THE CARDIOVASCULAR SYSTEM
By
Dr. Rabei Al Dubooni
Assist. Prof
Objectives: The following lectures aim to teach the student about:
Normal values of pulse rate in pediatrics
Congenital heart diseases
Cyanotic: TOF, TGA, TA, EA, TAPVR, Approach to neonatal cyanosis
Acyanotic: ASD,VSD, PDA.
Obstructive: Coarctation of Aorta.
Heart failure in infancy and childhood: Etiology, presentation, diagnosis,& treatment.
Rheumatic fever: Etiology, Diagnosis, Treatment, Prevention.
Infective endocarditis : Etiology, Diagnosis, Treatment, Prevention.
Cardiomyopathies : types with special focus on dilated CMP.
Supraventricular tachycardia.
HISTORY
CHILDREN DO NOT PRESENT WITH THE TYPICAL FEATURES OF CONGESTIVE HEART FAILURE
AS SEEN IN ADULTS.
Age is very important when assessing child.
Infants:
Feeding difficulties
Easily fatigued
Sweating while feeding
Rapid respirations
Older children:
Shortness of breath
Dyspnea on exertion
PHYSICAL EXAMINATION:
Cardinal features of heart failure in children:
•
•
•
•
Tachycardia
Rapid respiration
Tender hepatomegaly
Pulmonary rales
REMEMBER THAT DURING PHYSICAL EXAMINATION:
− Need to refer to normal heart and respiratory rates for ages to determine
tachycardia and tachypnea.
− Height and weight should be assessed to determine proper growth.
− Always get upper and lower extremity blood pressures and pulses.
− Hepatomegaly suggests heart failure. Splenomegaly in infective
endocarditis
− Always palpate for femoral pulses and compare with radials.
− Examine for cyanosis and clubbing.
DIAGNOSTIC TESTS
Chest radiograph for:
HEART SIZE
LUNG FIELDS
RIBS FOR NOTCHING
POSITION OF GREAT VESSELS
ELECTROCARDIOGRAM
ECHOCARDIOGRAPHY
OTHERS :
TESTING
MRI, CARDIAC CATHETERIZATION, ANGIOGRAPHY,
EXERCISE
Congenital Heart Diseases
Classification of congenital heart diseases
Group I :
Group II:
Group III:
Left to right shunts (acyanotic): ASD, VSD, PDA
Right to lefts shunts (cyanotic): TOF, TGA,TA, EA
Obstructive lesions: AS, PS, COA
INCIDENCE :
8/1000 BIRTHS
ETIOLOGY:
Multifactorial inheritance ( genetic predisposition +
environmental factors).
Common environmental factors include:
Maternal illness (eg, diabetes, rubella, systemic lupus
erythematosus).
Maternal intake of teratogenic agents (eg, lithium, retinoic acid,
alcohol, anticonvulsants).
Paternal age may also be a risk factor.
GENETIC FACTORS
Certain numerical chromosomal abnormalities, such as Down
syndrome (trisomy 21), trisomy 18, trisomy 13, and monosomy
X (Turner syndrome), are strongly associated with congenital
heart disease. However, these abnormalities account for only
about 5% of patients with CHD.
Many other cases involve microscopic deletions on
chromosomes or single-gene mutations. Often, the microscopic
deletions and mutations cause congenital syndromes affecting
multiple organs in addition to the heart. Examples include
Digeorge syndrome (microdeletion in 22q11.2) and Williams
syndrome (microdeletion in 7p11.23).
Single-gene defects that cause syndromes associated with
CHD like (Marfan syndrome).
Acyanotic Congenital Heart Disease
Left-to-Right Shunt Lesions
•
•
•
•
Atrial Septal Defect (ASD)
Ventricular Septal Defect (VSD)
Atrioventricular Septal Defect (AV Canal)
Patent Ductus Arteriosus (PDA)
Atrial Septal Defect
• ASD is an opening in the atrial septum permitting free
communication of blood between the atria. Seen in 10% of all
CHD.
There are 3 major types:
• Secundum ASD – at the Fossa Ovalis, most common.
• Primum ASD – is lower in position.
• Sinus Venosus ASD – high in the atrial septum,
associated with anomalous venous return & the least
common.
