High-Magnitude Amblyogenic Factors in school age kids
advertisement

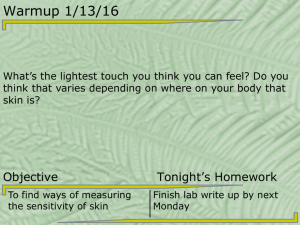
Sensitivity of Photoscreening to Detect High-Magnitude Amblyogenic Factors Sean P. Donahue, MD, PhD,a,b,c Tammy M. Johnson, MPH,a Wanda Ottar, CO, COMT,d and William E. Scott, MDd Purpose: To determine the sensitivity of a unique pupil-size based set of referral criteria of the MTI PhotoScreener (Medical Technology and Innovations, Inc, Cedar Falls, Iowa) to detect high magnitude refractive error. Methods: The photoscreening photographs of 949 preschool children previously analyzed were reevaluated with the new referral criteria. The original photographs had been obtained from pediatricians’ offices and public health and Women, Infants, and Children’s (WIC) clinics. The results of this analysis were compared with the gold standard clinical examination and cycloplegic refraction. Sensitivities were calculated for amblyogenic factors based on the magnitude of the refractive error. Results: For 26 patients with anisometropia, the sensitivity to detect anisometropia increased from 46% for ⫹1.25 or greater spherical interocular difference to 100% for ⫹2.50 spherical intraocular difference. For 36 patients with hypermetropia in at least 1 meridian ranging from ⫹3.75 to ⫹7.50 D, sensitivity increased from 53% to detect ⫹3.75 D or greater to 70% for ⫹5.00 D or greater. The sensitivity to detect hypermetropia of ⫹5.75 D or greater was 100%. These criteria detected 82% of patients with astigmatism greater than or equal to ⫹3.00 D, and 100% of patients with astigmatism greater than ⫹3.50 D. Conclusion: It is crucial that screening programs avoid overreferrals caused by high false-positive screening rates. The sensitivity of our new criteria increases with higher magnitude refractive error; patients with moderate and severe amblyogenic factors are almost never missed. While the sensitivity to detect lower magnitude refractive error is poor, the amblyogenic impact of such errors remains to be determined. (J AAPOS 2002;6:86-91) hotoscreening is receiving increased acceptance as a method of preschool vision screening in spite of legitimate concerns regarding interpretation of photographs and overreferral rates.1,2 The MTI PhotoScreener is an eccentric, off-axis photoscreener that has been tested extensively in various settings3-7 and the field.8 The MTI PhotoScreener detects amblyogenic factors rather than amblyopia, but shows promise for preschool vision screening. Many studies investigating photoscreening with the MTI PhotoScreener have reported sensitivity and specificity values.1-7 In all these studies, the reported sensitivity and specificity depend on the criteria to judge a photo- P From the Departments of Ophthalmology,a Neurology,b and Pediatrics,c Vanderbilt University School of Medicine, Nashville, Tennessee, and the Department of Ophthalmology,d University of Iowa Hospitals and Clinics, Iowa City, Iowa. Presented at the 27th Annual Meeting of the American Association for Pediatric Ophthalmology and Strabismus, Orlando, Florida, March 22, 2001. Supported in part by Research to Prevent Blindness, Inc, New York, New York. Dr Donahue is the recipient of a Career Development Award from Research to Prevent Blindness, Inc. The study was conducted at Vanderbilt University Medical Center. Submitted April 2, 2001. Revision accepted October 19, 2001. Reprint requests: Sean P. Donahue, MD, PhD, Department of Ophthalmology and Visual Sciences, Vanderbilt University School of Medicine, 8000 Medical Center East, Nashville, TN 37232-8808. Copyright © 2002 by the American Association for Pediatric Ophthalmology and Strabismus. 