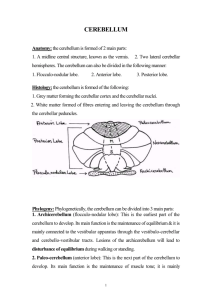
ATAXIA By Dr. Heba A. Metwally Anatomy and physiology of cerebellum Cerebellar disorders (Ataxia): defintion, clinical features, types. Problems of ataxic patients Physical management of ataxia A)Assessment B) treatment ANATOMY AND PHYSIOLOGY OF CEREBELLUM Anatomy: Cerebellum lies behind the brainstem and occupies most of the posterior cranial fossa. It is attached to the brain stem by 3 pairs of tracts called the cerebellar peduncles which connect the cerebellum with other centers in the CNS. It is composed of Gray matter → forming the Cerebellar cortex, Deep cerebellar nuclei (Dentate, Interposed and Fastigial nuclei). White matter → formed of fibers entering and leaving the cerebellum through the cerebellar peduncles Dentate nucleus Interposed nucleus Fastigial nucleus ANATOMY AND PHYSIOLOGY OF CEREBELLUM ♦ Anatomy It is divided (by 2 fissures; 1ry and posterolateral fissure) into 3 prominent anatomical lobes: A. The anterior lobe. B. The posterior lobe. C. The flocculonodular lobe. The anterior and posterior lobes are divided into longitudinal zones; a) Vermal zone → occupies the vermis. b) Intermediate (or paravermal) zone → lying on each side of the vermis, occupying the medial regions of the cerebellar hemispheres. c) Lateral zone of the cerebellar hemisphere → lying just lateral to the intermediate zone. ANATOMY AND PHYSIOLOGY OF CEREBELLUM It 1. 2. 3. is divided into 3 major functional divisions; Vestibulocerebellum→ composed of the "flocculonodular lobe“→ connected to vestibular apparatus. Spinocerebellum → composed of the vermis and paravermal zone→ connected to spinal cord. Cerebrocerebellum→ composed of lateral zones of the cerebellar hemispheres→ connected to cerebral hemispheres. FUNCTIONS OF THE CEREBELLUM 1. Regulation of Equilibrium. 2. Maintenance of tone. 3. Regulation (or Coordination) Voluntary Movements. 4. Motor learning. of FUNCTIONS OF THE CEREBELLUM 1. Regulation of Equilibrium. Through connections with vestibular apparatus, cerebellum helps to maintain equilibrium during the change in head position, and during exposure to acceleration or active movements of the body Lesion leads to disturbances in equilibrium during standing and walking 2. Maintenance of tone. Through connections with spinal cord, cerebellum regulates the tone and contraction of the axial and proximal limb ms. Lesion leads to hypotonia. FUNCTIONS OF THE CEREBELLUM 3. Coordination of Voluntary Movements. Through connections with cerebral hemispheres, cerebellum coordinate voluntary movements Defintion of coordination: it is the ability to use the right muscle at right time with proper intensity to reach certain goal. Coordination of movements means one's ability to proceed smoothly and precisely from one movement to the next in proper succession. FUNCTIONS OF THE CEREBELLUM 3. Coordination of Voluntary Movements: The cerebellar role in coordination of movements is carried out by a No. of mechanisms, including:a) Comparator and Error- Correction Mechanism. b) Damping Mechanism. c) Planning the Sequence and Timing of Movements FUNCTIONS OF THE CEREBELLUM 3. Coordination of Voluntary Movements: a) Comparator and Error- Correction Mechanism. When the motor areas of the CC send motor commands to ms for performance of a voluntary movement, the cerebellum receives immediately an "efference copy" of the intended motor command As the movement proceeds, the cerebellum receives proprioceptive signals about the actual motor performance. Cerebellum acts as a "comparator" that compares the motor intentions of the higher centers with the actual performance of the involved ms. When there is any "error" in performance or "deviation" from the original plan of the intended voluntary motor act, then the cerebellums send 'corrective signals" back to the motor areas of the CC →ms. Corrective signals Plan of motor act• Actual performance • FUNCTIONS OF THE CEREBELLUM 3. Coordination of Voluntary Movements: b) Damping Mechanism. All movements of the body tend to overshoot due to momentum. The cerebellum sends braking signals to stop the movement at intended point, thereby preventing the overshoot. If the cerebellum is damaged, the cerebral cortex will recognize the overshooting only after it occurs and corrects it, this leads to oscillation of the limb around the intended point i.e. intention kinetic tremor. FUNCTIONS OF THE CEREBELLUM 3. Coordination of Voluntary Movements: c) Planning the Sequence and Timing of Movements: a) A) Planning: cerebellum receives signal from the cortical association areas before the start of movement. it then provides the plan of the next movement without being involved at all at the present movement. B) Timing ( predictive): cerebellum provides perfect timing of voluntary movements. This is established by computing (calculating) the appropriate timing for the "onset" and "termination" of contraction of each of the ms involved in the performance of the successive movements during voluntary motor acts → assures the smooth progression of the whole movement. FUNCTIONS OF THE CEREBELLUM 4. Motor learning: When a person first performs a complex motor act, the degree of cerebellar adjustment of movements is almost always inaccurate, then cerebellar neuronal circuits learn to make more accurate movement the next time. Thus, after the motor act has been repeated many times (motor training), the successive steps of the motor act become gradually more precise. Once the cerebellum has perfectly learned its role in different patterns of movements, it establishes a specific "stored program" for each of the learned movements (feed-forward) Feed-forward: means that cerebellum programs or models voluntary movement skills based on memory of pervious sensory input and motor output. These movements include writing, typing, talking, running, and many other athletic and professional motor skills. These movements occur so rapidly that it is almost impossible to depend for their control on the sensory feed-back information from the periphery, because the movement would be over before such information reaches the cerebellum and the cerebral cortex. These movements are referred to as "ballistic" movements (ballistic is a word meaning "thrown"), because once the movement goes on there is no way to modify its present course by any sensory feed-back control mechanism. CEREBELLAR DISORDERS (ATAXIA): Definition: Ataxia is incoordination of voluntary motor activity with or without dis-equilibriation in the absence of motor weakness. Cerebellar syndromes (Main clinical features): a) Archicerebellum= vestibulocerebellum syndrome: It is manifested by:1) Swaying during standing, with a tendency to fall down. 2) Unsteady (staggering) gait→ wide-based in order to provide better equilibrium during walking CEREBELLAR DISORDERS (ATAXIA): Cerebellar syndromes (Main clinical features): b) Paleocerebellum=spinocerebellum syndrome: It is manifested by: Hypotonia and hyporeflexia that occur also in both Archicerebellar and Neocerebellar syndromes CEREBELLAR DISORDERS (ATAXIA): Cerebellar syndromes (Main clinical features): c) Neocerebellum= cerebro cerebellum syndrome: It is manifested by: Hypotonia and hyporeflexia Asthenia Incoordination; - 1) Dysmetria→ inability to judge (errors) in the range and direction of the movement (hypometria or hypermetria) - 2) Intention Tremors (Kinetic Tremors): They appear when the patient performs a voluntary motor act, not seen when the ms are at rest. N.B: patients has head nodding, trunk titubation and intention kinetic tremors of extremities. CEREBELLAR DISORDERS (ATAXIA): 3) Decomposition of Complex Movements: The motor act is carried out as several fragmented steps rather than a smoothly progressing movement. For instance, in reaching for an object by the hand, the cerebellar patient may first move the shoulder joint, then the elbow, followed by the wrist and fingers → simulate movements of a "robot". 4) Rebound Phenomenon The cerebellar patient is unable to stop the ongoing movement rapidly due to failure of the damping functions of the cerebellum. This can be observed in what is called "rebound phenomenon". When there is a flexion of the forearm against resistance (provided by the examiner's hand), the cerebellar patient cannot stop the resultant inward movement of his limb in due time following its release, and the forearm flexes forcibly and may strike his body with considerable violence. CEREBELLAR DISORDERS (ATAXIA): 5) Dysdiadochokinesia • Dysdiadochokinesia → inability of the patient to perform rapid alternating opposite movements e.g. rapid repetitive pronation and supination of forearm. The movements are slow and irregular. • It results from failure to adjust precisely the proper timing for the onset and termination of the successive alternating contractions of the opposing ms groups. 6) Nystagmus Nystagmus of cerebellar disorders is a tremor of the eye balls as a result of "dysmetria" of the "saccadic movements" of the eyes. CEREBELLAR DISORDERS (ATAXIA): 7) Dysarthria: Staccato speech →slow, explosive, interruptive speech. Or scanning speech →slow and decomposed speech. Decomposition of words is due to failure to adjust the precise timing of contraction of the different ms of speech. 8) Unsteady Gait The gait is unsteady and broad-based due to dysmetria and kinetic tremors of the lower limb ms. Unilateral Mild lesion→ deviation toward same side of lesion Bilateral mild lesion → zigzag gait. Unilateral sever lesion→ wide base gait Bilateral sever lesion → drunken gait. CEREBELLAR DISORDERS (ATAXIA): Types: Cerebellar ataxia Sensory ataxia Vestibular ataxia Combined ataxia CEREBELLAR ATAXIA CEREBELLAR ATAXIA Friedreich ataxia Heridofamilial, occurs 1st decade of life. Pathologically there is degeneration in Archicerebellum mainly------- Ataxia. Pyramidal tracts-------- +ve Babiniski sign Posterior column-----lost deep sensation, diminshed reflexes Peripheral neuropathy----stock and glove hypoesthesia Other features :skeletal deformities e.g. pes cavus, scoliosis and ♥cardiomyopathy. SENSORY ATAXIA Definition: It is ataxia due to loss of the proprioceptive (deep) sensations, at any point in their pathway (see fig. 9). Causes: Peripheral