CLINICAL PRESENTATION
• Most are asymptomatic but may have easy fatigability or mild growth
failure.
• Cyanosis does not occur unless pulmonary hypertension is present.
Examination:
• Hyperactive precordium, RV heave, fixed widely split S2.
• II-III/VI systolic ejection murmur at Left SB(2nd intercostal).
• A mid-diastolic murmur heard over LLSB indicates a large defect.
DIAGNOSIS
• Chest x-ray—varying heart enlargement (right ventricular and
right atrial); Increased pulmonary vessel markings.
•
•
ECG—right-axis deviation and RVH. In the right precordial
leads, an rsR ′ pattern is usually present.
Echocardiogram gives definitive diagnosis.
Treatment:
• Surgical or Catheterization closure is generally
recommended for secundum ASD with a Qp:Qs ratio
>2:1.
• Closure is performed electively between ages 1-3 yrs to
avoid late complications.
• Surgical correction is done earlier in children with CHF
or significant pulmonary hypertension.
COURSE & PROGNOSIS
Patients usually tolerate an ASD well in the first two decades of life,
and the defect often goes unnoticed until middle or late adulthood.
Pulmonary hypertension and reversal of the shunt (Eisnmenger
syndrome) are rare late complications.
Infective endocarditis is uncommon.
Spontaneous closure can occur, most frequently in children with a
defect less than 4 mm in diameter.
Mortality of surgical closure is < 1%.
Ventricular Septal Defect
VSD – is an abnormal opening in the ventricular septum, which
allows free communication between the Rt & Lt ventricles.
Accounts for 25% of CHD
Clinical Signs & Symptoms
• Small - moderate VSD, 3-6mm, are usually asymptomatic and
50% will close spontaneously by age 2yrs.
• Moderate – large VSD, almost always have
symptoms(dyspnea, feeding difficulties, poor growth, sweating,
pulmonary infection, heart failure) and will require surgical
repair
EXAMINATION
Small - moderate VSD
No lifts, heaves, or thrills are present.
The first sound at the apex is usually covered by the murmur, and
the second sound at the pulmonary area is physiologically split.
A grade II–IV/VI medium to high-pitched, harsh pansystolic murmur
is heard best at the left sternal border in the third and fourth
intercostal spaces. The murmur radiates over the entire precordium.
Large Ventricular Septal Defects With Pulmonary Hypertension
The precordium is prominent, the sternum bulges.
Both LV and RV heaves are palpable.
S2 is palpable in the pulmonary area.
A thrill may be present at the lower left sternal border.
S2 is usually single or narrowly split, with accentuation of the
pulmonary component. The murmur ranges from grade I to IV/VI
and is usually harsh and pansystolic.
A diastolic flow murmur may be heard, depending on the size of the
shunt.
IMAGING STUDIES
CX-ray findings depend on the size of the VSD.
Small VSD: usually have normal studies.
Larger VSD: cardiomegaly, increased pulmonary blood flow, main
pulmonary artery segment may be dilated.
ECG :
normal in small left-to-right shunts.
Left ventricular hypertrophy (LVH) usually occurs in patients with large
left-to-right shunts. Combined ventricular enlargement occurs in
patients with pulmonary hypertension caused by increased flow,
increased resistance, or both.
ECHOCARDIOGRAPHY
Two-dimensional echocardiography can reveal the size of a VSD and
identify its anatomic location.
CARDIAC CATHETERIZATION AND ANGIOCARDIOGRAPHY
Catheterization is indicated in those patients with increased pulmonary vascular
resistance.
Treatment
• Small VSD - no surgical intervention, no physical restrictions, just
reassurance and periodic follow-up and endocarditis prophylaxis.
• Symptomatic VSD - Medical treatment initially with afterload reducers
& diuretics.
• Prophylaxis against infective endocarditis(after dental or GU procedures).
Indications for Surgical Closure:
Patients with cardiomegaly, poor growth, poor exercise tolerance,
or other clinical abnormalities who have a significant shunt (> 2:1)
typically undergo surgical repair at age 3–6 months. Also those
with intractable heart failure not controlled by medical treatment.
