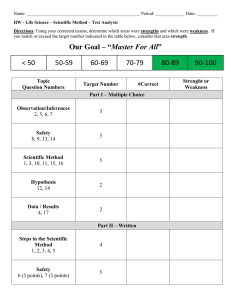
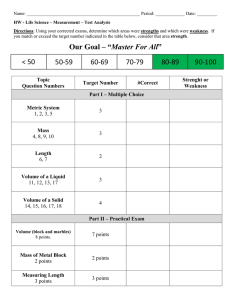
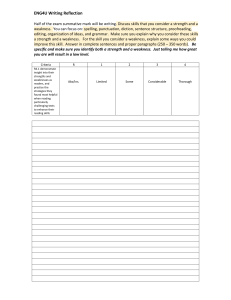
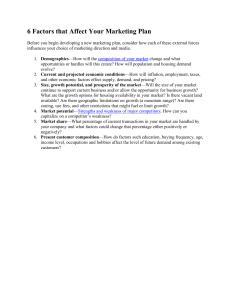
NEUROMUSCULAR EMERGENCIES Elana Pinchefsky Pediatric Neurology, PGY-3 August 14, 2013 OUTLINE ¡ Neuromuscular respiratory failure § Approach ¡ Overview of: § Guillain Barre Syndrome § MG & Myasthenic crisis Neuromuscular Respiratory Failure IMPORTANT INITIAL QUESTIONS TO ANSWER ¡ Is the patient stable? Is respiratory failure imminent? ¡ Should I call ICU? ¡ What is the patients code status? ¡ Also: § Is there a problem with the nervous system? § § § § What What What What is the localization? disorders localize there? investigations do you want to do? is the management? RESPIRATORY FAILURE ¡ Respiratory failure: occurs when the movement of air in and out of the lungs is compromised by weakness of the respiratory muscles ¡ Assuming normal function of the brain and lungs, respiratory failure will not usually occur until respiratory muscle strength has fallen to around ______ % of normal. RESPIRATORY FAILURE ¡ Respiratory failure: occurs when the movement of air in and out of the lungs is compromised by weakness of the respiratory muscles ¡ Assuming normal function of the brain and lungs, respiratory failure will not usually occur until respiratory muscle strength has fallen to around 25–30% of normal FUN FACTS ¡ The accessory muscles can provide adequate ventilation in patients even with diaphragmatic paralysis from bilateral phrenic nerve palsy ¡ ~1/2 the patients with unilateral phrenic nerve palsy are entirely asymptomatic WARNING SIGNS ¡ Rapid, shallow breathing ¡ Stridor ¡ Use of accessory muscles ¡ Single-breath count <20 ¡ Unable to speak in complete sentences ¡ Bulbar weakness § weak cough, nasal voice, accumulation of saliva § Can impair clearing secretion and lead to aspiration ¡ Orthopnea ¡ Staccato speech ¡ Paradoxical abdominal motion (abdo moves in with inspiration) ¡ Significant weakness of neck flexion ¡ Mental clouding or somnolence § 2° hypoxemia and hypercarbia MAJOR CAUSES Site of lesion Specific disorder Motor neuron ALS Poliomyelitis West Nile Virus Spinal Muscular Atrophy Peripheral nerve (+/- nerve roots) Guillain-Barre syndrome/AIDP, Tick paralysis Critical illness polyneuropathy Diphtheric, porphyric, arsenic neuropathy Toxic: shellfish poisoning Neuromuscular junction Botulism Myasthenia gravis Lambert-Eaten myasthenic syndrome Organophosphate poisoning Muscle Polymyositis, dermatomyositis, critical illness myopathy, rhabdomyolysis Acid maltase deficiency, congenital myopathy, congenital muscular dystrophy, Duchenne muscular dystrophy, Limb girdle muscular dystrophy (esp. LGMD 2C02F, 2I), mitochondrial myopathy, myotonic dystrophy (DM1) HISTORY ¡ History of NM disorder? § MG – exacerbation 2° systemic illness, medication § ALS – accelerated phase, decompensation 2° pneumonia ¡ Time course? § GBS - progressive weakness over hours to days § MG - fluctuating weakness (on an hourly basis) present for weeks/months ¡ Distribution of weakness? § MG & GBS - Proximal > distal § GBS – Ascending ¡ Sensory Sx? Autonomic symptoms? § GBS - Distal paresthesias common § MG -No sensory involvement HISTORY ¡ Pain? § Low backache frequently in GBS; neck pain: C-spine lesion? ¡ Any recent illness? § 60% of GBS triggered by viral URT illness or C.jejuni gastro § 40% of myasthenic crises triggered by infection ¡ Pre-existing systemic disorder? § Malignancy, sepsis ¡ Medications ¡ Exposure to fertilizers & pesticides? § Organophosphate poisoning ¡ Any possible exposure to tick bite, snake bite? ¡ Recent diet § Botulism