nerve: peripheral neuropathy specially diabetic, alcoholic and nutritional. Posterior root: tabes dorsalis. Posterior column: subacute combined degeneration of the cord. Medial lemniscus: brain stem lesions. Thalamus: thalamic syndrome. Cortical sensory area: parietal lobe lesions. SENSORY ATAXIA Clinical picture: Kinetic tremors appear only on closure of the eyes. Rhomberg's test: when the patient stands with his feet close together & his eyes closed, his body sways & he may fall if not supported. Stamping gait: heavy strike of the ground on walking due to lost deep sensation. Deep sensory loss. Hypotonia Hyporeflexia VESTIBULAR ATAXIA Definition: It is ataxia due to lesions of the vestibular division of the vestibulocochlear nerve . Causes: Meniere's disease. Labyrinthitis. Acoustic neuroma. Clinical picture: Vertigo, tinnitus, deafness & vestibular nystagmus. Problems of movement regulation expressed as error in rate, range, direction and force. Balance reactions are inappropriate and slow to be initiate . Difficulty in adapting posture to changing condition. Lack of the normal regulation and graduation of muscle contraction necessary for all movement and posture excess of motion Instability around shoulder interfere with: a) control of the arm b) manipulation of object at a distance from him. Instability around pelvis interfere with the control of the pelvis of the extended leg. Difficulty in regulating small ranges of mov + intention tremor lead to problems with manipulation activities Poor visual fixation and eye hand contact due to ataxic arm movement, nystagmus and voluntary restriction of head movement Orofascial dysfunction Poor posture Subnormal ADL Secondary problems as respiratory, circulatory and deformity may occur in sever cases. Gait problems hypermetria manifest itself by raising the feet to an unnecessary high level above the ground. decomposition result in lag of the trunk to be moved forward with the movement of the leg with a tendency to fall backward. MANAGEMENT OF ATAXIA Assessment: Some important points must be considered as: Assessment and evaluation of both sides of the body must be done even if unilateral lesion of cerebellum has been diagnosed. Assessment and evaluation of the patient must be done in quite place to prevent distraction, considering age of the patient, and his psychological status to gain full cooperation from him. Assessment and evaluation of functional activities must include: - Assistance needed - Time to complete activity - Level of effort involved - Potential hazards MANAGEMENT OF ATAXIA Assessment: Some important points must be considered as: Assessment and evaluation of posture and ROM are very important because the possibility of presence of congenital deformities. Assessment and evaluation of coordination, considering the components of movements ( response orientation, control, speed,…etc). Evaluation of gait, ask the patient firstly to walk slowly then change directions with different speeds. Patient’s progress in ambulation can be determined by the numbers they loose their balance in treatment session, frequency of a specific errors, the distance ambulated or the level of assistance needed. Assessment of ataxic patients - Motor assessment including muscle tone and muscle test, reflexes and ROM. - Sensory assessment including superficial and deep sensation - Orofacial function assessment including facial expression, lip & jaw closure….etc. - Coordination of respiration with swallowing and speech. Gait assessment - International Cooperative Ataxia Rating Scale (Evaluating truncal and extremity ataxia, gait ataxia, nystagmus and talking) Assessment of ataxic patients - Coordination assessment (the most important item) including equilibrium and non equilibrium subtypes. - Equilibrum coordination tests stastic and dynamic balance. - Non equilibrum coordination tests focus on assessment of movement capabilities in four main areas: 1- Alternate or reciprocal motion. 2- Movement composition, or synergy. 3- Movement accuracy. 4- Fixation, or limb holding. Movement Capabilities The non-equilibrium coordination examination focuses on movement capabilities in several main areas: • Alternate or reciprocal motion, which is the ability to reverse movement between opposing muscle groups • Movement composition, or synergy, which involves movement control achieved by muscle groups acting together • Movement accuracy, which is the ability to gauge or judge distance and speed of voluntary movement • Fixation or limb holding, which addresses the ability to hold the position of an individual limb or limb segment ASSESSMENT OF NON EQUILIBRIUM COORDINATION It includes specific tests In upper limb: Finger to nose test Finger to finger test Finger to Doctor finger test Adiadokokinesia Rebound phenomena In lower limb: Heel to knee test Walking along a straight line (tandom) Romberg test ASSESSMENT OF NON EQUILIBRIUM COORDINATION ASSESSMENT OF NON EQUILIBRIUM COORDINATION THE GOALS OF RESTORATIVE PHYSICAL TREATMENT CAN BE BRIEFLY DESCRIBED AS: Long term goal: - To make the patient functional as much as possible with maximum safety and less energy cost. Short term goals:1. To improve the background of movement by improving proximal control, stability, and postural reactions. 