1091-8531/2002/$35.00 ⫹ 0 75/1/121168 doi:10.1067/mpa.2002.121168 86 April 2002 graph abnormal (referral criteria) and the criteria to call a clinical examination finding abnormal (failure criteria) in addition to the person interpreting the photograph. Because photoscreening detects amblyogenic factors rather than amblyopia, and since many children with amblyogenic factors may never develop amblyopia, criteria both for referral and failure may differ significantly between studies but still be valid, depending on the screening situation. Nevertheless, a universal factor for all referral criteria should be a progressively increasing sensitivity to detect amblyogenic factors of higher magnitude, since they are more likely to be amblyogenic. We have been developing and refining a volunteer-led vision screening program for preschool children. Our statewide screening program uses lay volunteers from local Lions Clubs, a photograph reading center, and a network of optometrists and ophthalmologists in the child’s local community. Because we were concerned that a high referral rate and the resulting high false-positive rate could jeopardize the reputation of this volunteer-led program in the minds of community physicians, we developed unique criteria for referral. These criteria produced a referral rate of approximately 5.4% and a predictive value positive of approximately 70%, after screening 45,000 preschool children. Details regarding this program have been published elsewhere.8 Although we have published data regarding the referral rate and predictive value positive for these referral criteria, Journal of AAPOS Journal of AAPOS Volume 6 Number 2 April 2002 Donahue et al TABLE 1. Vanderbilt University photoscreening referral criteria 1. Any strabismus 2. Media opacity ⬎1 mm 3. Refractive error for: 4 mm pupillary diameter 6 mm pupillary diameter a. Myopic crescent ⱖ 2.5 mm Myopic crescent ⱖ 4.5 mm b. Hyperopic crescent ⱖ 2.5 mm Hyperopic crescent ⱖ 4.5 mm c. Astigmatism ⬎ 1.5 mm Astigmatism ⬎ 2.0 mm d. Anisometropia: No crescent in fellow eye: Crescent ⱖ 2.0 mm Crescent ⱖ 3.5 mm e. Anisometropia: Crescent in fellow eye: ⱖ1 mm crescent in fellow eye 1) ⱕ2.5 mm crescent in fellow eye 1 mm difference between eyes 2 mm difference between eyes 2) ⱖ 3 mm crescent in fellow eye 1 mm difference between eyes we have not reported sensitivity data. Obtaining such data with adequate confidence intervals would require comprehensive eye examinations with cycloplegic refraction on large numbers of children, and our program does not have the resources to do that. Instead, we obtained the photoscreening photographs from 949 previously reported children, who were photoscreened and who had a comprehensive eye exam, and whose results were used in determining initial sensitivities for the MTI PhotoScreener.3 We sought to determine the sensitivity of our referral criteria to detect various types of amblyogenic factors. We also determined the sensitivity of these criteria to detect refractive error of increasing magnitude. METHODS Subjects Data regarding the subjects used in this study have been reported previously.3 They come from a data set of 1003 healthy children between the ages of 6 months and 59 months who were examined during routine vision screening at Public Health, and Women, Infants, and Children’s (WIC) clinics in Iowa and Illinois, and from children evaluated in private offices of pediatricians in Iowa and Texas. Although the relative distribution of pathology for these children had been reported, in this study, the photographs were evaluated by trained readers in a masked fashion without having access to the results of the comprehensive eye examination and cycloplegic refraction. (The staff at the Vanderbilt Ophthalmic Imaging Center (VOIC) was not familiar with photoscreening literature and had not read the previous report by Ottar et al.3) All photographs were evaluated at the VOIC. Photographs were first determined to be readable or unreadable. Unreadable photographs had a pupil size smaller than 4 mm or lack of fixation on the camera. Once the determination of a readable photograph was made, the referral criteria shown in Table 1 were applied. All photographs were first interpreted by VOIC staff and then by 2 of the authors (S.P.D. and T.M.J.). A consensus of all 3 was necessary before a final grading was given. (Currently all 87 8 mm pupillary diameter Myopic crescent ⱖ 6.5 mm Hyperopic crescent ⱖ 6.5 mm Astigmatism ⬎ 2.5 mm Crescent ⱖ 4 mm 1) ⱕ3.5 mm crescent in fellow eye 2 mm difference between eyes 2) ⱖ 4 mm crescent in fellow eye 1 mm difference between eyes photographs