N-acetylcysteine Mucomyst DOSAGE ● PO: ADULTS, ELDERLY, CHILDREN - Loading dose of 140 mg/kg, followed in 4 hrs by maintenance dose of 70 mg/kg q4h for 17 additional doses (or until acetaminophen assay reveals nontoxic level). Repeat dose if emesis occurs within 1 hr of administration. IV: ADULTS, ELDERLY, CHILDREN - Consists of 3 doses. Total Dose: 300 mg/kg.) 150 mg/kg infused ● 26 | P a g e PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA over 60 min, then 50 mg/kg infused over 4 hrs, then 100 mg/kg infused over 16 hrs INDICATIONS ● Mucolytic adjunctive therapy for abnormal, viscid, or inspissated mucous secretions in acute and chronic bronchopulmonary disorders; to lessen hepatic injury in cases of acetaminophen toxicity. CONTRAINDICATIONS & CAUTIONS ● Caution should be used in cases of acute bronchospasm, peptic ulcer, and esophageal varices because the increased secretions could aggravate the problem. There are no data on the effects of the drugs in pregnancy or lactation. PHARMACOKINETICS ● The medication may be administered by nebulization or by direct instillation into the trachea via an endotracheal tube or tracheostomy. Acetylcysteine is metabolized in the liver and excreted somewhat in urine. It is not known whether it crosses the placenta or enters breast milk. ● PHARMACODYNAMICS Instillation Inhilation ● ● ● Onset - 1 min Peak - 5-10 min Duration - 2-3 hours Oral ● ● ● ● - 27 | P a g e Onset - 30-60 min Peak - 1-2 hours Duration - Unknown Half-life 2 to 3 hours; metabolized in the liver and excreted in urine. PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA MODE OF ACTION ● Splits links in the mucoproteins contained in the respiratory mucus secretions, decreasing the viscosity of the secretions; protects liver cells from acetaminophen effects. ADVERSE EFFECTS ● Adverse effects most commonly associated with mucolytic drugs include GI upset, stomatitis, rhinorrhea, bronchospasm, and occasionally a rash. Nursing Considerations ASSESSMENT ● ● ● ● ● DIAGNOSIS Assess for possible contraindications or cautions: any history of allergy to the drugs and the presence of acute bronchospasm, which are contraindications to the use of these drugs; and peptic ulcer and esophageal varices, which would require careful monitoring and cautious use. Perform a physical examination to establish baseline data for assessing the effectiveness of the drug and the occurrence of any adverse effects associated with drug therapy. Assess skin color and lesions to monitor for adverse reactions. Monitor blood pressure and pulse to evaluate cardiac response to drug treatment. Evaluate respirations and adventitious sounds to monitor drug effectiveness. Nursing diagnoses related to drug therapy might include the following: ● ● ● ● IMPLEMENTATION ● ● ● 28 | P a g e Acute Pain related to GI, CNS, or skin effects of the drug Disturbed Sensory Perception (Kinesthetic) related to CNS effects Ineffective Airway Clearance related to bronchospasm Deficient Knowledge regarding drug therapy Avoid combining with other drugs in the nebulizer to avoid the formation of precipitates and potential loss of effectiveness of either drug. Dilute concentrate with sterile water for injection if buildup becomes a problem that could impede drug delivery. Note that patients receiving acetylcysteine by face mask should have the residue wiped off the facemask and off their face with plain water to prevent skin breakdown. PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA EVALUATION ● ● ● ● Monitor patient response to the drug (improvement of respiratory symptoms, loosening of secretions). Monitor for adverse effects (CNS effects, skin rash, bronchospasm, GI upset). Evaluate the effectiveness of the teaching plan (patient can name drug, dosage, adverse effects to watch for, specific measures to avoid them, and measures to take to increase the effectiveness of the drug). Monitor the effectiveness of comfort and safety measures and compliance with the regimen. ANTIHISMATICS DRUGS LEUKOTRIENE RECEPTOR ANTAGONISTS AND SYNTHESIS INHIBITORS Leukotrienes ● The eicosanoid family includes a group of inflammatory mediators known as leukotrienes (LTs). ● Antigens, immune complexes, complement, cytokines, osmotic challenges, and pollutants are among the immunologic