COMPLICATIONS
Large defects lead to heart failure, failure to thrive
Endocarditis
Pulmonary hypertension
Patent Ductus Arteriosus
Persistence of the normal fetal vessel that joins the PA to the Aorta.
• Normally closes in the 1st wk of life.
• Accounts for 10% of all CHD, may be seen in association with other
congenital heart lesions and can often play a critical role in some
lesions.
• Female : Male ratio of 2:1
• Can be caused by congenital Rubella.
• The frequency of PDA in preterm infants weighing less than 1500 g
ranges from 20% to 60%.
Clinical Signs & Symptoms
•
•
•
•
•
•
Small PDA’s are usually asymptomatic.
Large PDA’s can result in symptoms of CHF, growth restriction, FTT.
Collapsing arterial pulses.
Widened pulse pressure .
Enlarged heart, prominent apical impulse.
The murmur is characteristic. It is a rough machinery murmur maximal
at the second left intercostal space.
• Mid-diastolic flow murmur may be heard at the apex.
IMAGING STUDIES
ECG AND
CHEST X-RAY findings are normal with small PDAS
moderate
to large shunts may result in a full pulmonary artery
silhouette and increased pulmonary vascularity.
ECG
findings vary from normal to evidence of LVH. If pulmonary
HTN is present, there is also RVH.
Echocardiography
Cardiac Catheterization and Angiocardiography
Treatment:
• Indomethacin, inhibitor of prostaglandin synthesis can be used
in premature infants. It has no effect on duct closure in full term
neonate and in children.
• PDA requires surgical or catheter closure.
• Closure is required for heart failure & to prevent pulmonary
vascular disease.
• Usually done by ligation & division or intra vascular coil.
• Prophylaxis against infective endocarditis(after dental or GU
procedures).
Obstructive Heart Lesions
• Pulmonary Stenosis
• Aortic Stenosis
• Coarctation of the Aorta
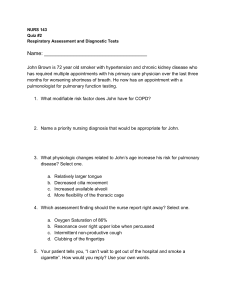
Coarctation of the Aorta
. Coarctation of the aorta is a narrowing in the aortic arch that usually occurs
in the proximal descending aorta near the takeoff of the left subclavian
artery near the ductus arteriosus (juxtaductal). It is commonly associated
with bicuspid valve. Abdominal aorta is rarely involved.
More common in Turner’s syndrome.
• Male: Female ratio 3:1.
• Accounts for 7 % of all CHD
• The obstruction to blood flow will lead to LVH.
Clinical Signs & Symptoms
• Classic signs of coarctation are diminution or absence of femoral pulses.
There is delay in femoral pulse compared with radial pulse.
• Blood pressure (> 15 mm Hg) discrepancy between the arms and legs.
• 90% have systolic hypertension of the upper extremities.
• With severe coarctation, heart failure and shock may occur.
• The systolic murmur of coarctation is heard in the left axilla and the left
back.
• Cardiomegaly, rib notching on X-ray.
• ECG in older children may be normal or may show LVH.
• Echocardiography
Notching of the ribs caused by marked enlargement
of the intercostal collaterals .
Treatment
• With severe coarctation maintaining the ductus with prostaglandin E is
essential.
• Surgical intervention, to prevent LV dysfunction.
• Angioplasty is used in some centers.
• Re-coarctation can occur, balloon angioplasty is the procedure of choice.
• Prophylaxis against infective endocarditis(after dental or GU
procedures).
Cyanotic congenital heart disease
Tetralogy of Fallot
It is the most common cyanotic congenital heart disease
Components:
Pulmonary stenosis and infundibular stenosis (obstruction to
right ventricular outflow)
VSD
Overriding
Right
aorta (overrides the VSD)
ventricular hypertrophy
Hemodynamics
Pulmonary stenosis plus hypertrophy of subpulmonic muscle (crista
supraventricularis) → Varying degrees of right ventricular outflow
obstruction → Blood shunted right-to-left across the VSD with varying
degrees of arterial desaturation and cyanosis.
