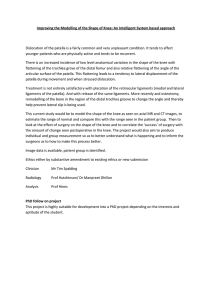
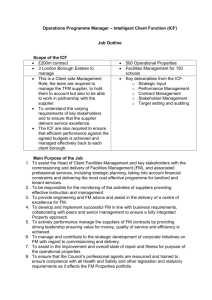
Case Report Kevin Helgeson, A Russell Smith Jr K Helgeson, PT, DHSc, is Assistant Professor, Physical and Occupational Therapy Department, Idaho State University, Campus Stop 8045, Pocatello, ID 83209-8045 (USA). Address all correspondence to Dr Helgeson at: helgkevi@ isu.edu. AR Smith Jr, PT, EdD, OCS, FAAOMPT, is Chair, Athletic Training and Physical Therapy Department, Brooks College of Health, University of North Florida, Jacksonville, Florida. [Helgeson K, Smith AR Jr. Process for applying the International Classification of Functioning, Disability and Health model to a patient with patellar dislocation. Phys Ther. 2008;88:956 –964.] © 2008 American Physical Therapy Association Background and Purpose. The International Classification of Functioning, Disability and Health (ICF) has been proposed as a possible framework for organizing physical therapist practice. The purpose of this case report is to describe an evaluative and diagnostic process that is based on the ICF framework for a patient with a patellar dislocation. Case Description. The patient was a 23-year-old woman who sustained a right knee and patellofemoral joint injury, resulting in a sprain of the medial collateral ligament and a suspected sprain of the medial patellofemoral ligament. Evaluation at 4 weeks demonstrated a primary impairment of patellar instability associated with the primary activity limitation of limited walking distances. A plan of care to address impairments, activity limitations, and participation restrictions was developed, with modifications made on the basis of the patient’s health condition and personal and environmental factors. Outcomes. The patient attained all of her goals for therapy and was able to return to her normal activities and recreational pursuits without a recurrence of a patellar dislocation. Lower-Extremity Function Scale scores increased from 30 out of 80 to 76 out of 80 during the course of treatment. Discussion. The ICF model has been proposed as a framework for developing diagnostic classifications for rehabilitation professionals. The ICF model also should be assessed with regard to whether it provides a useful process for clinical decision making. The ICF model directs practitioners to address patients’ problems at the level of the whole person, with modifications made on the basis of health conditions and personal and environmental factors. Post a Rapid Response or find The Bottom Line: www.ptjournal.org 956 f Physical Therapy Volume 88 Number 8 August 2008 Downloaded from https://academic.oup.com/ptj/article-abstract/88/8/956/2683635 by guest on 26 June 2020 Process for Applying the International Classification of Functioning, Disability and Health Model to a Patient With Patellar Dislocation Applying the ICF After Patellar Dislocation T A patellar dislocation may result in damage to the soft and bony tissues of the patellofemoral joint.4 – 6 A significant sprain or rupture of the medial patellofemoral ligament (MPFL) has been highly associated with a lateral dislocation of the patella and can be considered the essential lesion responsible for ongoing patellar instability.4,5,7 Consideration of the healing time needed for the MPFL is critical in the design of rehabilitation programs for patients with patellar dislocations. Studies of rehabilitation programs used after patellar dislocations have described interventions only in broad terms, with impairment-level goals for range of motion and strength (force-generating capacity) and for a return to activities.8 –10 developed on the basis of an evaluative process that considers patients’ examination findings, their goals for returning to activities, and the prevention of further patellar subluxation and dislocation events. A plan of care based on just a consideration of patients’ impairments and associated pathologies may not consider the problems at the level of the whole person. Rehabilitation programs for patients with patellar dislocations need to be Case Description Figure 1. Components and definitions of the International Classification of Functioning, Disability and Health (ICF) model.1 Health conditions⫽umbrella term for diseases, disorders, injuries, or traumas; body function⫽physiological functions of body systems; body structure⫽anatomic parts of the body; impairments⫽problems in body function or structure, such as a significant deviation or loss; activities⫽execution of tasks or actions by an individual; activities limitations⫽difficulties an individual may have in executing activities; participation⫽involvement in a life situation; participation restrictions⫽ problems an individual may experience in involvement in life situations; environmental factors⫽physical, social, and attitudinal environments in which people live and conduct their lives; personal factors⫽particular background of an individual’s life and living, comprising features of an individual that are not part of a