and nonimmunologic stimuli that stimulate their production, which is largely carried out by leukocytes. These substances work together to promote the inflammatory cascade by altering vascular permeability, affecting leukocytes, and constricting smooth muscle. ● Most notably, the bronchoconstriction caused by leukotriene activity plays an important part in the pathophysiology of asthma, which opens the door to the use of targeted pharmacotherapy to treat asthma and comparable disorders. ● Leukotrienes are largely synthesized in leukocytes. Different leukocytes generate mostly leukotriene B (LTB) or the cysteinyl class of leukotrienes. Neutrophils are the principal producers of LTB and only a little quantity of cysteinyl leukotrienes. The cysteinyl leukotrienes are mostly produced by eosinophils, basophils, and mast cells. They have a negligible capability for LTB production. Macrophages and monocytes act as intermediaries because they are sufficiently capable of producing both LTB and cysteinyl leukotrienes. ● cysLT1 is involved in airway changes including bronchoconstriction, edema, and mucus formation. cysLT2 causes increased vascular permeability and tissue fibrosis, but has no effect on the airways. 29 | P a g e PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA ● As stated, Leukotrienes are crucial in asthma because they promote inflammation, bronchoconstriction, and mucus development. LTC 4, LTD 4, and LTE 4 are the most potent bronchoconstrictors in humans. ● Leukotrienes have the potential to draw white blood cells to the lungs, causing thickening and swelling of the lining of the lung. They also have the additional effect of increasing mucus formation and making it easier for fluids to collect (an important part of inflammation). ● Due to its severe bronchoconstrictive impact (which is at least 200 times greater than histamine), LTD4 is considered to be the most significant cysteinyl leukotriene in the pathophysiology of asthma. This is due to the fact that LTD4 causes the muscles around the airways to tighten. 30 | P a g e PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA Figure 1. Overview of the leukotriene pathway demonstrating the key enzymes encoded by genes with variants associated with asthma, aspirin-exacerbated respiratory disease (AERD), or the pharmacologic response to leukotriene modifier therapy. Red boxes demonstrate known genetic associations. BLT, Leukotriene B; PG, pharmacogenetic association; CysLT, cysteinyl leukotriene. Modified with permission from N Engl J Med. 1999;340:197-206. Retrieved from https://pubmed.ncbi.nlm.nih.gov/19665766/ 31 | P a g e PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA Leukotriene Receptor Antagonists and Synthesis Inhibitors ● also called leukotriene modifiers ● These medications are beneficial in decreasing the inflammatory symptoms of asthma brought on by allergy and environmental triggers. ● utilized for exercise-induced asthma but not approved for use in the treatment of acute asthmatic attacks 32 | P a g e PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY Leukotriene Receptor Antagonists PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA zafirlukast (Accolate) Pharmacotherapeutic: Leukotriene receptor antagonist; Bronchodilator Clinical: Antiasthma Trade name: Accolate Pregnancy Category: B Drug Classification Mode of Action montelukast (Singulair) Pharmacotherapeutic: Leukotriene receptor inhibitor; Bronchodilator Clinical: Antiasthma Trade name: Singulair Pregnancy Category: B Selective and competitive receptor antagonist of leukotriene D4 and E4 (LTD4 and LTE4), components of slowreacting substance of anaphylaxis (SRSA). Selective receptor antagonist of leukotriene D4, thus inhibiting bronchoconstriction. Binds with leukotriene receptors to inhibit smooth muscle contraction and bronchoconstriction Therapeutic Effects helps to prevent the signs and symptoms of asthma o airway edema, o smooth muscle constriction, and o altered cellular activity due to inflammation Controls asthmatic attacks by inhibiting leukotriene release as well as inflammatory action associated with the attack. Uses and Indications Prophylaxis and chronic treatment of asthma in adults and children >5 y (not for acute bronchospasm). Reduces inflammation within