Clinical Picture
• Cyanosis may present at any time but usually not in the first few
weeks ( in contrast to TGA )
• Paroxysmal attacks of Anoxic Spells (=Tet spells = hypercyanotic spells)
Most commonly start at age 4–6 months
– Predominantly after waking up.
– Child is irritable and cries.
– Dyspnea& deepening of cyanosis. Decrease or disappearance of the
systolic murmur.
– Altered consciousness.
– There may be convulsions due to brain anoxia.
– Frequency varies from once a few days to many attack everyday.
Examination
Generally: growth failure.
Varying degrees of cyanosis .
Clubbing of fingers & toes.
Right ventricular impulse at the left sternal border.
Single S2
Murmur: usually ejection systolic heard best over the pulmonary area.
Squatting increase systemic vascular resistance . This decreases
the amount of right-to-left shunt, forcing blood through the
pulmonary circuit, and would help ward off cyanotic spells.
Squatting may be seen in older children during exersises.
Investigations
CXR : Boot-shaped normal
size heart
ECG : RAD & RVH
Echocardiography
Cardiac Catheterization
CBC: secondary polycythemia
Complications:
1)
2)
3)
4)
5)
6)
7)
Each anoxic spell is potentially fatal
Polycythemia may lead to Cerebrovascular thrombosis
Anoxic infarction of CNS
Brain Abcess
Infective endocarditis
Fatal arrhythmias
Growth failure
Management of anoxic spell:
Knee chest position
Humified O2
Be careful not to provoke the child
Morphine 0.1 -0.2 mg/kg subcutaneously or iv.
Correct acidosis : sodium bicarbonate iv 1 mmol/kg slowly
Propranolol start (0.1mg/kg/iv) slowly during spells followed by (0.5 to 1.0)
mg/kg/6hourly orally (prophylaxis).
Vasopressors: Methoxamine or Phenylephrine im or iv drip
The onset of Tet spells usually prompts surgical intervention
SURGICAL REPAIR FOR TOF
Palliative procedure: BLALOCK
TAUSSIG shunt
Subclavian a. to Pulmonary a. anastomosis
Definitive operation: complete surgical repair with VSD closure
and removal of the pulmonary stenosis can be performed in infancy.
TRANSPOSITION OF GREAT ARERIES (TGA)
Aorta originating from the right ventricle, and pulmonary artery originating
from the left ventricle.
Accounts for 5-7% of all congenital heart disease.
Survival is dependent on the presence of mixing between the pulmonary
and systemic circulation( associated ASD, VSD, or PDA).
50% of patients have a VSD
Usually presents in the first day of life with profound cyanosis without
respiratory distress.
More common in boys
Examination :
Cyanosis in an otherwise healthy looking baby
Loud S2
Loud VSD murmur if it is present
CXR : Egg on side & narrow mediastinum
ECG : frequently looks normal
Echocardiography
Cardiac Catheterization and Angiocardiography
Acute (Emergency) management in newborn baby
Initial medical management includes prostaglandin E1 to maintain ductal
patency. If significant hypoxia persists on prostaglandin therapy, a balloon
atrial septostomy improves mixing between the two circulations.
Surgical repair Aterial switch (old style).
Arterial switch (ASO) : performed at age 4–7 days
TRICUSPID ATRESIA:
The absence of the tricuspid valve results in a hypoplastic right
ventricle. All systemic venous return must cross the atrial septum
into the left atrium.
A PDA or VSD is necessary for pulmonary blood flow and
survival.
Clinical Manifestations
Usually severely cyanosed since birth.
Single S2.
If a VSD is present, there may be a murmur.
ECG: LVH & LAD with right atrial enlargement .
Echocardiography &Cardiac Catheterization : for definite diagnosis
Treatment:PGE-1, and minimal O2 to maintain ductal patency
Palliative procedure: Blalock-Taussig procedure
Definitive: bidirectional cavopulmonary shunt (bidirectional Glenn) and
Fontan procedure.
EBSTEIN ANOMALY
Downward displacement of abnormal tricuspid valve into right ventricle; the right
ventricle gets divided into two parts: an atrialized portion, (which is thin-walled), and a
smaller normal ventricular myocardium (the really functioning RV).