from home-canned goods § Shellfish (saxitoxin, brevetoxin) SYMPTOMS ¡ Subacute (ex. GBS): dyspnoea and orthopnoea § Often assoc w/ bulbar weakness & inability to clear secretions ¡ Gradual onset: inadequate respiration usually occurs first during sleep § Symptoms of nocturnal hypoventilation§ a broken sleep pattern, nightmares, nocturnal confusion, morning headache, daytime fatigue, mental clouding and somnolence ¡ Exertional dyspnea less common in NMDs than in those with other cardioresp d/o ¡ Dyspnoea when lying flat or immersed in water § suggests weakness of the diaphragm PHYSICAL EXAM ¡ Vital signs (stable?, dysautonomia) ¡ Long, thin face (myotonic dystrophy, congenital myopathy) ¡ Skin rash (dermatomyositis) ¡ CNs § Pupils: § Reactivity may be lost in botulism or Miller-Fisher variant of GBS § EOM: § Opthalmoparesis or ptosis (myasthenia, mito d/o, MFS) § Bulbar weakness ¡ Motor exam: § Fasciculations (motor neuron disease) § Paraspinal muscle wasting (acid maltase deficiency) § Power § fatigable weakness § distribution: proximal (myopathy) vs. distal (peripheral neuropathy) PHYSICAL EXAM ¡ Sensory: § Normal in MG § Distal sensory loss in GBS § Sensory level à cord lesion ¡ Coordination: § Ataxia in MFS variant of GBS ¡ Reflexes: § Areflexia in GBS § DTR preserved in MG INVESTIGATIONS ¡ Bedside PFTs: “20/30/40 rule” § Vital capacity, (VC): max exhaled volume after full inspiration § Normal = 60 ml/kg (4 L in 70 kg person). § VC < 20 ml/kg (or 1 L) means intubation § Max inspiratory pressure (MIP) § Index of ability to avoid atelectasis § Normal = > 80 cm H2O (male), >70 cm H2O (female) § MIP >-30 means intubation § Max expiratory pressure (MEP) § Index of ability to cough/clear secretions § Mean MEP = 140 cm H2O (male), 95 cm H20 (female) § MEP <40 means intubation INVESTIGATIONS ¡ ABG: § Hypercarbia = PCO 2 > 45 mmHg •PCO 2 abnormalities are a late feature of NM resp failure • Established respiratory failure from NMDs: ê pO2, compensated respiratory acidosis (~normal pH, é bicarb & pCO2) • Nocturnal hypoventilation: é pH & bicarb with normal pO2 & pCO2 § Hypoxia (PO 2 < 75 mmHg) = usually atelectasis or pneumonia in acute setting ¡ CXR ¡ Basic labs (CBC, SMA-10, LFTs, CK, ESR) PREDICTORS OF NEED FOR MECHANICAL VENTILATION ¡ 20/30/40 rule § Vital capacity <20ml/kg § MIP < 30cm H20 § MEP < 40cm H20 ¡ Serial reduction in VC, MIP, or MEP by >30% ¡ PO 2 <70 mmHg on RA or PCO 2 >50 mmHg w/ acidosis ¡ Bulbar dysfunction- Dysarthria, dysphagia, impaired gag reflex ¡ Bilateral facial weakness ¡ Inability to lift head or elbow of f the bed ¡ Dysautonmia QUESTION? ¡What percentage of patients with GBS require mechanical ventilation? QUESTION? ¡What percentage of patients with GBS require mechanical ventilation? §~25% G B S THE BASICS ¡ Rapidly progressive, often ascending paralysis § Progressive bilateral, relatively symmetric weakness of the limbs with or without involvement of respiratory muscles or cranial-nerve innervated muscles ¡ Areflexia ¡ Albuminocytologic dissociation: Increased CSF protein, normal cell count ¡ NCS- evidence of demyelination ¡ Neurologic emergency àcan rapidly progress to respiratory compromise GBS ¡ Often preceded by: § URTI, GI infection or nonspecific febrile illness in 60% § Respiratory infections = most common § Campylobacter jejuni = most frequently identified organism § Cross reactivity C jejuni epitopes and peripheral nerve gangliosides ¡ Also associated with: § CMV, EBV, mycoplasma, HIV, hepatitis A and B § Surgery, cancer, pregnancy, autoimmune disease, vaccinations EPIDEMIOLOGY ¡ ¡ ¡ ¡ ¡ Incidence increases linearly w/ age Men are 1.5 x