bronchial tubes and airways. Off label: Urticaria Prophylaxis and chronic treatment of asthma or allergic rhinitis. Prophylaxis, chronic treatment of asthma. Prevention of exerciseinduced bronchoconstriction. Off label: Urticaria 33 | P a g e PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA Dosage A: PO: 20 mg b.i.d. 1 h before or 2 h after meals; max: 40 mg/d C: >5 y: PO: 10 mg b.i.d.; max: 20 mg/d Hypersensitivity to zafirlukast; acute asthma attacks, including status asthmaticus, acute bronchospasm; children <5 years. Hypersensitivity to montelukast; severe asthmatic attack, status asthmaticus or acute bronchospasm Hepatic impairment, hepatic disease; patients 65 years older status asthmaticus Severe liver disease, suicidal ideation, breastfeeding, corticosteroid withdrawal LAB VALUES: Abnormal liver function tests (ALT, AST) DRUG Interactions to: o Dasabuvir o Leflunomide o Pixantrone o Teriflunomide Contraindications Cautions DRUG: Erythromycin, theophylline may decrease concentration/effect. May increase effects of warfarin (increases INR). HERBAL: None significant. FOOD: Food decreases bioavailability by 40%. LAB VALUES: None significant. Absorption: PO, rapidly Pharmacokinetics absorbed Bioavailability: Reduced 40% with food Distribution: 99% proteinbound Metabolism: t½: 10hrs, metabolized in liver Excretion: 90% excreted in feces, 10% in urine Pharmacodynamics PER OREM Interactions 34 | P a g e A: PO: 10 mg/d at least 2 h before exercise C: 6-15 y: PO: 5 mg/d at least 2 h before exercise Absorption: Well absorbed Distribution: 99% proteinbound Metabolism: t½: : 2.7-5.5 h Elimination: Feces, bile PER OREM PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA Side Effects Adverse Effects Onset: UK Peak: 3 hours Duration: 12 hours Frequent (13%): Headache. Occasional (3%): Nausea, diarrhea. Rare (less than 3%): Generalized pain, asthenia, myalgia, fever, dyspepsia, vomiting, dizziness. Onset: UK Peak: 3–4 h for oral tablet, 2–2.5 h for chewable tablet. Duration: 24 h Fever, headache, drowsiness, dizziness, fatigue, restlessness, insomnia, confusion, depression, nasal congestion, cough, sore throat, dental pain, influenza, dyspepsia, nausea, vomiting, abdominal pain, weight loss, rash Concurrent administration of inhaled corticosteroids increases risk of upper respiratory tract infection Angioedema, bleeding, vasculitis, seizures, edema Life-threatening: anaphylaxis, suicidal ideation, StevensJohnson syndrome Regularly assess respiratory and airway condition. Lab tests: Periodic liver function tests. Monitor closely PT and INR with concurrent warfarin therapy. Monitor closely phenytoin level with concurrent phenytoin therapy. Monitor effectiveness carefully when used in combination with phenobarbital or other potent cytochrome P450 enzyme inducers. Lab test: Periodic liver function tests. Taking medication regularly, even during symptom-free periods. Note: Drug is not intended to treat acute episodes of asthma. Report S&S of hepatic toxicity (see Appendix F) or Nursing Implications Assessment and Drug Effects Patient and Family Education 35 | P a g e Do not use for reversal of an acute asthmatic attack. Inform physician if shortacting inhaled bronchodilators are needed more often than usual with montelukast. PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA 36 | P a g e flu-like symptoms to physician. Follow-up lab work is very important. Notify physician immediately if condition worsens while using prescribed doses of all antiasthmatic medications. Do not breastfeed while taking this drug. Use chewable tablets (contain phenylalanine) with caution with PKU. Do not breastfeed while taking this drug. PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY Leukotriene Synthesis Inhibitor PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA Drug Classification zileuton (Zyflo CR) Pharmacotherapeutic: Leukotriene synthesis inhibitor; Bronchodilator Clinical: Antiasthma Trade name: Zyflo CR Pregnancy Category: C Mode of Action Therapeutic Effects Uses and Indications Dosage A: PO: 1200 mg b.i.d. within 1 hr after morning and evening meal Contraindications Hypersensitivity to zileuton or zafirlukast, active liver disease, lactation Cautions Hepatic insufficiency. Safety and effectiveness in children >12 