that are referred or considered unreadable by VOIC staff are also reviewed by both S.P.D. and T.M.J., and a consensus is required prior to making a formal reading.) When several amblyogenic factors were present, the amblyogenic factors were ordered as to the most significant diagnosis (media opacity ⬎ strabismus ⬎ anisometropia ⬎ hyperopia ⬎ myopia ⬎ astigmatism). Anisometropia was determined by comparing across meridians. (When astigmatism was present in only 1 eye, it was considered to be anisometropia). Because only 3 patients had strabismus on the formal exam, these were later excluded from analysis except for their refractive errors. No patients had media opacity. No patients had myopia without also having superimposed anisometropia or astigmatism. Therefore, for this study patients were categorized into 3 groups based on the primary refractive problem: (1) anisometropia, (2) hypermetropia, and (3) astigmatism, in that order of diagnosis. In addition to the sensitivity for the primary diagnosis, we also calculated sensitivities for patients with anisometropia, hypermetropia, or astigmatism without regard to the primary diagnosis (ie, a patient with anisometropia and hyperopia is given a primary diagnosis of anisometropia, but is also included in the hyperopia group). It should be noted that the flash on the MTI photoscreener is oriented so as to detect meridional astigmatism; a significant limitation of this instrument is the relative inability to detect oblique astigmatism. We also determined the sensitivity to detect various magnitudes of each amblyogenic factor. For purposes of classification, we used the criteria for examination failure listed in Table 2. These criteria were derived from a survey of pediatric ophthalmologists9 and were the exam failure criteria used for previous reports regarding this program.8,10 TABLE 2. Criteria for failure of clinical eye examination 1. Anisometropia ⬎ 1.00 D 2. Astigmatism ⬎ 1.50 D 3. Hypermetropia ⬎ 3.50 D 4. Myopia ⬎ ⫺3.00 D 88 Journal of AAPOS Volume 6 Number 2 April 2002 Donahue et al TABLE 3. Sensitivity to detect anisometropia Amount* N Passed Referred ⫹1.25 ⫹1.50 ⫹2.00 ⫹2.50 ⫹3.00 ⫹3.50 Total Sph Sph Sph Sph Sph Sph 5 12 6 1 1 1 26 3 10 1 0 0 0 14 Sensitivity† 2 2 5 1 1 1 12 46% 48% 89% 100% 100% 100% *Inter eye difference in refractive error in greatest meridian. †Sensitivity to detect amblyogenic factor of this or greater magnitude. RESULTS Photo Interpretation The original Iowa data set had 978 patients. We excluded 39 photographs because of a small pupillary diameter or difficulty obtaining a photoscreening photograph or clinical information. Of the 939 patients with interpretable photographs and examination results, 88 had significant abnormalities. Twenty-six met the clinical criteria for primary anisometropia (⬎1.00 D), 40 met the clinical criteria for primary astigmatism (⬎1.50 D) and 22 met the criteria for primary hypermetropia (⬎3.5 D in 1 meridian). However, because many patients with anisometropia also had hypermetropia or astigmatism in 1 meridian, and many patients with astigmatism had significant hypermetropia in 1 meridian, several patients could be categorized into multiple diagnostic groups. When classified in this manner, 51 children had astigmatism, 36 had hypermetropia, and 26 had anisometropia. Overall, the sensitivity for amblyogenic factors of all magnitudes (Table 2) was 50% and the specificity was 98.5%. The negative predictive value was 94.4% and the positive predictive value was 57.5%. Sensitivity to Detect Anisometropia Twenty-six patients had anisometropia greater than 1.00 D detected on the clinical examination and cycloplegic refraction. The distribution of anisometropic refractive errors is listed in Table 3. Of the 5 patients with anisometropia of 1.25 D, 3 were passed by the VOIC while 2 were referred. Of the 12 patients with ⫹1.50 D anisometropia, 10 were passed and 2 were referred. One patient was referred for suspected myopia and had it confirmed on the examination (along with the anisometropia), and 1 patient was referred with suspected hypermetropia. For the 9 patients having anisometropia