more likely to be affected Annual incidence 1-2/100,000 Peds: 0.5-1.5/100,00 <16 years In North America- 5% axonal subtype (higher in China, Japan, Central and South America 30-47%) SUBT YPES GBS subtypes Clinical findings Antibodies EMG/NCS other Acute inflammatory demyelinating polyneuropathy (AIDP) Acute motor axonal neuropathy (AMAN) -Ascending paralysis -Minor sensory symptoms Nonspecific -Demyelination on NCS -Absent F waves -85-90% of cases -flaccid paralysis -often with c. jejuni infection -Acute (<1wk) -profound quadriparesis -ventilation often required -ataxia -areflexia -ophthalmoplegia IgG anti-GM1 IgG anti-GD1a -reduced motor amplitudes -normal sensory -AMAN + AMSAN: 10% IgG anti-GM1 -reduced or absent motor amplitudes - reduced or absent sensory amplitudes -axonal injury by EMG IgG anti GQ1b -ê sensory nerve action potential -motor conduction often Normal - 3-5% - young men Acute motor sensory axonal neuropathy (AMSAN) Miller Fisher Variant SPECTRUM OF GBS SUBT YPES AND SERUM ANTIGANGLIOSIDE ANTIBODIES ACUTE AND CHRONIC VARIANTS Guillain-Barré Syndrome Subtype Acute inflammatory demyelinating polyneuropathy (AIDP) Acute motor and sensory axonal neuropathy (AMSAN) Acute motor axonal neuropathy (AMAN) Miller Fisher syndrome Polyneuritis cranialis Acute sensory neuropathy Description Acute onset of ascending weakness and hyporeflexia with elevated CSF protein and EMG showing demyelinating neuropathy; triphasic course, usually with good recovery Acute onset of ascending weakness and hyporeflexia with elevated CSF protein and EMG showing axonal involvement with reduction of CMAP; triphasic course, usually with poor or limited recovery Clinical syndrome similar to AIDP or AMSAN; elevated CSF protein; electrophysiologic and histopathologic evidence of degeneration strictly limited to sensory axons Acute onset of ophthalmoplegia, hyporeflexia, and ataxia with elevated CSF protein and subsequent recovery Acute onset of multiple cranial nerve palsies (usually bilateral VII and sparing of II) with elevated CSF protein, slowing of motor conduction velocities and recovery Acute onset of sensory loss, areflexia, elevated CSF protein, slowing of motor conduction velocities and recovery ACUTE AND CHRONIC VARIANTS Guillain-Barré Syndrome Subtype Acute pandysautonomia Chronic inflammatory demyelinating polyneuropathy Chronic inflammatory relapsing demyelinating polyneuropathy Chronic inflammatory axonal polyneuropathy Guillain-Barré syndrome with acute onset of weakness and hyporeflexia with encephalopathic features Description Acute onset of multiple dysautonomic symptoms with limited or no motor involvement, CSF protein elevation, and good recovery Subacute or indolent onset of weakness and hyporeflexia with elevated CSF protein and EMG showing demyelinating neuropathy; symptoms persist for >8 weeks and may remain chronic or become progressive Acute or subacute onset of weakness and hyporeflexia with elevated CSF protein and EMG showing demyelinating neuropathy; symptoms persist for >8 weeks and follow a chronic relapsing course Subacute or indolent onset of weakness and hyporeflexia with elevated CSF protein and EMG consistent with an axonal neuropathy; symptoms follow a chronic course; sural nerve biopsy is normal Elevated CSF protein and EMG showing neuropathy. Accompanied by encephalopathic and brainstem symptoms and/or myelitis that may have a protracted course, usually with good recovery CLINICAL PRESENTATION ¡ 1-3 weeks after infection or inciting event § 2/3 of pt had infection in preceding 6 wks ¡ Sensor y: § 70% - initial paresthesias and numbness § children- pain may