health condition. Reprinted with permission from: International Classification of Functioning, Disability and Health: ICF. Geneva, Switzerland: World Health Organization; 2001. August 2008 The purpose of this case report is to describe an evaluative and diagnostic process that is based on the ICF model for a patient with a knee injury, that addresses the patient’s current impairments and limitations, and that can be used to develop strategies to prevent recurrences. The patient was a 23-year-old female graduate school student who incurred a right-knee injury during a recreational floor hockey game. She reported feeling her right patella in a dislocated position that she was able to reduce by extending her knee. She was subsequently seen in a local emergency department; she was assessed as having a knee sprain and was placed in a knee extension immobilizer. Because she was about to leave school for Christmas break, she was advised to follow up with an orthopedic surgeon in her hometown. She was seen the following week by an orthopedic surgeon, who concluded that she had incurred a second-degree tear of the medial collateral ligament (MCL) of the right knee, with a lateral dislocation of the patella. She was referred for magnetic resonance imaging (MRI) of her right knee; the MRI was performed the following week. The MRI findings reported by the radiologist were “sprain of the medial collateral ligament with overlying edema and bone bruises of the posterior medial tibial plateau and of the lateral femoral condyle with a Volume 88 Number 8 Physical Therapy f 957 Downloaded from https://academic.oup.com/ptj/article-abstract/88/8/956/2683635 by guest on 26 June 2020 he International Classification of Functioning, Disability and Health (ICF) has been proposed by the World Health Organization as a unified framework for describing the health status of people (Fig. 1).1 The ICF recently was discussed in the physical therapy community as a possible framework for organizing and directing treatment for patients and clients.2,3 Jette3 described the language, framework, and concepts used within the ICF. Discussions about the ICF have centered on how this framework or model can be used to develop diagnostic classifications, with little discussion of whether the model provides a process that is useful for clinical decision making. In this case report, we describe a process of applying the components of the ICF model for a patient with a knee injury. Applying the ICF After Patellar Dislocation The patient’s first visit to a physical therapist was at a university campus physical therapy clinic 4 weeks after her injury. She reported that this was her fourth right patellar dislocation event and that she had also had multiple left patellar dislocations. The patient gave written informed consent for treatment, and Health Insurance Portability and Accountability Act guidelines were followed. The patient was very anxious to regain her mobility because she was in her last semester of graduate school in geology and would need to be making field trips to geological sites for sample collection. She also was concerned that her repeated patellofemoral injuries would interfere with her future work as a geologist, which would require her to make frequent hikes over uneven terrain. During her initial visit, she reported having mild medial patellofemoral discomfort that increased with walking long distances. This was a significant problem at that time of year because she usually walked 0.8 km (0.5 mile) to and from campus in snowy and icy conditions. She re958 f Physical Therapy Volume 88 Figure 2. Identification of patient information and classification into the International Classification of Functioning, Disability and Health model. Modified and reprinted with permission from: International Classification of Functioning, Disability and Health: ICF. Geneva, Switzerland: World Health Organization; 2001. ported feelings of instability in her right patella when descending stairs and walking on uneven surfaces. Her score on the Lower-Extremity Function Scale was 30 out of a possible score of 80, indicating the inability to squat, run, hop, or participate in her normal recreational activities.12 A review of systems demonstrated normal finding for the myotomes and dermatomes in the lower extremities. Active movements of the left lower extremity and trunk were all within normal limits. The patient was ⬃165 cm (65 in) tall and weighed ⬃59 kg (132 lb), for a body mass index of 22. She appeared be very fit and healthy and was very knowledgeable about her knee condition. Clinical Impression The patient’s detailed knowledge of the history of her condition allowed for the identification of patient infor- Number 8 mation and classification into the ICF model (Fig. 2). The focus of the examination was to further identify and measure her body function and structure impairments and activity limitations. The interrelationships of the ICF framework components would continue to be evaluated