• Right atrium is huge; tricuspid valve regurgitant
• Right ventricular output is decreased because:
− Poorly functioning, small right ventricle
− Tricuspid regurgitation
− Variable right ventricular outflow obstruction—abnormal anterior tricuspid valve
leaflet. Therefore, increased right atrial volume shunts blood through foramen Ovale or
ASD → cyanosis.
Clinical presentation
− Severity and presentation depend upon degree of displacement of valve
and degree of right ventricular outflow obstruction
° May not present until adolescence or adulthood
° If severe in newborn → marked cyanosis, huge heart
− Pansystolic murmur of tricuspid insufficiency over most of anterior left
chest (most characteristic finding)
Chest x-ray: heart size varies from normal to massive .
pulmonary oligemia in severe cases.
ECG:
tall and broad P waves, RBBB, WPW (delta wave) may be
associated.
Echocardiography
•
Treatment:
− PGE1
− Systemic-to-pulmonary shunt
− Then staged surgery
Total Anomalous Pulmonary Venous Return:
Total anomalous pulmonary venous return (TAPVR) occurs when all
the pulmonary veins connect to the systemic veins or right atrium
instead of draining into the left atrium.
The anomalous drainage may be at the supracardiac (e.g.
innominate vein or superior vena cava), cardiac (right atrium directly
or coronary sinus) or infracardiac (e.g. portal vein, inferior vena
cava) level or may be of a mixed type with more than one
anomalous site.
Presentation
Congestive heart failure and varying degrees of cyanosis.
A prominent left parasternal heave (RV volume overload).
The second heart sound may be widely split and fixed with
respiration(due to associated ASD)
There is a flow murmur across the pulmonary and mitral valve.
ECG shows right ventricular hypertrophy .
CXR will show increased pulmonary vascular markings. The
‗snowman‘ sign (enlarged superior mediastinum) is seen in
supracardiac TAPVR to the left innominate vein in older infants.
Echocardiogram defines the anatomy sufficiently.
Treatment: Cardiac surgery
APPROACH TO NEONATAL CYANOSIS
Central cyanosis is a bluish discoloration of the skin,
mucus membranes and tongue that is observed when
deoxygenated hemoglobin is > 3g/dl in arterial blood
or > 5g/dl) in capillary blood.
Another type of cyanosis, called peripheral cyanosis, involves a
bluish discoloration of the skin but sparing of the mucus membranes
& tongue. In this type, a normal PaO2 value is detected. Vasomotor
instability, and vasoconstriction caused by cold, low cardiac output
and polycythemia can all slow movement through the capillaries and
lead to peripheral cyanosis.
Peripheral cyanosis is often a normal finding in newborns, especially
when only the extremities are affected (acrocyanosis) due to
vasoconstriction as a result of transient hypothermia; however, it is
important to rule out serious causes of peripheral cyanosis, such as
sepsis
Pregnancy & labor HX
GDM
Oligohydramnios
Hypertension
Maternal age
Lithium(1st trimister)
PROM, fever, GBS +ve
Sedatives/anesthetics
C-section
Preterm infant
Meconium
Associated causes
TTN, RDS, CHD, Low BS
Pulmonary hypoplasis.
IUGR, polycythemia, hypoglycemia
Down’s S.
Epstein anomaly
Sepsis
Apnea
TTN, RDS, PPHN
RDS, Apnea
MAS
Differential Diagnosis :
1.CNS (associated with other CNS manifestation)
2.Respiratory(associated with dyspnea and respiratory findings)
3.Right to Left shunt(little or no dyspnea , possibility of murmurs)
4.Methemoglobinemia
Hyperoxia test:
Administer 100 % oxygen for > 10 min
If PaO2 exceeds 100 mmHg: pulmonary disease likely.
If PaO2 remains below 70 mmHg or rises by < 30 mmHg or
SaO2 unchanged: cardiac cause (R-L shunt) likely
CONGESTIVE HEART FAILURE
Refers to a clinical state of systemic and pulmonary congestion
resulting from inability of the heart to pump as much blood as
required for the adequate metabolism of the body.