be prominent presenting sx ¡ a few days later- symmetric weakness: § progresses over days to weeks (by definition max within 4 wks) § max by 2 wks in 50% and by 1 mo in >90% § Ascending: LE before UE; proximal > distal § But may be prox, distal or combination of both CLINICAL PRESENTATION ¡ Reflexes: § Reduced then absent ¡ Pain: § Paresthesia or dysaesthesia, backache or root pain, meningism, muscle pain, joint pain, and visceral pain § Low backache is frequent ¡ Cranial ner ve involvement: § facial weakness in 50% § ophthalmoplegia and lower cranial neuropathies (dysarthria and dysphagia) CLINICAL PRESENTATION ¡ Autonomic involvement: § § § § § § BP fluctuations Cardiac arrhythmias Flushing, sweating Papillary abnormalities AbN hemodynamic responses to drugs AbN GI motility/constipation and bladder dysfunction CLINICAL PRESENTATION ¡ Life threatening respiratory paralysis § Intubation in 25% ¡ Peds: § 16% artificial ventilation § 26% remain able to walk PRESENTATION ¡ Triphasic model: § progressive weakness till nadirà plateau (days, wks or several months) à slower recovery phase § peds: § progressive phase mean 10-12 days § plateau phase 10-12 days (range: days – 4 wks) § prolonged plateau phase if axonal degen ¡ if progresses for longer than 4 wks- consider subacute or chronic inflammatory polyradiculoneuropathy § GBS: max weakness by <4 wks § Subacute : 4-8wks § CIDP: duration of progressive weakness >8 wks EXAMINATION ¡ Symmetric weakness (mild to severe flaccid) § Muscles become wasted after 2 wks in severe cases ¡ Sensation usually normal despite sensory Sx § Mild distal vibration loss ¡ DTR- diminished or absent ¡ Normal sphincter tone ¡ Bedside PFTs (FVC, MIPs/MEPs) INVESTIGATIONS ¡ Lumbar puncture: Albuminocytologic dissociation § CSF protein éa few days after Sx onset § Peaks at 4-6 wks § May not be detectable early in 20% of children § Cell count normal or mild lymphocytic pleocytosis § If é CSF cell count: r/o leptomeningeal malignancy, lyme disease, WNV, HIV related GBS, poliomyelitis INVESTIGATIONS ¡ NCS/EMG: § Reduced motor conduction velocities § Prolonged or loss of F waves § Conduction block in motor nerves and temporal dispersion § Reduced motor amplitudes, fibrillations, positive sharp waves: 2° axonal injury (worse prognosis for complete recovery) ¡ Imaging studies of spinal cord if need to r/o myelopathic disease (transverse myelitis) § Ex. back pain and weakness in LE only NEUROPHYISIOLOGICAL CRITERIA DIFFERENTIAL DIAGNOSIS OF GBS ¡ I n t r a c r a n i a l / s p i n a l c o r d a b n o r m a l i t i e s § Brainstem encephalitis § brainstem ischemia § meningitis carcinomatosis/ lymphomatosis, transverse myelitis, § Acute Myelopathy § Acute transverse myelitis § Space-occupying lesion ¡ A n t e r i o r h o r n c e l l a b n o r m a l i t i e s § Poliomyelitis § West Nile virus or other neurotropic viruses ¡ S p i n a l n e r v e r o o t a b n o r m a l i t i e s § Compression, inflammation (eg, cytomegalovirus), leptomeningeal malignancy ¡ P e r i p h e r a l n e r v e a b n o r m a l i t i e s § Guillain-Barre syndromes § periodic paralysis § CIDP § Diphtheric neuropathy § Post-rabies vaccine neuropathy § drug-induced neuropathy, § § § § § § § § § acute intermittent porphyria critical illness neuropathy vasculitic neuropathy lymphomatous neuropathy heavy metal, biological toxins or or drug intoxication (ex. organophosphates, arsenic), vitamin B1 deficiency (beri-beri), tick paralysis, metabolic disturbances (hypokalaemia, hypophosphataemia, hypermagnesaemia, hypoglycaemia) Mononeuropathy multiplex DIFFERENTIAL DIAGNOSIS OF GBS ¡ Neuromuscular junction