during the examination. Examination The patient’s gait pattern was characterized by her right knee being held in an extended position throughout the stance phase, limited ankle plantar flexion at the end of the stance phase, and limited knee flexion during the swing phase. A walking speed test demonstrated her walking 35 m in 25 seconds, for a speed of 83.3 m/min (2.7 miles/h). Her standing posture showed normal alignments of the lower extremities. She was able to stand on the right leg only without discomfort for 30 seconds. August 2008 Downloaded from https://academic.oup.com/ptj/article-abstract/88/8/956/2683635 by guest on 26 June 2020 small knee joint effusion.” These MRI findings are consistent with a “flexion with valgus and external rotation” mechanism for a knee injury that also is associated with lateral patellar dislocations.11 The radiologist’s report did not include an assessment of the patellofemoral joint. At 3 weeks after the injury, the patient was again seen by the orthopedic surgeon, who concluded that the ligamentous sprain was healing satisfactorily. The surgeon encouraged her to start moving her knee as tolerated and to begin a rehabilitation program as soon as she returned to campus. She was given a neoprene knee sleeve with a cutout and lateral pad for the patella to wear and was advised to take ibuprofen at 800 mg/d for knee pain. Applying the ICF After Patellar Dislocation tibial attachment of the MCL and over the medial patellofemoral joint. The medial patellofemoral joint discomfort was further localized toward the medial femoral condyle, the attachment site for the MPFL. Ligamentous testing of the knee joint was deferred on the basis of the patient’s knowledgeable report of her condition and her overall anxiety regarding passive movements of her knee. The patient expressed apprehension with minimal amounts of medial and lateral gliding of the right patella as well as with lateral gliding of the left patella. To further assess the stability of her patellofemoral joint, her knee was flexed to the point at which she began to complain of medial patellofemoral discomfort (approximately 80° of flexion); a medially directed force placed across the patella immediately relieved the medial patellofemoral discomfort. These findings were interpreted to mean that increasing tension within the MPFL and other medial knee joint tissues with knee flexion decreased with a medially directed force (Fig. 3).13 Application of the ICF Model The ICF framework was used to organize the patient’s examination information, make judgments about the examination findings, and guide the decisions needed for the management of the patient’s condition.14 The first step was to classify all of the examination findings into the following components: body function and structure impairments, activity limitations, participation restrictions, and environmental and personal factors (Fig. 4).1 The second step was to evaluate the interrelationships among each of the 6 concepts of the ICF framework. The following principles were used in this step: 1. The ICF model does not describe unidirectional causations of the components but does describe associations or relationships among the components. 2. The first consideration is the patient’s problems at the level of the whole person; these are her activity limitations and participation restrictions. 3. Consistent with the scope of physical therapist practice,14 the relationships between a patient’s activity limitations and impaired body functions and structures are the emphasis of the evaluative process for determining a diagnosis and plan of care. Figure 3. Relief of medial patellofemoral discomfort when the knee was placed at 80 degrees of flexion and a medially directed force was applied to the patella (arrow). August 2008 The third step was to prioritize or rank the activity limitations. The activity limitation the patient considered to be her most significant current problem was identified. Most Volume 88 Number 8 Physical Therapy f 959 Downloaded from https://academic.oup.com/ptj/article-abstract/88/8/956/2683635 by guest on 26 June 2020 The patient’s right knee passive range of motion showed full extension, but she tolerated only 85 degrees of knee flexion, with complaints of medial patellar pain and what she described as a “catching sensation.” Volitional contraction of the right quadriceps femoris muscle groups was assessed with the lower extremities supported on a plinth with the knees extended. Visual and palpatory comparisons of the isometric quadriceps femoris muscle contractions demonstrated significantly decreased contraction of the right quadriceps femoris muscle versus the left muscle. Circumferential measurements of the right and left thighs at 10 and 20 cm above the knee joint line showed decreases of 2 and 4 cm, respectively, in the right thigh muscle circumference. Palpation of the right knee demonstrated diffuse swelling over the medial aspect of the joint, with tenderness over