2. To regulate the interplay between two muscle groups. 3. To reduce tremor. 4. To improve visual fixation and eye hand contact. 5. To improve orofacial problems. 6. To improve gait problems. TREATMENT: 1-Methods to improve proximal instability : Approximation Rhythmic Stabilization: - It is simultaneous isometric contraction of agonist and antagonist. Alternative isometric technique. It is an isometric contracrion of antagonist followed by isometric contraction of agonist. Tonic holding Weight bearing position as quadruped position and maintain it for 20 minutes. TREATMENT: 2- Methods to improve coordination : A- PNF techniques Slow-reversal and Slow-reversal hold technique. Compined pattern of PNF (bilateral symmetrical, bilateral asymmetrical, reciprocal same diagonal and reciprocal opposite diagonal). B. Frenkel's ex for lower limbs and coordinated exercises for upper limbs TREATMENT: 2-Methods to improve coordination : C. Frenkel's ex: - It is a series of coordinated exercise designed to improve coordination of lower limb with specific graduation to compensate proprioceptive loss by other intact neural sense. Principles - It should be done slowly -The patient must watch movement carefully so put pillow under the head if the patient is supine lying. - When he control one activity then proceed the next one - - Command should be sharp. TREATMENT: Methods to improve coordination : 1. Frenkel's ex: Graduations 1. Fast then slow 2. Big joint then small joint 3. One joint then more than one joint 4. One direction then more than one direction 5. Unilateral then bilateral 6 Symmetrical then asymmetrical 7. Continuous then interrupted 8. on the bed then off the bed 9. Wide BOS then narrow BOS (Supine then sitting then standing) COORDINATION TRAINING INCLUDE: Perception: to tell whether or not performance is occuring as desired through proprioceptive pathways and reinforced by visual and tactile perception. Precision: breaking down activity to units which are simple so that they can be practiced more precisely. Perceptual practice: repetition of activity at frequentaly intervals. Millions of time. Peak performance: the patient practices the movement below the peak performance which is determined according to complexity, muscular effort and repetion in order to avoid fatigue Progression: revision of peak performance as improvement occur and transition of exercise s into functional goal. TREATMENT: 3. Methods to decrease The Tremor of limbs Tonic holding Alternative isometric ex. Slow reversal hold with hold at the end and in between It can be reduced by ankle and wrist weights (Velcro cuffs) (1-2LB) for wrist (2-3LB) for ankle or weighted belt 4. Methods to manage athenia: Graduated Resistive exercises to antigravity muscles. Endurance Ex TREATMENT: 5. Methods to improve balance: Balance can improved in antigravity position (sitting, standing) in normal base of support - Postural stability is improved by using antigravity position in the developmental sequence - Tai Chi and yoga - Plyometric ex’s TREATMENT: 6. Methods to manage gait (gait training): Preparation for ambulation 1. This starts from sitting or prone to reach a quadruped position, then advances to kneeling and then applies crawling 2. When standing from sitting, patient slides forward in the chair and bends his trunk to put COG over his feet .The trunk and legs should be extended only after gaining balance on the feet. 3. Standing activities should be started in the parallel bars. 4. Standing balance exercises. 5. Approximation through shoulders and hips. 6. Tremor can be reduced by ankle weight or weighted belt. 7. Rhythmic Stabilization for trunk rotation. 8. Maintain Standing without pulling on bars. 9. Once standing is stable, alternate lifting of feet is practiced. SPECIFIC INTERVENTIONS FOR BALANCE AND GAIT I. Video-game based coordinative training Intensive coordination training using whole-body controlled videogames can be an effective and motivational therapy for children with progressive ataxia. Supervision from a physiotherapist is essential to ensure the correct movements are being performed and for safety. SPECIFIC INTERVENTIONS FOR BALANCE AND GAIT II. Treadmill training Treadmill training can be an effective intervention for people with ataxia due to brain injury. Intensity and duration of training seem to be significant factors. Consistent intensive training over many months combined with over-ground training may be required. This intervention has not been tested in people with progressive ataxias. The training programme consisted of three commercially available Microsoft Xbox Kinect videogames 7- Methods to manage vertigo: - Vestibular habituation exercises - Cawthorne and Cooksey exercises N.B.: Cold application, vibration and strong resistance have adverse effects on the ataxic patients. crutches or canes may be used but require reciprocal movement of arms and legs with appropriate timing and placement.