of 2 D or greater, sensitivity improved substantially. Six patients had anisometropia of 2 D. Of these patients, 5 were referred and only 1 was passed by the VOIC. The patients with ⫹2.50 D, ⫹3.00 D, and ⫹3.50 D anisometropia were all appropriately referred. In summary, the sensitivity to detect 1.25 D or greater anisometropia was 46%. However, the sensitivity to detect 2.00 D or greater anisometropia was 89%. TABLE 4. Sensitivity to detect hypermetropia Amount (D) N Pass Refer ⫹3.75 ⫹4.00 ⫹4.25 ⫹4.50 ⫹5.00 ⫹5.25 ⫹5.50 ⫹5.75 – ⫹6.00 ⬎ ⫹6.00 Total Sensitivity 2 6 1 7 3 3 8 3 1 3 1 6 1 1 4 0 1 3 0 1 2 2 4 3 53% 53% 54% 55% 70% 71% 71% 100% 3 36 0 17 3 19 100% *Sensitivity to detect amblyogenic factor of this or greater magnitude. Sensitivity to Detect Hypermetropia Thirty-six patients met the clinical criteria for hypermetropia (⬎3.5 D). Of these, 14 patients had astigmatism or anisometropia, with hypermetropia in 1 axis of 1 eye greater than 3.5 D, while 22 had hypermetropia without anisometropia or astigmatism. Of these 36 patients, 17 were passed by the VOIC, whereas 19 were referred (Table 4). The 17 patients who were passed had hypermetropia ranging from ⫹3.75 D to ⫹5.50 D. The 19 patients who were referred had hypermetropia ranging from ⫹3.75 D to ⫹7.50 D. The sensitivity to detect ⫹4.00 D or more hypermetropia in at least 1 meridian was 53%. However, the sensitivity to detect ⫹5.00 D or greater of hypermetropia was 70%, while the sensitivity to detect greater than ⫹5.50 D of hypermetropia was 100%. Six patients with refractive error of at least ⫹5.00 in 1 meridian were missed (falsenegatives). Patients having hypermetropia along with astigmatism or anisometropia were more likely to be detected than those with hypermetropia alone. Of the 8 patients with hypermetropia and astigmatism (hyperopia ⬎ ⫹3.50 D in at least 1 meridian), 5 were referred. Of 6 patients with anisometropia and hypermetropia, 4 were referred. However, this may reflect a sampling bias as patients with hypermetropia and either astigmatism or anisometropia had higher levels of hypermetropia in 1 axis than did those with spherical symmetric hypermetropia. Sample size limitations precluded us from making this comparison more directly. Sensitivity to Detect Astigmatism Forty patients met the clinical criteria for primary astigmatism (⬎1.50 D in 1 meridian without concomitant anisometropia or hyperopia). An additional 11 patients had astigmatism, but with a primary diagnosis of anisometropia (n ⫽ 11). Thus, 51 children were considered to have astigmatism for the purpose of this study. Of these 51 children, 29 were referred by the VOIC and 22 were passed. The distribution of the astigmatism is listed in Table 5. Journal of AAPOS Volume 6 Number 2 April 2002 TABLE 5. Sensitivity to detect astigmatism Amount of astigmatism N Pass ⫹1.75 ⫹2.00 ⫹2.25 ⫹2.50 ⫹2.75 ⫹3.00 ⫹3.50 ⫹4.00 ⫹4.50 ⫹6.00 Total 11 13 1 14 1 3 4 1 2 1 51 7 7 0 5 1 1 1 0 0 0 22 Donahue et al Refer Sensitivity 4 6 1 9 0 2 3 1 2 1 29 57% 63% 70% 69% 75% 82% 88% 100% 100% 100% *Sensitivity to detect factor of this or greater magnitude. As the magnitude of astigmatism increased, the criteria became more sensitive to detect it. The sensitivity to detect astigmatism greater than 1.50 D was 57%, but increased to 70% for astigmatism greater than 2.00 D. The sensitivity to detect 3.00 D or greater of astigmatism was 82%. These criteria detected 7 of the 8 children with astigmatism of ⫹3.50 D and all 4 children with astigmatism greater than or equal to 4.00 D (100%). There was no difference in sensitivity for the 40 patients with primary astigmatism (23 referred) compared with the 11 with astigmatism associated with anisometropia (6 referred). DISCUSSION Screening for amblyogenic factors is inherently different than most other types of health screening, because photoscreening identifies risk factors for a disease rather than the disease itself. It is more similar to using cholesterol levels to detect heart disease than it is to using mammography to detect breast cancer. Photoscreening must have a high sensitivity to detect the highest magnitude amblyogenic factors, but