the Applying the ICF After Patellar Dislocation Next, possible relationships between the patient’s primary activity limitations and body function and structure impairments were evaluated. Many relationships were considered for this patient. For example, the diminished function of her quadriceps muscle was considered to be related to the limitations in ambulation, especially in walking long distances to and from school. Medial patellofemoral joint discomfort also was an important feature because this discomfort was what she initially described as limiting her walking abilities. The structural impairments of the MCL sprain and the suspected MPFL rupture, along with residual swelling from the injury, were considered to be related to the limitations in walking and might have been related to an inhibition of the quadriceps muscle function and to pain. The impaired mobility of the knee was not considered to be closely associated with the limitations in walking long distances because the knee flexion range was more than that needed for ambulation.15 The strongest relationship with the patient’s primary activity limitation was considered to be the finding of impaired stability of the patellofemoral joint. This impaired stability of joint function was closely associated with the impaired structure of the MPFL from her injury.4,5,7 This impaired stability was a recurrent problem for this patient and might 960 f Physical Therapy Volume 88 Figure 4. Classification of all of the examination findings into the components of the International Classification of Functioning, Disability and Health. Modified and reprinted with permission from: International Classification of Functioning, Disability and Health: ICF. Geneva, Switzerland: World Health From figOrganization; 4 to 5, the2001. stability becomes the main impairment have been related to other structural impairments or to a problem with controlling lower-extremity movements. The impaired stability of the patellofemoral joint was considered to be the primary impairment, with secondary impairments of pain in the patellofemoral joint, diminished quadriceps femoris muscle function, and impaired knee joint mobility. Following these clinical judgments of the relationships and identification of the primary impairment, the model was reorganized (Fig. 5). In addition to the patient’s immediate needs, the prevention of recurring patellar dislocations would be a long-term consideration for this patient. She considered regular exercise and recreational activities to be important components of her physical and psychological health status. The long-term instability of her patella had significant social and economic consequences because her Number 8 ability to hike over rocky terrain for long distances was necessary for the collection of geological samples for her graduate school work and future employment as a geologist. The application of the ICF model to this patient began with identification of the components of the model determining her problems at the level of the whole person. The evaluative process focused on the relationship between activity limitations and impairments. As indicated by this process, the most appropriate diagnostic label for this patient is the relationship between the primary activity limitation and the primary impairment, which was limited ambulation distance associated with patellofemoral joint instability. This diagnostic label will help to direct the goals and plan of care for this patient. August 2008 Downloaded from https://academic.oup.com/ptj/article-abstract/88/8/956/2683635 by guest on 26 June 2020 significant to the patient was her limitation in walking long distances, which was clearly related to her limited participation in recreational activities and potentially limited her participation in the data collection needed to complete her degree in geology. Limited walking distance, therefore, was ranked as her primary activity limitation. Because she also reported significant limitations with stair climbing, this was considered to her secondary activity limitation. Applying the ICF After Patellar Dislocation Reorganization of the International Classification of Functioning, Disability and Health (ICF) model following clinical judgments of the relationships among the components of the ICF and identification of the primary limitation and impairment. Modified and reprinted with permission from: International Classification of Functioning, Disability and Health: ICF. Geneva, Switzerland: World Health Organization; 2001. The patient’s prognosis was based on her current level of activities and impairments and the normal healing time for ligaments. Her prognosis was a return to her usual walking and hiking activities within 12 weeks. The prevention of future patellar injuries was considered the most difficult challenge because of her previous patellar dislocations.4,5,10 Intervention Consistent with the ranking of the patient’s activity limitations and participation restrictions, she agreed to the following goals for her physical therapy program: 1. Walking needed for transportation from her home to school without patellar instability in 4 weeks. 