abnormalities § Myasthenia gravis, § botulism, § organophosphate poisoning ¡ M u s c u l a r a b n o r m a l i t i e s § Critical illness polyneuromyopathy, § Inflammator y myopathy: polymyositis, dermatomyositis § acute rhabdomyolysis § hypokalaemia § hypophosphatemia § trichinosis …Long…. MANAGEMENT ¡ IVIG (0.4g/kg/day) x 5 days or plasmapharesis (5-6 exchanges over 1-2 wks) § Appear equally effective when given in the first 2 wks after onset § 2012 AAN practice parameters § PE is recommended for nonambulant adult patients with GBS who seek treatment within 4 weeks and should be considered for ambulant patients within 2 weeks of the onset of symptoms § IVIg for nonambulant adult patients with GBS within 2 or possible 4 weeks of the onset § Corticosteroids are not recommended § Sequential treatment with PE followed by IVIg is not recommended § PE and IVIg are treatment options for children with severe GBS § Reduce the duration of the disease and improve the neurological outcome MANAGEMENT ¡ IVIg Equivalent efficacy when compared to PE in first 2 wks Multiple complications were sign. less frequent with IVIg than PE No evidence comparing IVIg and PE for axonal forms Use up to 4 wks (level B recommendation derived from class II evidence of PE started within the first 4 wks and the class I evidence of comparing IVIg and PE in the first 2 wks) § mechanism: ?binding anti-idiotypic Ab, absorbing complement, or downregulating B-call mediated Ab production § § § § MANAGEMENT ¡ PLEX § Beneficial when applied within the first 4 wks of onset, but the largest effect seen when started early (within 2 wks) § 6 trial, but not all studies provided all the outcome measures of interest § costs of PLEX re more than recovered by saving made in avoiding intensive care and hospital stay § mechanism: remove circulating antibody directed towards peripheral nerve Ag MANAGEMENT ¡ Minimize complications of intubation specific to NMDs: § Dysautonomia: can cause severe bradycardia, BP shifts, profound hypotension w/ sedatives § Denervated muscle: can cause fatal hyperkalemia with use of succinylcholine § Avoid depolarizing NM blockers MANAGEMENT ¡ RCTs for oral and IV steroids have failed to show benefit in GBS § 6 trials with 587 pts: corticosteroids are ineffective § 4 trials of oral corticostoids § significantly less improvement after 4 wks with corticosteroids than without § possible explanation: adversely affect the recovery by inhibiting macrophage clearance of myelin debris and so hamper remyelination or aggravate the damage of denervated muscle fibers MANAGEMENT ¡ In children: § No definitive, prospective data to indicate that tx of children with GBS using PLEX or IVIg is effective. § Several limited studies that indicate that both treatments may be effective TREATMENT OF PATIENTS THAT CONTINUE TO DETERIORATE ¡ May have severe or prolonged immune attack that causes severe axonal degeneration § Uncontrolled study: a repeat course of IVIg could be effective § Combination or PE followed by IVIg is no better than IVIg alone § PE after IVIg is also not advised (wash out IVIg) – Lancet review § ? Trial of PE after IVIg since may be a non-responder to IVIG ¡ Treatment of pt who deteriorate after initial improvement: (happens in 8-16%) § Give a second course of IVIg § Prolonged immune response that causes persistent nerve damage that needs treatment for a longer period of time MANAGEMENT ¡ General care: § Serial PFTs (MIP/MEP/FVC) bid to qid § Electrolytes: low potassium, high magnesium & low phosphate à exacerbate muscle weakness § Chest physio, suctioning & incentive spirometry § DVT prophylaxis: sc