ETIOLOGY:
CARDIAC
congenital structural malformations
● excessive preload
● excessive afterload
non - congenital structural anomalies
● cardiomyopathy
● myocarditis
● myocardial infarction
● acquired valve disorders
● hypertension
● kawasaki syndrome
● arrhythmia (bradycardia or tachycardia)
NONCARDIAC
● Anemia
● Sepsis
● Hypoglycemia
● Diabetic ketoacidosis
● Hypothyroidism
● Other endocrinopathies
● Arteriovenous fistula
● Renal failure
HISTORY
CHILDREN DO NOT PRESENT WITH THE TYPICAL FEATURES OF CONGESTIVE HEART
FAILURE AS SEEN IN ADULTS.
AGE IS VERY IMPORTANT WHEN ASSESSING CHILD.
INFANTS:
FEEDING DIFFICULTIES
EASILY FATIGUED
SWEATING WHILE FEEDING
RAPID RESPIRATIONS
OLDER CHILDREN:
SHORTNESS OF BREATH
DYSPNEA ON EXERTION
PHYSICAL EXAMINATION:
•
•
•
•
Tachycardia
Rapid respiration
Tender hepatomegaly
Pulmonary rales
IMAGING STUDIES
The absence of cardiomegaly on a chest x-ray usually rules out the
diagnosis of heart failure.
An Echocardiogram assesses the heart chamber sizes, measures
myocardial function, and diagnoses congenital heart defects when present.
ECG : Can diagnose different arrhythmias
TREATMENT
The goals of medical therapy for congestive heart failure include
the following:
Reducing the preload
Enhancing cardiac contractility
Reducing the afterload
Improving oxygen delivery
Enhancing nutrition
GENERAL MEASURES:
Bed rest and limit activities
Nurse propped up or in sitting position
Expressed breast milk for small infants
Fluid and salt restriction in volume overloaded
Correction of anemia ,acidosis, hypoglycemia and hypocalcaemia
if present
Oxygen
TREATMENT: PHRMACOLOGICAL THERAPY
PRELOAD REDUCTION:
1. Diuretics: (oral) or (IV) diuretics (furosemide, thiazide. metolazone).
2. Venous dilators (eg: nitroglycerin).
CONTRACTILITY SUPPORT:
1. Dopamin, dobutamin
2. Digoxin
AFTERLOAD REDUCTION
1.Oral Angiotensin converting enzyme inhibitors (ACEI) e.g: captopril, enalapril
2. IV hydralazine, nitroprusside, or alprostadil
DOSES:
Furosemide: 1 mg/kg/dose PO or IV
Hydrochlorothiazide: 2 mg/kg/d PO divided bid
IV Dopamine : 5-10 mcg/kg/min IV (usual dosage; maximal dosage may be up to
28 mcg/kg/min)
Dobutamine: 5-10 mcg/kg/min iv
Captopril: 0.1-0.5 mg/kg/d orally divided q8h
Enalapril: 0.1 mg/kg/d orally divided doses, not to exceed 0.5 mg/kg/d
Carvidolol: 0.2-0.4 mg/kg/dose bid.
Spironolactone: 1-3 mg/kg/day.
DIGOXIN: start with rapid digitalization then shift to maintenance:
Rapid digitalization can be achieved by administration of ―total
digitalizing dose (TDD) as follow:
Premature: 20 μg/kg (0.02 mg/kg).
Full-term neonate (up to 1 mo): 20-30 μg/kg
Infant or child: 25-40 μg/kg
Adolescent or adult: 0.5-1 mg in divided doses
NOTE: these doses are PO; IV dose is 75% of PO dose.
½ TDD is given initially followed by 1/4 TDD in 2 doses 12 hrs apart.
Maintenance digoxin : 5-10 μg/kg/day, divided q12h
Managing acute congestive heart failure (acute pulmonary edema) in children:
Admit to the ICU.
Head up position.
Oxygen.
IV furosemide: 1-2 mg/kg.
Dopamine if there is associated hypotension: (5-10 mcg/kg/min) .
Nitrates ( nitroglycerin1–3 mcg/kg/min ) as venodilators if ↑ pulmonary capillary wedge
pressure
???Digoxin (TDD):
RHEUMATIC FEVER:
Due to an immunologic reaction that is a delayed sequele of group A betahemolytic streptococcal infections of the pharynx.
