Unit 1:
Introduction to Epidemiology
1
Unit 1 Learning Objectives:
1. Define and understand the uses of epidemiology.
2. Distinguish between public health, epidemiology, and
clinical medicine.
3. Understand the inter-disciplinary nature of
epidemiology.
6. Understand the “epidemiologic transition” of causes
of mortality from developing to developed countries.
7. Understand the natural history of disease
progression.
8. Distinguish between primary, secondary, and tertiary
2
levels of disease prevention.
PRACTICAL DEFINITION OF
DISEASE AND EXPOSURE
Disease: broad array of health conditions that
we seek to understand and ultimately modify,
including physiologic states, mental health,
and the entire spectrum of human diseases
(synonym: outcome, dependent variable).
Exposure: a catch-all term for agents,
interventions, conditions, policies, and
anything that might affect health (synonym:
predictor/explanatory/independent variable).
3
Discussion Question 1
When we think of studying “disease”,
is “disease” a stable concept?
4
Discussion Question 1
Probably not, because:
1. Cultural values can influence definitions and
perceptions of disease (especially psychiatric
disorders).
2. Improvements in diagnostic instrumentation
can lead to earlier detection of asymptomatic
disease.
3. Clinical thresholds for disease classification
change over time.
5
EPIDEMIOLOGY
Greek:
EPI - Upon
DEMOS - People
LOGOS - Study of, Body of
Knowledge
6
DEFINITIONS OF EPIDEMIOLOGY
• The study of the distribution and
determinants of disease frequency in
human populations. (1970)
• The study of the distribution and
determinants of health-related states or
events in specified populations, and the
application of this study to control of
health problems. (1988)
7
DEFINITIONS OF EPIDEMIOLOGY
The underlying premise of
epidemiology is that disease not
occur at random, but rather in
patterns that reflect the operation of
underlying factors.
8
DEFINITIONS OF PUBLIC HEALTH
• The science and art of :
1) preventing disease
2) prolonging life and
3) promoting health and efficiency through
organized community effort. (1920)
9
DEFINITIONS OF PUBLIC HEALTH (cont’d)
• To fulfill society’s interest in assuring
conditions in which people can be healthy.
• The field of health science concerned with
safeguarding and improving the physical,
mental and social well-being of the
community as a whole. (1992)
10
THE CONTENT OF PUBLIC HEALTH PRACTICE
• Focus on primary prevention.
• Community protection through monitoring and
surveillance for infectious and toxic agents.
• Response to unanticipated natural and humangenerated disasters.
• Health promotion through programs to notify
and educate the community about risks and
protective measures.
• Target hard-to-reach populations with clinical
services.
11
Why is epidemiology the basic science of
public health?
PUBLIC HEALTH WORKS BY:
• Defining a health problem
• Identifying risk factors associated with the
problem
• Developing and testing community-level
interventions to control or prevent the causes of
the problem
• Implementing interventions to improve the health
of the population; and
• Monitoring those interventions to assess their
effectiveness
12
EPIDEMIOLOGY HAS THE
METHODOLOGY TO:
• Determine the extent of disease in the community
• Study the natural history and prognosis of
disease
• Identify associations and potential etiology
(causes) of a disease and risk factors for disease
• Evaluate new preventive and therapeutic
measures and new modes of health care delivery
13
EPIDEMIOLOGY HAS THE
METHODOLOGY TO:
• Provide a foundation for developing public
policy and regulatory decisions relating to
environmental problems.
• In short, the primary goal of epidemiology
is to measure relationships between
“exposures” and health outcomes – these
may provide a basis for public health
initiatives and policies.
14
THE RELATIONSHIP BETWEEN
EPIDEMIOLOGY + CLINICAL PRACTICE
Clinical Practice Uses Population Data:
• Diagnoses are defined and determined from
large groups of patients.
• Prognosis is based on experience of large
groups of patients with the same disease,
stage of disease, and treatments.
• Selection of therapy is based on the results of
large treatment studies, such as clinical trials.
15
EVOLVING FIELD OF EPIDEMIOLOGY
Chief Causes of Death in the U.S. -- 1900
l
l
l
l
l
l
l
Pneumonia/Influenza
Tuberculosis
Gastritis, enteritis, colitis
Heart disease
Senility, ill-defined conditions
Vascular lesions affecting CNS
Nephritis and renal sclerosis
11.8%
11.3%
8.3%
8.0%
6.8%
6.2%
4.7%
16
Chief Causes of Death in the U.S. -- 2001*
l
l
l
l
l
l
l
Disease of heart
Malignant neoplasms
Cerebrovascular diseases
Chronic lower respiratory diseases
Unintentional injuries
Diabetes mellitus
Pneumonia & influenza
248
196
58
44
36
25
22
*Age-adjusted per 100,000
17
Causes of Disease Burden (DALYs)
Worldwide: 2002: Ages 15 - 59
Cause
DALYs (000)
HIV/AIDS
68661
Unipolar depressive disorders
57843
Tuberculosis
28380
Road traffic injuries
27264
Ischemic heart disease
26155
Alcohol use disorders
19567
Hearing loss, adult onset
19486
Violence
18962
18
Causes of Disease Burden (DALYs)
Worldwide: 2002: Ages 60 and Older
Cause
DALYs (000)
Ischemic heart disease
31481
Cerebrovascular disease
29595
COPD
14380
Alzheimers and other dementias
8569
Cataracts
7384
Lower respiratory infections
6597
Hearing loss, adult onset
6548
Trachea, bronchus, lung cancers
5952
19
EVOLVING FIELD OF EPIDEMIOLOGY
l
l
l
Historically, in developed countries, there
has been a marked shift in the leading
causes of mortality from “infectious” to
“chronic” diseases.