y are not established. Interactions DRUG: May double theophylline levels and increase toxicity. Increases hypoprothrombinemic effects of warfarin. May increase levels of BETA BLOCKERS (especially propranolol), leading to hypotension and bradycardia. FOOD: Improved absorption when administered w/ food (controlled-release). Alcohol may increase CNS depression and risk of hepatotoxicity. Pharmacokinetics Inhibits 5-lipoxygenase, the enzyme needed to start the conversion of arachidonic acid to leukotrienes. Zileuton helps to prevent the signs and symptoms of asthma including airway edema, smooth muscle constriction, and altered cellular activity due to inflammation. For prophylaxis and maintenance therapy for chronic asthma. Reduces inflammation in airways and decreases bronchoconstriction Absorption: Rapidly absorbed from GI tract Distribution: 93% protein-bound Metabolism: t½: 2.5 hrs, metabolized in liver Excretion: Excreted primarily in urine (94%) Pharmacodynamics PER OREM 37 | P a g e Onset of Action: UK PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA Side and Adverse Effects Peak: 1.7 hours Duration: 5-8 hours Headache, dizziness, pain including pharyngolaryngeal pain, GI disturbances, myalgia, arthralgia, sinusitis, conjunctivitis, fever, hypertonia, lymphadenopathy, malaise, neuropsychiatric events (e.g. sleep disorders, behaviour changes), UTI, vaginitis, hypersensitivity, urticaria, rash, leucopenia, jaundice, hyperbilirubinaemia and elevated liver enzymes. Potentially Fatal: Severe hepatic injury. Nursing Implications Assessment and Drug Effects Patient and Family Education Assess respiratory status and airway function regularly. Lab tests: Periodic CBC and routine blood chemistry; monthly liver function tests for 3 mo, then every 2–3 mo for rest of first year, then periodically. Instructions for CONCURRENT THERAPIES: Reduce theophylline dose and closely monitor theophylline levels; closely monitor PT and INR with warfarin therapy; closely monitor phenytoin level with phenytoin therapy; closely monitor HR and BP for excessive beta blockade with propranolol therapy. Take medication regularly even during symptom-free periods. Drug is not intended to treat acute episodes of asthma. Report to physician promptly S&S of hepatic toxicity (see Appendix F) or flu-like symptoms. Follow-up lab work is very important. Notify physician if condition worsens while using prescribed doses of all antiasthmatic medications. Do not breastfeed while taking this drug. Nursing Process Assessment Record medical, drug, and herbal histories; note any drug-drug or drug-herb interactions. Record baseline vital signs for identifying abnormalities and for future comparisons. Assess for wheezing, decreased breath sounds, cough, and sputum production. Assess sensorium for confusion and restlessness caused by hypoxia and hypercapnia. Assess for a history of phenylketonuria when montelukast is prescribed, because children’s chewable tablets contain phenylalanine. Determine hydration; diuresis may result in dehydration in children and older adults. 38 | P a g e PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA Nursing Diagnosis Ineffective airway clearance related to retained secretions in bronchi Activity intolerance related to imbalance between oxygen supply and demand Deficient knowledge of OTC drug interaction related to lack of exposure to information Planning Patient will be free from wheezing, or wheezing has significantly improved. Patient’s lung fields will be clear within 2 to 5 days. Patient will take medications as prescribed. Interventions Monitor respirations for rate, depth, rhythm, and type. Monitor lung sounds for rhonchi, wheezing, or rales. Observe lips and fingernails for cyanosis. Monitor drug therapy for effectiveness. Observe for side effects. Provide adequate hydration; fluids aid in loosening secretions. Monitor liver function tests; AST and ALT may be elevated with zafirlukast and montelukast. Provide pulmonary therapy by chest clapping and postural drainage, as appropriate. Patient Teaching General Advise patient that if allergic reaction occurs (i.e., rash, urticaria), drug should be discontinued and health care provider should be notified. Monitor periodic liver function tests. Direct patient not to take