2. Ascending and descending stairs without patellar instability in 4 weeks. August 2008 3. Returning to hiking activities without patellar instability in 8 weeks. The ICF model includes environmental and personal factors as important modifying variables in the development of patients’ goals and interventions. Because of the environmental factor of the patient needing to walk for daily transportation in snowy and icy conditions, she was encouraged to wear the neoprene sleeve and use proper footwear when walking outside.16 The patient’s personal factors of being recreationally active and knowledgeable about her condition made these restrictions and precautions easy for her to agree upon. Interventions directed at improving the dynamic stability of the patellofemoral joint were considered appropriate to address both the primary and the secondary impairments in the stability of the patellofemoral Cryotherapy with cold packs and ice massage was used to address the pain-related impairments and to control swelling around the knee. Because impaired knee mobility was not highly ranked and knee flexion past 80 degrees seemed to be causing tensioning of the MPFL, knee flexion was limited for the first 2 weeks of treatment in order to allow these tissues to heal and regain their normal extensibility. * Autogenic Systems, 620 Wheat Ln, Wood Dale, IL 60191. † The Hygenic Corp, 1245 Home Ave, Akron, OH 44310-2575. Volume 88 Number 8 Physical Therapy f 961 Downloaded from https://academic.oup.com/ptj/article-abstract/88/8/956/2683635 by guest on 26 June 2020 Figure 5. joint and the diminished function of the quadriceps femoris muscles. First, isometric contractions of the quadriceps femoris muscle group with the knee in extended positions was facilitated with the use of auditory and visual biofeedback.* This exercise progressed to exercise with the patient sitting in a chair with the knee flexed to 45 degrees and the right foot resting on the floor. Isometric contractions of the quadriceps femoris muscles, along with cocontractions of the hamstring and hip extensor muscles, were initiated by having the patient press her heel downward onto an inclined platform (Fig. 6). Because the patient had a history of patellofemoral instability, which has been associated with motor control problems throughout the lower extremities,17 this exercise progressed to standing with the knee at approximately 15 degrees of flexion to reproduce the position of the right lower extremity during the initial contact period of the gait cycle.18 Balance activities were started with the patient standing on the right leg only and then progressed to singleleg standing activities with perturbations with a Thera-Band† (Fig. 7) and with the patient maintaining good alignment and stability at the hip, knee, and ankle joints.19,20 Applying the ICF After Patellar Dislocation Figure 6. Sitting quadriceps femoris muscle sets. Contraction of the quadriceps femoris muscle group was initiated by pressing the foot downward. Electromyographic activity of the vastus medialis muscle was monitored with a biofeedback unit. The exercise progressed to a standing position to replicate the lower-extremity position during the initial contact period of the gait cycle. Dynamic control of the lower extremities with stepping motions was introduced with an ⬃20-cm (8-in) step.21 This stepping activity progressed to ascending and descending stairs with the patient keeping the knee aligned with the foot and maintaining control of the hip and thigh muscles. Passive knee flexion, with stretches of up to 2 minutes in duration, was added during the third week. The patient had minimal discomfort with knee flexion at that time and reached full knee flexion within the next 6 weeks. The patient did not attend therapy sessions during weeks 5 to 8 because of graduate school work that included hiking into remote areas. She returned to therapy during weeks 9, 11, and 12 to continue her exercise program and monitor her symptoms. Lower-extremity squatting, stepping, and hopping activities progressed during these visits, and the patient continued with these activities during her home exercise program. The patient was counseled to avoid knee valgus and laterally (externally) rotated positions during activities to 962 f Physical Therapy Volume 88 Figure 7. Single-leg standing activities with perturbations. The patient was instructed to hold on to the Thera-Band at the level of the umbilicus, and oscillating perturbations were applied by the therapist pulling on the Thera-Band. Perturbations can be applied in multiple directions and at various speeds and intensities. Number 8 August 2008 Downloaded from https://academic.oup.com/ptj/article-abstract/88/8/956/2683635 by guest on 26 June 2020 The emphasis during the third and fourth weeks of treatment continued to be