heparin, compression stockings § HOB elevation § NPO if bulbar weakness; NG or Dobhoff feeding § If severe disease- monitor for possible cardiac arrhythmias ¡ Treat PAIN § § § § Gabapentin Voltaren (diclofenac) Tramacet Other : corticosteroids, opioids, carbamazepine MANAGEMENT ¡ Treat autonomic dysfunction (in 2/3 of pt) § Constipation § Vasoactive and morphine derivatives should be used with caution ¡ Fatigue § § § § Severe fatigue in 60%-80% Independent from severity of weakness ?Due to permanent loss of axons may respond to exercise program § 12 wks of bicycle training was to be effective in 16 severely fatigued, but neurologically recovered GBS pt Diagnosis(of(typical(GBS(! Features(required(for(diagnosis(! Progressive!weakness!in!both!arms!and!legs!(might!start!with!weakness!only!in!the!legs)! Areflexia!(or!decreased!tendon!reflexes)!! ! Features(that(strongly(support(diagnosis(! Progression!of!symptoms!over!days!to!4!weeks! Relative!symmetry!of!symptoms! Mild!sensory!symptoms!or!signs! Cranial!nerve!involvement,!especially!bilateral!weakness!of!facial!muscles!! Autonomic!dysfunction! Pain!(often!present)! High!concentration!of!protein!in!CSF!! Typical!electrodiagnostic!features!! ! Features(that(should(raise(doubt(about(the(diagnosis(! Severe!pulmonary!dysfunction!with!limited!limb!weakness!at!onset! Severe!sensory!signs!with!limited!weakness!at!onset! Bladder!or!bowel!dysfunction!at!onset!! Fever!at!onset! Sharp!sensory!level! Slow!progression!with!limited!weakness!without!respiratory!involvement!(consider!subacute! inflammatory!demyelinating!polyneuropathy!or!CIDP)! Marked!persistent!asymmetry!of!weakness! Persistent!bladder!or!bowel!dysfunction! Increased!number!of!mononuclear!cells!in!CSF!(>50×106/L)!! PROGNOSIS ¡ 5% die (3-10%) – some of these is likely secondary to (sudden) autonomic failure § children ~ 0% in industrialized countries § vs. countries w/ limited resources = 10% ¡ Residual motor weakness in 25% after 1 year ¡ 20% of pt remain unable to walk independently at 6 months ¡ prognosis worse in elderly. In children recovery is more rapid and more likely to be complete § not unanimous- some argue that the clinical course and prognosis are similar PROGNOSIS ¡ Poor prognostic factors (<20% probability of walking independently at 6 months) Older age (>60) Ventilatory support Rapid progression (<7 days) Low motor amplitudes (sugg axonal injury) or absent motor on early NCS responses § Peroneal nerve conduction block § § § § PROGNOSIS ¡ Predictors of need for MV § § § § § § § § § Time from onset to admission < 7 days Inability to cough, bulbar palsy Inability to stand Inability to lift elbows or head LFT increases Presence of autonomic dysfxn Reduction in vital capacity of more than 20% Signs of demyelination Peds: § Onset of sx within 8 days of preceding infection § Presence of CN involvement § CSF protein >800mg/L during the first wk of illness M G BASICS ¡ Fluctuating, fatigable weakness of commonly used muscles ¡ Often involves ocular, bulbar, and respirator y muscles ¡ Can be associated with thymoma or thymic hyperplasia § Thymic lymphofollicular hyperplasia in 70% § Thymoma in 10% ¡ Most patients have circulating antibodies to the Acetylcholine receptor causing defective transmission across the NMJ ¡ Diagnosis of MG is primarily based on the clinical histor y and examination findings demonstrating the distinctive pattern of weakness MG ¡ Antibody -mediated autoimmune disease ¡ Most common NMJ disorder ¡ Prevalence: 1/10,000-20,000 § prevalence rates have increased over time with recent estimates approaching 20 per 100,000 in the US population ¡ ¡ ¡ ¡ Women: 