St. John’s wort without first checking with health care provider, because this herb may decrease montelukast concentration. Warn patient that black or green tea and guarana with montelukast and zafirlukast may cause increased stimulation. Encourage patient to stop smoking. Discuss ways to alleviate anxiety (relaxation techniques, music). Advise patient having frequent or severe asthmatic attacks to wear an ID bracelet or MedicAlert tag. Encourage patient contemplating pregnancy to seek medical advice before taking montelukast. Caution patient or significant other not to open oral granule packets until ready for use. After opening packet, dose must be administered within 15 minutes. If mixed with baby formula or approved food (applesauce, carrots,rice, or ice cream), do not store for future use. Advise patient with known aspirin sensitivity to avoid a bronchoconstrictor response by avoiding aspirin and NSAIDs while taking montelukast. Self-Administration Teach patient not to use montelukast for reversal of an acute asthmatic attack, because it is only recommended for prevention of acute attacks and treatment of chronic asthma. Advise patient to continue to use the usual regimen of inhaled prophylaxis and short-acting rescue medication for exercise-induced bronchospasm. 39 | P a g e PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA Encourage patient to inform health care provider if short-acting inhaled bronchodilators are needed more often than usual with montelukast. Tell patient to comply with medication regimen even during symptom-free periods. Advise patient (especially children) that chewable tablets are to be chewed thoroughly because swallowing whole may alter absorption. Diet Tell patient to take leukotriene receptor antagonists in the evening for maximum effectiveness. Cultural Considerations Use both hands to show respect when offering a prescription, instructions, or pamphlets to Asians and Pacific Islanders. Evaluation Evaluate the effectiveness of the bronchodilators.Patient is breathing without wheezing and without side effects of the drug. Evaluate tolerance to activity. MAST CELL STABILIZERS Mast cells ● Mast cells or mastocytes are connective tissue cells that are responsible for the inflammatory response of the body, or its reaction to injury or infection. ● Mastocytes produce different substances such as histamine and leukotrienes, in response to inflammation or irritation, which causes the dilation of small blood vessels and kills bacteria. Mast Cell Stabilizer ● ● ● A mast cell stabilizer is a drug that focuses mainly on the inhibition of histamine and slow-reacting substance of anaphylaxis (SRSA) production at the cellular level. It prevents the mast cells from releasing substances that cause inflammation and bronchoconstriction during situations wherein mast cells are stimulated due to irritation or the presence of an antigen. Currently, there is only one drug still available under this drug class, Cromolyn. ○ It is an FDA-approved medication with the purpose revolving around the prophylaxis of bronchial asthma and treatment of allergic rhinitis and mastocytosis (the excessive gathering of mast cells in the body’s tissues) in pediatric and adult patients. Hence, it is the prototype drug of this class. 40 | P a g e PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA CROMOLYN Drug Name ● ● ● Drug Classification ● ● ● Dosage Generic Name: Cromolyn Chemical Name: Sodium Cromoglycate, Sodium Cromolyn Brand/Trade Name: NasalCrom, Gastrocrom, Intal Therapeutic: antiasthmatics, allergy, cold, and cough remedies Pharmacologic mast cell stabilizers Pregnancy Category B Adult Dose: ● ● Nasalcrom ○ 1 spray each nostril ○ 3 to 4 times a day Gastrocrom ○ Adults and Adolescents (13 years and above): 2 ampules 4 times a day, 30 minutes before meals and at bedtime Pediatric Dose: ● ● ● Indications ● ● ● ● 41 | P a g e Nasalcrom ○ 2 to 11 years old: 1 spray in each nostril ○ 3 to 4 times a day Intal ○ 5 years and above: 4 times at regular intervals (should not be exceeded) Gastrocrom ○ Children (2 to 12 years old): 1 ampule 4 times a day, 30 minutes before meals and at bedtime ○ Not recommended for pediatric patients under 2 years old Prophylaxis of severe bronchial asthma (it is not used for acute asthmatic