also needs to have a low false-positive rate. The perils and excessive costs associated with high false-positive referral rates in photoscreening have been well-documented by Simons et al.1 When we designed our program, we were keenly aware of the effect that a high false-positive rate would have on the reputation of a volunteer-led program with respect to primary care physicians, parents, and the volunteers themselves. Our pilot studies had demonstrated a referral rate that approached 15% when the manufacturer’s criteria were used to interpret MTI photographs. In addition, we recognized that in-the-field interpretation of photoscreening photographs by lay volunteers would present a massive quality control problem. All of these concerns have been documented since that time.1,2 Therefore, we designed a unique grading system that used a pupil-based referral criteria and a centralized reading center to deal directly with these issues.8 Our photoscreening program has screened more than 45,000 preschool children (ages 6-48 months) in the state 89 of Tennessee using the MTI PhotoScreener, lay volunteers, and optometrists and ophthalmologists in the children’s local areas. Our current rate of follow-up has averaged more than 70%, and for the last 6 months of calendar year 2000 exceeded 90% (For comparison, the immunization rate in Tennessee is 74%). Our current referral rate averages 5.4% and our predictive value positive is nearly 70% (a 30% false-positive rate). However, in spite of our high predictive value and low referral rate, we did not know how well our criteria detected high magnitude refractive errors compared with those of moderate magnitude. Rather than perform such a study in the field, which would require significant resources, we applied our criteria to a previously studied group of children who had photoscreening photographs done using the MTI PhotoScreener and cycloplegic refractions by a trained orthoptist. Our results demonstrate that while we have only fair sensitivity to detect small magnitude refractive error, the sensitivity increases with the magnitude of the refractive error. In our study, no children with anisometropia greater than 2.00 D, no patients with astigmatism greater than 3.50 D, and no patients with hypermetropia greater than 5.50 D were missed. We recognize that the small sample size for these high refractive error groups limits conclusions about the exact sensitivity for these groups, but are confident that these criteria detect the vast majority of potentially amblyopic children without producing a large number of false-positive referrals. Clearly, further studies need to investigate larger numbers of patients with higher magnitude refractive error. Most patients with anisometropia of 1.50 D or less were not detected using these criteria. However, it should be noted that anisometropia of this magnitude is likely not associated with more than a mildly increased risk for the development of amblyopia. Kutschke et al11 found that only 6 of 124 patients with anisometropic amblyopia had anisometropia less than 1.5 D, and all of these had manifest strabismus. Because the patients in this study with low levels of anisometropia were all orthotropic, it is not likely that they will develop amblyopia. Ottar et al3 noticed an increased sensitivity of the manufacturer’s criteria to detect larger magnitude anisometropia in this patient group; those criteria detected 84% of anisometropia greater than 1.5 D. Moderate degrees of hypermetropia were not detected reliably under the noncycloplegic conditions of photoscreening. While this is concerning given the increased risk of strabismus developing in patients with uncorrected hyperopia,13 the natural history of moderate levels of hypermetropic refractive error in children who do not develop accommodative esotropia is unknown. We believe that a child with mild to moderate hypermetropia who accommodates without developing strabismus is likely at minimal risk for developing amblyopia. In contrast, the child with very high hypermetropia (⫹6.00 D or ⬎) is at 90 Donahue et al greater risk of developing either accommodative esotropia