2 n d & 3 r d decade Men: 5 t h & 6 t h decade Associated autoimmune diseases: 5% Comorbid thyroid disease: 10% CLINICAL PRESENTATION ¡ The clinical hallmark of MG is the presence of fluctuating fatigable muscle weakness that is brought on by activity and improves with rest § Differentiate from general fatigue or exhaustion ¡ Initial symptoms involve the ocular muscles in up to 85% of pt § ptosis, intermittent diplopia, or both § Ptosis worsens after exercise, reading, while driving, and with exposure to direct sunlight ¡ Prominent bulbar symptoms in 20% early in MG course § dysarthria, dysphagia, and difficulty chewing § higher in anti-MuSK CLINICAL PRESENTATION ¡ ¡ ¡ ¡ Weakness of palatal muscles à nasal quality to the voice Speech - may become slurred with prolonged talking Facial weakness – sleepy or sad appearance Swallowing concerns - may be limited to mild difficulty with solid foods, eg, ‘‘feels like the food gets stuck’’ § Progressively weaker chewing force with each successive bite § Worse with solids ¡ Diaphragmatic weakness à orthopnea ¡ Symptoms of MG may worsen with: § exposure to extreme heat, emotional stress, infection, systemic illness, pregnancy, the menstrual cycle, or drugs that affect neuromuscular transmission. PHYSICAL EXAM ¡ Ptosis § may improve in response to local cooling of the lid § Curtain sign (enhanced ptosis or paradoxical ptosis) § Lid twitch sign ¡ Ophthalmoparesis § The medial rectus muscle is most frequently affected § Examination of EOM should include a min of 15-30 sec of lateral and superior gaze holding ¡ Bulbar weakness ¡ Fatigable extremity weakness ¡ Normal pupils ¡ Normal sensory exam and DTR PHYSICAL EXAM ¡ Respiratory muscle weakness § tachypnea and shallow breathing § weak sniff and cough § tachypnea or tachycardia ¡ Patients with MG with respiratory muscle weakness will often have coexisting weakness of neck flexion/ extension PHYSICAL EXAM- FATIGUING MANEUVERS INVESTIGATIONS ¡ Antibodies ¡ Tensilon – no longer available ¡ Ice Pack test – apply ice pack to ptotic lid ¡ EMG/ NCS: § Repetitive stimulation § Single fiber EMG (SFEMG) ¡ CT chest § r/o thymoma ANTIBODIES ¡ Anti - AchR Ab § 90% of generalized patients § 50% of ocular MG § 50% of childhood MG ¡ MuSK - muscle-specific receptor tyrosine kinase (MuSK) § 40% of pt with no AchR Ab § Typically prominent bulbar weakness DIAGNOSTIC TESTS MANAGEMENT ¡ Symptomatic therapy § Mestinon (cholinesterase inhibitor) ¡ Immune Modulators § Short term § IVIG § PLEX § Long term § § § § Prednisone Azathioprine Mycophenylate mofetil Cyclosporine ¡ Thymectomy is mandatory for thymoma and should be considered for non-thymomatous patients • Symptomatic therapy • Mestinon (cholinesterase inhibitor) • Initial oral dose: 30 mg to 60 mg every 4 to 6 hours • Max 120 mg every 4 hours • Muscarinic side effects: cramps, diarrhea, sweating, bronchial and nasal secretions, bradycardia, nausea, and vomiting • *higher doses may overexpose remaining functional AChRs to Ach, potentially desensitizing them and exacerbating weakness * MANAGEMENT ¡ Short-term immune-directed therapies: § (1) inducing rapid improvement in patients with severe disease or crisis § (2) reducing perioperative morbidity prior to surgery often thymectomy § (3) chronic therapy in selected refractory patients. § PLEX or IVIG MANAGEMENT ¡ Long-term immune-directed therapies: § Corticosteroids § Prednisone is the first choice for immunosuppressive therapy of MG, and its use is indicated when generalized or ocular symptoms are not adequately controlled by cholinesterase inhibitors § clinical response ~ rapid: within 2 to 4 weeks § dose ~1 