attacks) Prevention of exercise-induced asthma Intranasal route: Prevention and treatment of seasonal and perennial allergic rhinitis. PO: Mastocytosis, treatment of food allergy, treatment of inflammatory bowel disease (IBD) PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA Therapeutic Actions ● Cromolyn inhibits the release of histamine and SRSA. ● It is able to prevent allergic asthmatic response when a person’s respiratory tract is exposed to the foreign substance through blocking the calcium ions from entering mast cells, which are needed for mast cell degranulation, thereby stopping the release of the stimulated chemical mediators. ● Cromolyn is not absorbed from the site of administration, therefore it only has a local effect. Since there are numerous drugs available for inflammation that are far more effective and have fewer side effects, cromolyn is not as frequently used compared in the past. ● There are several formulations of the drug: ○ ophthalmic solution for eye-related allergic symptoms, ○ nasal for allergic rhinitis, ○ inhaled form for allergies and; ○ capsule or oral form may prevent food allergy. ○ The nasal and eye drop forms of cromolyn are used for hay fever and the oral formulation is available for food allergy. Pharmacokinetics Pharmacokinetics Absorption ● ● ● ● Oral: 0.5 to 2 % Nasal: 8% Affects local areas only Small amounts may reach systemic circulation after inhalation Distribution ● Since only small amounts are absorbed, its distribution is unknown and does not have enough studies. Metabolism and Excretion ● ● Metabolized in the liver Small amounts absorbed are excreted unchanged in urine and feces Majority of the drug, about 98%, is excreted in the feces and the rest in the urine; others via exhalation ● Half-life 42 | P a g e 80 to 90 minutes PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA Route Onset Peak Duration Inhalation 1 to 2 weeks 2 to 4 weeks 6 to 8 hours Nasal 1 to 2 weeks 2 to 4 weeks 6 to 8 hours Oral 2 to 6 weeks 15 minutes 6 to 8 hours Contraindications and Cautions ● Cromolyn is contraindicated in patients who have shown hypersensitivity. ● It cannot also be used during acute attacks of asthma because it does not take action immediately and has no direct bronchodilator effects. ● The drug is not recommended for the usage of children 2 years old and below, due to the limited studies of its safety and efficacy. ● Furthermore, there is insufficient adequate and well-controlled studies when used in pregnant women and human response is different with regards to animal reproduction studies, therefore the risk is not yet defined. It must only be administered if needed and the benefit to the mother clearly outweighs potential risk to the fetus. ● There is no established studies if the drug can be excreted in breast milk, thus lactating women should use the drug with caution. Adverse Effects and Side Effects ● Its most common side effects include postnasal drip, irritation of the nose and airway, and cough--especially when administered through aerosol spray. Also, drug allergy cases are rare. These side effects may be decreased by drinking water before and after the administration of the drug. ● A serious side effect of cromolyn that may occur when the therapy is discontinued abruptly, rebound bronchospasm. ● Despite it having a low incidence of side effects, it is only moderately effective, accordingly, there are more and newer drugs produced that replaced the use of cromolyn. 43 | P a g e PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA Area of the body Adverse Effects/Side Effects Central Nervous System dizziness, headache Skin rash, urticaria, angioedema Ears, eyes, nose, throat (EENT) intranasal— nasal irritation, nasal congestion, sneezing Respiratory inhalation— irritation of the throat and trachea, cough, wheezing, bronchospasm Gastrointestinal nausea, unpleasant taste, diarrhea Others allergic reactions including ANAPHYLAXIS or worsening of conditions being treated Drug to Drug Interactions ● Currently, it is said that there are no existing drug to drug interactions. Nursing Considerations ● Assessment ○ Perform a physical examination to have a baseline data of the client and to serve as a basis for the assessment of the effectiveness of the drug and drug