or refractive amblyopia, and must be detected with screening. We detected all 6 children with hypermetropia in any meridian greater than ⫹5.50 D. Tong et al12 have recently proposed guidelines for the detection of hypermetropia with the MTI PhotoScreener and we are currently prospectively comparing their guidelines to those reported here. Most of the false-negative hyperopic children in this study were likely missed because they remained orthotropic while accommodating partially or fully on the camera fixation light. This problem has been discussed previously by Ottar et al.3 A significant problem with photoscreening for hypermetropia is that, in the absence of accommodation, crescents become so large with ⫹3.00 D of uncorrected hypermetropia that additional increments of hypermetropia produce little additional incremental increase in crescent size.14 It is unknown whether children who fail to accommodate this degree at the time of photoscreening are at greater risk for developing amblyopia than those who do accommodate. Further research into mechanisms to detect latent hypermetropia with photoscreening and into the natural history of moderate degrees of hypermetropia on the development of amblyopia are warranted. It is somewhat surprising that we were able to detect moderate levels of astigmatism so well. This is even more surprising in that similar levels of hypermetropia could not be detected. We believe this is likely due to our criteria for the detection of astigmatism, which require smaller crescents than do those for hypermetropia. However, a tradeoff of this increased sensitivity is a decrease in predictive value positive; our predictive value for the suspected diagnosis of astigmatism is in the range of 42%, whereas that for hypermetropia approaches 80%.7 An additional limitation of photoscreening with the MTI PhotoScreener is that it is theoretically unable to detect oblique astigmatism bilaterally (unilateral oblique astigmatism will be revealed as anisometropia). No patients in this study had significant oblique astigmatism, because of its rarity. Nevertheless, an optimal screening instrument must be able to detect it. The biggest limitation of this study is that the study group refractions were performed by the same person who did the photoscreening. This represents a potential bias that could not be overcome without reproducing the entire study. We interpreted all photographs, however, prior to receiving examination results on these children and therefore were masked to their examination findings at the time of photograph interpretation. Many sets of criteria have been proposed to determine referral and failure criteria for photoscreening. This has been termed a problem of a “moving goal post.” While having several sets of referral criteria appears bothersome from a standpoint of research and standardization, it clearly is beneficial in some settings. In remote, sparsely populated areas, it is very expensive to bring a child with a suspected eye problem in for a formal eye examination. In Journal of AAPOS Volume 6 Number 2 April 2002 Alaska, for example, the child often needs to be flown to the examination location with his or her parents.15 This is much different than the situation in urban areas, where the costs associated with a false-positive overreferral are much less. We were aware of the problems that a low predictive value positive would bring to the reputation of a volunteer-led program, and therefore developed stringent referral criteria. Other programs having less need to control false positives may choose a less stringent set of referral criteria. Photoscreening will continue to have a role in detecting amblyogenic factors prior to the onset of literacy. Further refinements in vision screening technology will likely produce digital cameras and digital analysis systems.16 However, problems with the control of accommodation and the over-detection of astigmatism will continue to exist. Further research is needed to continue to refine referral criteria, determine the natural history of various levels of amblyogenic factors, and identify children who need intervention