A family history of rheumatic fever and lower socioeconomic status are
additional factors.
The infection often precedes the presentation of rheumatic fever by 2 to 6
weeks. Streptococcal antibody tests, such as the antistreptolysin O (ASOT)
titer, are the most reliable laboratory evidence of prior infection.
Diagnosis:
= {2 Major or (1Major + 2Minor) Jones Criteria} + Evidence of
antecedent Streptococcal infection(recent scarlet fever, positive
throat culture, or elevated ASOT or other antistreptococcal
antibodies).
Major : Migratory polyarthritis, Carditis, Erythema marginatum,
Chorea, Subcutaneous nodules.
Minor : Fever, Arthralgias, Previous rheumatic fever, leukocytosis,
elevated ESR or CRP, and prolonged PR interval.
.
TREATMENT
Bed rest
Benzathine Penicillin 1.2 million unit im.
Salicylate: 50-70 mg/kg/day in 4 divided doses PO for 3-5 days,
followed by 50 mg/kg/day in 4 divided doses PO for 3 wks and half
that dose for another 2-4 wks
Prednisolone: 1-2mg/kg/day for 3 weeks for severe carditis or
congestive HF.
Prevention:
Benzathine Penicillin: 600,000 IU for children weighing ≤27
kg ; 1.2 million IU for children weighing >27 kg every 4 wk.
Duration of prophylaxis for the patient:
without carditis: 5years or until he is 21 years old.
With carditis : 10 years or until age is 40.
Infective Endocarditis ;
Etiology/epidemiology
− Most are Streptococcus viridans (alpha hemolytic) and Staphylococcus
aureus
− Organism associations
° S. viridans—after dental procedures
° Group D streptococci—large bowel or genitourinary manipulation
° Pseudomonas aeruginosa and Serratia marcescens— intravenous drug users
° Fungi—after open heart surgery
° Coagulase-negative Staphylococcus—indwelling intravenous catheters
− Highest risk with prosthetic valve and uncorrected cyanotic heart lesions
• Clinical presentation
− Prolonged intermittent fever, weight loss, fatigue, myalgia, arthralgia, headache,
nausea, vomiting
− New or changing heart murmur
− Splenomegaly, petechiae, embolic stroke, CNS abscess, CNS hemorrhage, mycotic
aneurysm (all more with Staphylococcus)
− Skin findings—rare; late findings (uncommon in treated patients); represent vasculitis
from circulating Ag-Ab complexes; if present, are highly suggestive
° Osler nodes—tender, pea-sized, intradermal nodules on pads of fingers and toes
° Janeway lesions—painless, small erythematous or hemorrhagic lesions on
palms and soles
° Splinter hemorrhage—linear lesions beneath nail beds
º Roth spots —retinal exudates
DIAGNOSIS
Three to 5 separate blood collections should be obtained after careful
preparation of the phlebotomy site.
Complications
− Most common: heart failure from aortic or mitral lesions
− Others: systemic or pulmonary emboli, myocardial
abscess, myocarditis, valve obstruction, heart block,
meningitis, osteomyelitis, arthritis, renal abscess, immune
complex−mediated glomerulonephritis.
TREATMENT
Antibiotic therapy must be started after blood cultures
are obtained.
Vancomycin+ gentamicin, for a 6-week course is the
most common regimen( may be modified by the
results of culture).
PREVENTION : According to
(AHA 2017):
There is no evidence for IE prophylaxis in gastrointestinal
procedures or genitourinary procedures.
Prophylaxis against IE is reasonable before dental procedures that
involve manipulation of gingival tissue, manipulation of the
periapical region of teeth, or perforation of the oral mucosa in
patients with the following:
1. Prosthetic cardiac valves, including transcatheter-implanted prostheses
2. Prosthetic material used for cardiac valve repair.
3. Previous IE.
4. Unrepaired cyanotic congenital heart disease or repaired congenital heart
disease, with residual shunts or valvular regurgitation at the site of or adjacent
to the site of a prosthetic patch or prosthetic device.
5. Cardiac transplant with valve regurgitation due to a structurally abnormal
valve.