therapy, including the occurrence of adverse effects. ○ Assess for possible contraindications or cautions before administering the drug or beginning the drug therapy, keeping in mind the adverse effects and if there is any presence of impaired renal or hepatic function. ■ Impaired renal or hepatic function may affect the metabolization or excretion of the drug. ○ Assess lung sounds and respiratory function to evaluate the effectiveness of the drug before and routinely during the drug therapy. ● Diagnoses ○ ○ ○ ○ 44 | P a g e Ineffective airway clearance Acute Pain related to local effects, headache, or GI effects Risk for Injury related to CNS effects Deficient Knowledge regarding drug therapy PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA ● Implementation ○ ○ ○ ○ Review the proper administration procedure and delivery with the patient periodically to ensure the effectiveness of the drug. Instruct the patient of cautions, especially avoiding the abruptly discontinuation use of the drug to prevent adverse effects. Provide patient teaching of the needed information namely the drug name, dosage, cautions, warning signs that may indicate potential problems to avoid any adverse effects such as the usage of the drug during acute asthmatic attacks and to enhance patient knowledge of the drug therapy and it promotes cooperation. Ensure to offer support and encouragement to guide and aid the patient throughout the drug therapy and cope with it. ● Evaluation ○ ○ ○ ○ Monitor the patient’s response to the drug and drug therapy, to know the effectiveness such as the improvement of breathing, relief of signs of allergic disorders. Monitor for any adverse effects for early detection and to avoid further complications. Evaluate the effectiveness of the patient teaching to ensure patient knowledge. The therapeutic effects are usually observable within 2 to 4 weeks after the beginning of therapy. Patient Education ● Instruct patient and/or guardian on the correct use of medication and all the needed information. ● ● ● ● ● The medication must be administered routinely and should not exceed the prescribed dose. Missed doses must be taken as soon as remembered, but still with regular intervals with other doses. Double doses are not allowed. The therapy must not be discontinued abruptly without the physician’s instructions or adverse effects may occur. Throat irritation, cough, and hoarseness may be minimized by the following actions: gargling water, drinking a few amounts of water, or by taking a lozenge after each treatment. Know the correct procedure or proper actions when an acute asthma attack occurs. Cromolyn is not applicable for acute asthma. Cromolyn does not entirely eliminate the continued need for therapy with bronchodilators, expectorants, antibiotics, or corticosteroids, but they may be reduced in terms of their amount and usage frequency. Note and immediately contact your physician for any unusual signs or symptoms, such as adverse effects (e.g., hypersensitivity reactions) for these can be severe or life-threatening. Physicians may advise the patient to discontinue the use of drug when an allergic reaction is detected. Remember the contraindications and cautions of the drug to avoid complications. REFERENCES Comerford, K. C., & Durkin, M. T. (2021). Nursing 2021 drug handbook. 41st edition. Philadelphia: Wolters Kluwer. Hodgson, B. B., & Kizior, R. J. (2020). Saunders nursing drug handbook. Philadelphia: Saunders. 45 | P a g e PAMANTASAN NG LUNGSOD NG MAYNILA | COLLEGE OF NURSING| BLOCK 2 PHARMACOLOGY PROFESSOR MARY CRIS T. ROMBAOA ANIEVAS| BAUTISTA| COSING| DAYAO| DEL PILAR| DOMASIN| ECHANO| PRILLA Karch, A. M. (2017). Focus on nursing pharmacology. Seventh edition. Philadelphia: Wolters Kluwer. Katzung, B. G. (2004). Basic & clinical pharmacology. New York: Lange Medical Books/McGraw Hill. Katzung, B. G., Kruidering-Hall, M., & Trevor, A. J. (2019). Katzung & Trevor's pharmacology: Examination & board review (Twelth edition.). New York: McGraw-Hill Education. LeFever Kee, J., Hayes, E. R., & McCuistion, L. E. (2015). Pharmacology: A patient-centered nursing process approach. St. Louis, MO: Elsevier/Saunders. 8. Tortora, G. J. (2006). Principles of anatomy and physiology. 11th ed. Hoboken, NJ: J. Wiley. 46 | P a g e