dynamic control of the lower extremities with decreasing levels of protection of the healing tissues.20 The emphasis of the exercises was to replicate the multijoint movements that occurred during the patient’s activities of walking and squatting while maintaining good dynamic control of the patellofemoral joint as well as the rest of the lower extremity. Walking forward and backward was used to increasing the patient’s walking speed through longer stride length and arm swing. The patient performed standing, squatting, and lunging activities while keeping the hip, knee, and ankle aligned and maintaining control of the hip and thigh muscles. Applying the ICF After Patellar Dislocation decrease the risk of recurrent patellar subluxation and dislocation. Outcomes The patient was contacted at 6 months after the injury and indicated that she was able to tolerate the hiking activities required to complete her graduate degree in geology and was planning to work as a geologist in the western United States. Discussion The ICF model is a secondgeneration biopsychosocial model designed as a framework for developing diagnostic classifications for rehabilitation professionals.1 Biopsychosocial or disablement models have been advocated as the models that typify physical therapist practice and are the models used for organizing clinical practice.3,14 The ICF model, as proposed by the World Health Organization, does not provide a “process” for evaluating functioning and disability; rather, the model provides users with building blocks with which to conAugust 2008 An important aspect of this evaluative process is the ability to reevaluate the interrelationships within the ICF framework and decisions made throughout the course of treatment. The choice of impaired patellofemoral joint stability as the primary impairment for the patient in this case report was reevaluated through an assessment of the level of improvement of the patient’s primary activity limitation. If she had not been making progress toward resolving the activity limitation in the first weeks of treatment, then reevaluation of the primary and secondary impairments would have been indicated. If the primary impairment of limited patellofemoral joint stability was still considered to be appropriate, then changes to the interventions would have been considered. One of the concerns for many clinicians regarding disablement models has been how a patient’s pathology will be considered and applied to the plan of care. The ICF model provides for the consideration of the patient’s health condition and impaired body structures. The health condition of the patient in this case report included repeated patellofemoral joint injuries and impaired structures, including the MCL and possibly the MPFL. The primary lesion demonstrated in imaging studies and surgical examinations of patellofemoral joints after patellar dislocation is a sprain or rupture of the MPFL.4 – 6 The plan of care for this patient was directed initially at protecting the healing tissues and then at addressing the lack of patellofemoral joint stability. Interventions directed at resolving primary or secondary impairments need to be appropriate for and modified on the basis of a patient’s health condition. For the patient in this case report, the secondary impairment of impaired mobility of the knee joint was not addressed until the MPFL had had adequate time to heal. People with patellar instability potentially have ongoing pain and instability and may choose to significantly limit their activities to avoid these problems.8,23,24 Limitations in recreational pursuits may have a significant impact on the overall quality of life and health status for these people. Conclusion This case report highlights an evaluative process in which the ICF framework is applied for a patient with a patellar dislocation. The ICF framework allowed for an evaluation at the level of the whole person, with selection of goals and interventions appropriate for the patient. Consideration by physical therapists of the ICF model as a classification system as well as an evaluative process may be beneficial in the care of patients and the management of various conditions. Both authors provided concept/idea/project design and writing. Dr Helgeson provided data collection, project management, the patient, and facilities/equipment. Dr Smith provided consultation (including review of manuscript before submission). This article was submitted August 14, 2007, and was accepted April 4, 2008. DOI: 10.2522/ptj.20070233 References 1 International Classification of Functioning, Disability and Health: ICF. Geneva, Switzerland: World Health Organization; 2001. Volume 88 Number 8 Physical Therapy f 963 Downloaded from https://academic.oup.com/ptj/article-abstract/88/8/956/2683635 by guest on 26 June 2020 The patient reached the first and second goals of walking to and from school and ascending and descending stairs without patellar instability by week 3 of treatment and then attained