Recommended propylaxis is
50 mg/kg of oral amoxicillin for patients < 40 kg and
or 2000 mg for those > 40 kg.
This dose is to be given 1 hour prior to procedure.
If the patient is allergic to amoxicillin, alternative prophylactic antibiotics
are recommended in the AHA guidelines.
CARDIOMYOPATHIES:
-CONGESTIVE(DILATED)
-HYPERTROPHIC
-RESTRICTIVE
Dilated Cardiomyopathy
Pathophysiology
- Extensive ventricular dilatation; mostly left ventricle.
- Vast majority is idiopathic (may be familial).
- Other causes-viral infection, endocrine (hypothyroidism), metabolic
(storage disease), systemic disease (connective tissue), hereditary muscle or
neurologic disease (muscular dystrophies), abnormality of coronary arteries.
Clinical presentation
- Initially nonspecific (respiratory symptoms, failure to thrive, abdominal
complaints).
- Then findings of failure:
- Tachycardia, decreased pulse pressure, cool and pale skin, decreased
pulses, increased jugular venous pressure, hepatomegaly, edema, rales
- Cardiomegaly, mitral insufficiency, tricuspid insufficiency, gallop
rhythm
Diagnosis
- ECG-atrial enlargement, left ventricular or right ventricular enlargement;
nonspecific T-wave changes
-Chest x-ray--cardiomegaly, pulmonary congestion.
-Echocardiogram-dilatation of left atrium and left ventricle ± right
ventricle and decreased contractility; decreased flow velocity across aortic
valve with mitral regurgitation.
Prognosis : downward progression; relapse of heart
failure; emboli; ventricular arrhythmias & sudden
death.
Treatment
- Antifailure.
- Antiarrhythmic agents
- May need an implantable cardioverter-defibrillator (ICD)
-Systemic anticoagulation
-Beta blocker (metoprolol, carvedilol)
- Trial of PO carnitine (for possibility of mitochondrial disorder)
-Referral to transplant center
Supraventricular Tachycardia
The mechanisms of tachycardia are generally divided into
reentrant and automatic mechanisms and
can be described by the location of tachycardia origination.
Symptoms and Signs
Presentation varies with age. Infants tend to turn pale and mottled
with onset of tachycardia and may become irritable. With long
duration of tachycardia, symptoms of HF develop.
Older children complain of dizziness, palpitations, fatigue, and chest
pain. Heart rates range from 240–300 beats/min . HF is less
common in children than in infants. Tachycardia may be associated
with either congenital heart defects or acquired conditions such as
cardiomyopathies and myocarditis.
Electrocardiography
ECG is the most important tool in the diagnosis of SVT and to define the precise
tachycardia mechanism. Findings include a heart rate that is rapid and out of
proportion to the patient‘s physical status .. For reentrant mechanisms, the
rhythm would be extremely regular with little variability. For automatic
mechanisms, the rhythm would be less regular. The QRS complex is usually the
same as during normal sinus rhythm. The presence of P waves and their
association with the QRS are important in determining tachycardia mechanism.
With automatic tachycardias, there is often a 1:1 or 2:1 A:V relationship with P
waves preceding the QRS. With atrioventricular nodal reentrant tachycardia, P
waves cannot be identified as they are occurring at the same time as the QRS.
Acute Treatment
Close monitoring. Correction of acidosis and electrolyte
abnormalities
maneuvers: the ―diving reflex‖ produced by placing
an ice bag on the nasal bridge for 20 seconds (for infants)
or by immersing the face in ice water (for children or
adolescents) will increase parasympathetic tone and
terminate some tachycardias. The valsalva maneuver,
which can be performed by older compliant children, may
also terminate reentrant tachycardias.
1. Vagal
2. Adenosine: Adenosine transiently blocks AV
conduction and terminates tachycardias that
incorporate the AV node.. The dose is
100–250 mcg/kg by rapid intravenous bolus.
It is antagonized by aminophylline and should be used
with caution in patients with sinus node dysfunction or
asthma.
3. Transesophageal atrial pacing
4. Direct current cardioversion: (0.5–2 synchronized J/kg)
THANK YOU