mg/kg/d to 1.5 mg/kg/d § *Transient worsening of weakness has been reported to occur in ~1/3 - 1/2 § intubation req in 8.6% § PE or IVIG prior to or during steroid initiation - lessening the risk of steroidinduced exacerbation. § Non steroidal immune mediated Tx/Steroid sparing agents § Azathioprine § Mycophenylate mofetil § Cyclosporine - severe generalized disease refractory to all conventional tx MYASTHENIC CRISIS ¡ Defined by: weakness from MG that is severe enough to necessitate intubation for ventilatory support or airway protection. ¡ ~1/5 patients with MG will suffer myasthenic crisis at some point during their illness INDICATION FOR INTUBATION ¡ ¡ ¡ ¡ ¡ ¡ increasing tachypnea declining tidal volumes, hypoxemia, hypercapnia difficulty with secretions forced vital capacity < 1L negative inspiratory force of< 20 cm H2O MYASTHENIC CRISIS ¡ Common precipitants: § § § § § § Broncho-pulmonary infections, aspiration, surgical procedures including thymectomy, corticosteroid-induced worsening, rapid tapering of immune modulators exposure to drugs that may increase myasthenic weakness MYASTHENIC CRISIS - MANAGEMENT ¡ Cholinesterase inhibitors à hold when intubated § can potentially increase weakness due to depolarization blockade. § signs of cholinergic hyperactivity (excessive salivation, increased bronchial secretions, muscle fasciculations, and abdominal cramping) àcomplicate the management of airway secretions ¡ PLEX or IVIG § PLEX § IVIG ¡ Prednisone § Since the effect of PE is short- term § High-dose daily prednisone –add to confer a more prolonged therapeutic effect § *transient worsening of weakness MYASTHENIC CRISIS - MANAGEMENT ¡ PLEX § § § § § 3 – 6 exchanges, every- other-day reduces the levels of circulating antibodies produces improvement in days Need central line Common side effects: paresthesias from citrate-induced hypocalcemia, symptomatic hypotension, complications from line (infections and thrombotic complications), reduce coagulation factors MYASTHENIC CRISIS - MANAGEMENT ¡ IVIG § 2 g/kg, which is divided over 2 to 5 days § Maintenance doses: 0.5 g/kg to 1 g/kg usually on a monthly basis § reports suggest a similar efficacy of IVIG compared with PE, but other reports and personal experience suggest that it is less effective in MG crisis. § RCTs showing comparable efficacy in treatment response compared with PE (Gajdos et al, 2008) and a recent double-blind placebo-controlled trial in MG patients with worsening weakness (Zinman et al, 2007) § onset of improvement: 7 - 10 days & lasts for 4 - 8 weeks § Common side effects: headaches, chills, and fever, (usually improve with slower infusion rate) § Serious side effects (rare): renal toxicity, stroke, and aseptic meningitis, anaphalaxis in IgA deficiency MYASTHENIC CRISIS ¡ Noninvasive mechanical ventilation –BiPAP § may circumvent the need for intubation in selected MG patients who have not developed hypercapnia (PCO2 greater than 50 mm Hg) § reduces pulmonary complications and lengths ICU and hospital stay § Most effective – prominent oropharyngeal weakness and less severe diaphragmatic impairment TAKE HOME POINTS ¡ Is respirator y failure imminent? § § § § Identify early and avoid emergency intubation Do bedside PFTs 20/30/40 rule Monitor for warning signs ¡ Is there a problem with the ner vous system? § § § § What What What What is the localization? disorders localize there? investigations do you want to do? is the management? ¡ GBS: Progressive bilateral, ascending, relatively symmetric weakness of the limbs + areflexia ¡ MG: Fluctuating, fatigable weakness of commonly used muscles THANK YOU! B O T U L I S M