the third goal of tolerating hiking activities without patellar instability by completing her data collection during weeks 5 and 6 of her rehabilitation program. At week 9 of the program, the patient scored 76 out of 80 points on the LowerExtremity Function Scale, indicating some difficulties with squatting and running on uneven surfaces.12,22 Treatment goals were then reestablished to include a return to running activities. By week 12 of treatment, the patient was running for up to approximately 3 km (2 miles) 3 times per week and was maintaining an independent program of lowerextremity weight-lifting activities and jumping activities. sider the possible interactions among the components of the ICF and to explore possible processes for describing or evaluating patient problems.1(p18) The evaluative process described in this case report has been useful for the evaluation of patients with musculoskeletal conditions. Physical therapists treating other types of conditions should explore whether this process is useful for the evaluation of their patients. Applying the ICF After Patellar Dislocation 964 f Physical Therapy Volume 88 11 Hayes CW, Brigido MK, Jamadar DA, Propeck T. Mechanism-based pattern approach to classification of complex injuries of the knee depicted at MR imaging. Radiographics. 2000;20(special number): S121–S134. 12 Binkley JM, Stratford PW, Lott SA, Riddle DL. The Lower Extremity Functional Scale (LEFS): scale development, measurement properties, and clinical application. North American Orthopaedic Rehabilitation Research Network. Phys Ther. 1999;79: 371–383. 13 Tanner SM, Garth WP Jr, Soileau R, Lemons JE. A modified test for patellar instability: the biomechanical basis. Clin J Sports Med. 2003;13:327–338. 14 Guide to Physical Therapist Practice. 2nd ed. Phys Ther. 2001;81:9 –746. 15 Neumann DA. Kinesiology of the Musculoskeletal System. St Louis, Mo: Mosby; 2002:557. 16 Herrington L, Simmonds C, Hatcher J. The effect of a neoprene sleeve on knee joint position sense. Res Sports Med. 2005;13: 37– 46. 17 Powers CM. The influence of altered lower extremity kinematics on patellofemoral joint dysfunction: a theoretical perspective. J Orthop Sports Phys Ther. 2003;33:639 – 646. 18 Cowan SM, Bennell KL, Crossley KM, et al. Physical therapy alters recruitment of the vasti in patellofemoral pain syndrome. Med Sci Sports Exerc. 2002;34:1879 –1885. Number 8 19 Cowan SM, Bennell KL, Hodges PW, et al. Simultaneous feedforward recruitment of the vasti in untrained postural tasks can be restored by physical therapy. J Orthop Res. 2003;21:553–558. 20 Voight M Cook G. Impaired neuromuscular control: reactive neuromuscular training. In: Prentice WE, Voight ML, eds. Techniques in Musculoskeletal Rehabilitation. New York NY: McGraw-Hill; 2001:93–124. 21 Boling MC, Bolgla LA, Mattacola CG, et al. Outcomes of a weight-bearing rehabilitation program for patients diagnosed with patellofemoral pain syndrome. Arch Phys Med Rehabil. 2006;87:1428 –1435. 22 Watson CJ, Propps M, Ratner J, et al. Reliability and responsiveness of the Lower Extremity Functional Scale and the Anterior Knee Pain Scale in patients with anterior knee pain. J Orthop Sports Phys Ther. 2005;35:136 –146. 23 Hawkins RJ, Bell RH, Anisette G. Acute patellar dislocation: the natural history. Am J Sports Med. 1986;14:117–120. 24 Arendt EA, Fithian DC, Cohen E. Current concepts of lateral patella dislocation. Clin Sports Med. 2002;21:499 –519. August 2008 Downloaded from https://academic.oup.com/ptj/article-abstract/88/8/956/2683635 by guest on 26 June 2020 2 Coffin-Zadai CA. Disabling our diagnostic dilemmas. Phys Ther. 2007;87:641– 653. 3 Jette AM. Toward a common language for function, disability, and health. Phys Ther. 2006;86:726 –734. 4 Arendt EA, Fithian DC, Cohen E. Current concepts of lateral patella dislocation. Clin Sports Med. 2002;21:499 –519. 5 Elias DA, White LM, Fithian DC. Acute lateral patellar dislocation at MR imaging: injury patterns of medial patellar soft-tissue restraints and osteochondral injuries of the inferomedial patella. Radiology. 2002; 225:736 –743. 6 Nomura E, Inoue M. Cartilage lesions of the patella in recurrent patellar dislocation. Am J Sports Med. 2004;32:498 –502. 7 Steensen RN, Dopirak RM, McDonald WG III. The anatomy and isometry of the medial patellofemoral ligament: implications for reconstruction. Am J Sports Med. 2004;32:1509 –1513. 8 Nikku R, Nietosvarra Y, Aalto K, Kallio PE. Operative treatment of primary patellar dislocation does not improve mediumterm outcome: a 7-year follow-up report and risk analysis of 127 randomized patients. Acta Orthop. 2005;76:699 –704. 9 Beasly LS, Vidal AF. Traumatic patellar dislocation in children and adolescents: treatment update and literature review. Curr Opin Pediatr. 2004;16:29 –36. 10 Atkin DM, Fithian DC, Marangi KS, et al. Characteristics of patients with primary acute lateral patellar dislocation and their recovery within the first 6 months of injury. Am J Sports Med. 2000;28:472– 479.