on the basis of their refractive error. It should also be remembered that the efficacy of photoscreening, while now quite well established in the ophthalmic literature, is not well documented when compared with traditional vision screening, because most traditional vision screening techniques have never been adequately validated in the field. It is only through further investigation that the knowledge to support a preschool vision screening mandate will develop. References 1. Simons BD, Siatkowski RM, Schiffman JC, Berry BE, Flynn JT. Pediatric photoscreening for strabismus and refractive errors in a high-risk population. Ophthalmology 1999;106:1073-80. 2. Tong PY, Enke-Miyazaki E, Bassin RE, Tielsen JM, Stager DR Sr, Beauchamp GR, et al. Screening for amblyopia in preverbal children with photoscreening photographs. National Children’s Eye Care Foundation Vision Screening Study Group. Ophthalmology 1998; 105:856-63. 3. Ottar WL, Scott WE, Holgado SI. Photoscreening for amblyogenic factors. J Pediatr Ophthalmol Strabismus 1995;32:289-95. 4. Weinand F, Gräf M, Demming K. Sensitivity of the MTI Photoscreener for amblyogenic factors in infancy and early childhood. Graefes Arch Clin Exp Ophthalmol 1998;236:801-5. 5. Lewis RC, Marsh-Tootle WL. The reliability of interpretation of photoscreening results with the MTI PS-100 in Headstart school children. J Am Optom Assoc 1995;66:429-34. 6. Holgado SI, Arfeli S, Gomez-Demmel E, Espinosa J. Comparative study of the MTI Photoscreener,™ visual acuity, and Lang stereopsis test for amblyogenic factors in mentally delayed children. Am Orthoptic J 1998;48:122-30. 7. Tong PY, Bassin RE, Enke-Miyazaki E, Macke JP, Tielsch JM, Stager DR, et al. Screening for amblyopia in preverbal children with photoscreening photographs II. Ophthalmology 2000;107:1623-9. 8. Donahue SP, Johnson TM, Leonard-Martin TC. Screening for amblyogenic factors using a volunteer lay network: initial results from a statewide program targeting preliterate children. Ophthalmology 2000;107:1637-44. 9. Miller JM, Harvey EM. Spectacle prescribing recommendations of AAPOS members. J Pediatr Ophthalmol Strabismus 1998;35:51-2. 10. Donahue SP, Johnson TM. Age-based refinement of referral criteria for photoscreening. Ophthalmology 2001;108:2309-14. Journal of AAPOS Volume 6 Number 2 April 2002 Donahue et al 11. Kutschke PJ, Scott WE, Keech RV. Anisometropic amblyopia. Ophthalmology 1991;98:258-63. 12. Tong PY, Macke JP, Bassin RE, Everett M, Enke-Miyazaki E, Tielsch JM, et al. Screening for amblyopia in preverbal children with photoscreening photographs III. Ophthalmology 2000;107:1630-6. 13. Atkinson J, Braddick O, Robier B, Anker S, Ehrlich D, King J, et al. Two infant vision screening programmes: prediction and prevention of strabismus and amblyopia from photo- and videorefractive screening. Eye 1996;10:189-98. 91 14. The MTI Photoscreener Instruction and Interpretation Manual. Cedar Falls, IA: Medical Technology, Inc, 1994. 15. Arnold RW, Gionet EG, Jestrzebski AI, Kovtoun TA, Machida CJ, Armitage MD, et al. The Alaska Blind Child Discovery Project: rationale, methods and results of 4000 screenings. Alaska Med 2000; 42:58-72. 16. Granet DB, Hoover A, Smith AR, Brown SI, Bartsch DU, Brody B. A new objective digital computerized vision screening system. J Pediatr Ophthalmol Strabismus 1999;36:251-6. An Eye on the Arts – The Arts on the Eye The Song of the Blindman I am blind, you out there—that is a curse, against one’s will, a contradiction, a heavy daily burden. I lay my hand on the arm of my wife, my grey hand upon her greyer grey, as she guides me through empty spaces. You move about and stir, and imagine your sounds differing from stone to stone. But you are mistaken; I alone live and suffer and complain, for in me is an endless crying, and I do not know whether it is my heart that cries or my bowels. Do you recognize these songs? You never sang them, not quite with this intonation. For you every morning brings its new light warm through your open windows. And you have the feeling from face to face that tempts you to be indulgent. —Rainer Maria Rilke (translated by Albert Ernest Flemming)