In the U.S. today, the fastest growing
segment of the population is aged 85 and
older.
Virtually all “chronic” diseases have
multi-factorial etiologies.
20
Discussion Question 2
If a “cure” was found for heart disease,
how might this likely affect mortality
rates from: (1) AIDS; and (2) Cancer in
the United States?
21
Discussion Question 2
Most likely:
1. AIDS-related mortality would be largely unaffected
since most deaths from AIDS occur in persons not at
high risk (age) for heart disease mortality.
2. Cancer mortality would increase since persons who
would not have died from heart disease would now
be at risk of dying from cancer.
This concept of one cause of mortality affecting
another is know as “competing risks.”
22
THE HOST - ENVIRONMENT INTERACTION
ANKYLOSING SPONDYLITIS
l
l
Persons with HLA-B27 approximately
90 times more likely to develop the
disease (Genetic Susceptibility)
However, only 10% of the individuals
with HLA-B27 will develop the disease
(Environmental Exposure)
23
THE HOST - ENVIRONMENT INTERACTION
“Virtually all chronic diseases have multi-factorial
etiologies” -- many may have infectious components.
Enteroviruses
Epstein Barr virus
Chlamydia pneumoniae
Helicobacter pylori
Hepatitis B and C
Borna disease virus
Type I diabetes
B-cell lymphomas
Heart disease
Peptic ulcers
Liver cancer
Schizophrenia
24
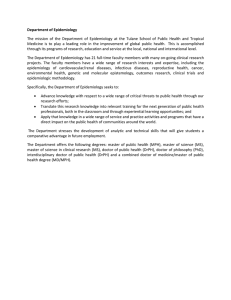
Natural history of disease
Onset of
symptoms
Exposure
Pathologic
changes
Stage of
susceptibility
PRIMARY
PREVENTION
Stage of
subclinical
disease
Usual time
of diagnosis
Stage of
clinical disease
SECONDARY
PREVENTION
Stage of
recovery,
disability or
death
TERTIARY
PREVENTION
25
The natural history of disease
STAGE 1:
Susceptibility
DESCRIPTION:
Risk factors which assist
the development of
disease exist, but disease
has not developed
EXAMPLE:
Smoking
26
The natural history of disease
(cont’d)
STAGE 2:
Presymptomatic disease
DESCRIPTION:
Changes have occurred
to lead toward illness but
disease is not yet
clinically detectable
EXAMPLE:
Alveoli deteriorate
27
The natural history of disease
(cont’d)
STAGE 3:
Clinical Disease
DESCRIPTION:
Detectable signs and/or
symptoms of disease exist
EXAMPLE:
Emphysema detected by
pulmonary function test
28
The natural history of disease
(cont’d)
STAGE 4:
Disability
DESCRIPTION:
Disease has progressed to
the point of causing a
residual effect
EXAMPLE:
Person has difficulty
breathing
29
LEVELS OF PREVENTION
LEVEL:
Primary
DESCRIPTION:
Promote general health
and avoid risk factors for
disease --- Utilize protective
measures to prevent
susceptibility and
presymptomatic disease
EXAMPLE:
Stop smoking or choose
not to start; avoid areas
where people are smoking
30
LEVELS OF PREVENTION
(cont’d)
LEVEL:
DESCRIPTION:
EXAMPLE:
Secondary
Early detection and
timely treatment
Routine pulmonary
function tests for those at
risk; medicine to help
patients breath more
easily; smoking cessation
programs if patient
smokes
31
LEVELS OF PREVENTION
(cont’d)
LEVEL:
Tertiary
DESCRIPTION:
Rehabilitation and
prevention of further
disease or disability
EXAMPLE:
Oxygen therapy;
facilitating ambulation
with technical devices
32
PREVENTION APPROACHES
Population-Based Approach:
• Preventive measure widely applied to an
entire population (public health approach)
• Strive for small absolute change among
many persons
• Must be relatively inexpensive and noninvasive
33
PREVENTION APPROACHES
High-Risk Approach:
• Target group of individual at high risk
• Strive for strong risk factor control
• Often times requires clinical action to
identify the high risk group and to
motivate risk factor control.
34
LEVELS OF PREVENTION (Review)
PRIMARY PREVENTION
Prevention of disease by controlling
risk factors (e.g., non-smoking
promotion)
35
LEVELS OF PREVENTION (Review)
SECONDARY PREVENTION
Reduction in consequences of disease
by early diagnosis and treatment
(e.g., cervical cancer screening)
36
LEVELS OF PREVENTION (Review)
TERTIARY PREVENTION
Reduction in complications of disease
(e.g., MV crashes and ICU)
37
 0
0