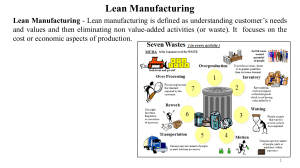
See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/271582392 “Lean occupational” safety: An application for a Near-miss Management System design Article in Safety Science · March 2013 DOI: 10.1016/j.ssci.2012.09.012 CITATIONS READS 71 6,481 4 authors, including: Maria Grazia Gnoni Serena Andriulo Università del Salento Università del Salento 89 PUBLICATIONS 999 CITATIONS 5 PUBLICATIONS 116 CITATIONS SEE PROFILE Some of the authors of this publication are also working on these related projects: Special collection on Circular Economy View project Environmental Pallets View project All content following this page was uploaded by Maria Grazia Gnoni on 10 January 2018. The user has requested enhancement of the downloaded file. SEE PROFILE (This is a sample cover image for this issue. The actual cover is not yet available at this time.) This article appeared in a journal published by Elsevier. The attached copy is furnished to the author for internal non-commercial research and education use, including for instruction at the authors institution and sharing with colleagues. Other uses, including reproduction and distribution, or selling or licensing copies, or posting to personal, institutional or third party websites are prohibited. In most cases authors are permitted to post their version of the article (e.g. in Word or Tex form) to their personal website or institutional repository. Authors requiring further information regarding Elsevier’s archiving and manuscript policies are encouraged to visit: http://www.elsevier.com/copyright Author's personal copy Safety Science 53 (2013) 96–104 Contents lists available at SciVerse ScienceDirect Safety Science journal homepage: www.elsevier.com/locate/ssci ‘‘Lean occupational’’ safety: An application for a Near-miss Management System design M.G. Gnoni a,⇑, S. Andriulo b, G. Maggio b, P. Nardone b a b Dept. of Innovation Engineering, University of Salento, Lecce, Italy Tecnologie Diesel e Sistemi Frenanti S.p.A, Bari, Italy a r t i c l e i n f o Article history: Received 1 March 2012 Received in revised form 10 September 2012 Accepted 25 September 2012 Keywords: Lean Management Occupational safety Near-miss Management System Automotive supplier firm a b s t r a c t A critical component of a safety management system is the Near-miss Management System (NMS). An effective NMS aims to recognize signals from the operational field in order to apply more effective prevention strategies. These systems are widespread in industrial contexts characterized by a high risk level, such as major hazard and hospital sectors. Few examples occur in manufacturing processes which are characterized by different operational conditions at workplace and, consequently, different risk types. The Lean Thinking (or Management) strategy currently represents a worldwide competitive tool for improving productivity in the manufacturing sector all over the world. Thus, the application of these principles forces firms to define new approaches to design and manage the whole organization and consequently the safety management system. The paper proposes innovative design of a NMS based on the integration of principles of Lean Management in occupational safety for a worldwide automotive supplier firm. As no reference model has been previously defined, several factors have been assessed aiming to efficiently integrate occupational safety in the current Lean Management system. Innovative features characterizing the proposed model have been also discussed together with first results obtained by the full scale application. Ó 2012 Elsevier Ltd. All rights reserved. 1. Introduction Recognizing signals (or precursors) before that an accident occurs, offers the potentiality to improve safety by developing effective prevention strategies; several industrial organizations all over the world have sought to develop programs to identify and benefit from both ‘‘ex ante’’ and ‘‘ex post’’ analysis. The first one refers to alerts, signals and prior indicators – usually defined as near-miss events – which allow to define more effective prevention strategies; the latter focuses on accident analysis. Both are the basis of the well known ‘‘Learning From Experience’’, LFE paradigm (Nielsen et al., 2006; Sepeda, 2006; Pasman, 2009; Dechy et al., 2012) which aims to identify knowledge derived from accident analysis as well as precursors in a structured way. The paper focuses on precursors of an accident, such as near-miss events. A near-miss event is a hazardous situation where the event sequence could lead to an accident if it had not been interrupted by a planned intervention or by a random event (Jones et al., 1999; Meel et al., 2007). Starting from pioneer studies carried out by Heinrich et al. (1980) and Bird and Germain (1966) to more recent ones (Masimore, 2007; Manuele, 2011), all authors agree with the importance ⇑ Corresponding author. Tel.: +39 832297366. E-mail address: mariagrazia.gnoni@unisalento.it (M.G. Gnoni). 0925-7535/$ - see front matter Ó 2012 Elsevier Ltd. All rights reserved. http://dx.doi.org/10.1016/j.ssci.2012.09.012 of managing efficiently near-miss events in order to improve risk prevention in a firm. The level of complexity differs managing near-miss events compared to accident events: the two types differ both quantitatively – as reported in Fig. 1 – and also qualitatively. These events point out lacks in safety system as they provide ‘‘weak signals’’: each near-miss could heavily contribute to improve the knowledge and the safety culture in several complex industrial sectors (Mason et al., 1995; Muermann and Oktem, 2002; Nivolianitou et al., 2006; Grabowski et al., 2007; Agnello et al., 2012). Currently, Near-miss Management Systems (NMSs) are widespread in process industry starting from chemical to petrochemical sectors (Van de Schaaf, 1995; Marsh and Kendrick, 2000; Phimister et al., 2003; Oktem, 2003; OECD, 2008; Koo et al., 2009) where they are mandatory on the Major Accident Hazard (MAH) legislations. Recently, few applications are developing in new industrial sectors such as construction and health care (Cambraia et al., 2010; Wu et al., 2010a, b). Several papers are facing with NMSs in the chemical sector. An interesting analysis of near-miss reporting system is proposed by Van de Schaaf (1995) in the Major Accident Hazard (MAH) context. Oktem (2003) proposed a reference schema to integrate environmental, health and safety issues in near-miss management for large chemical sites. Therefore, the application of a NMS in the manufacturing sector is not widespread as several factors have Author's personal copy M.G. Gnoni et al. / Safety Science 53 (2013) 96–104 97 Fig. 1. Traditional representation proposed by Heinrich (a) and the more recent one proposed by Massimore (b). contributed to. Firstly, according to a risk point of view, these production systems are quite different from the process industry. First of all, risk types are quite different: risk analysis in the manufacturing sector focuses on Occupational Safety and Health (OSH) hazards more than MAHs. Thus, the criticality is more on the frequency of occupational accidents rather than on the consequence analysis. According to an organizational point of view, manufacturing firms are strictly oriented to guarantee a higher level of customer satisfaction and simultaneously to reduce costs. An effective strategy applied worldwide is the Lean Thinking or Lean Management concept (Womack et al., 1990), firstly developed in Toyota production sites. In brief, the focus is to reduce ‘‘waste’’ aiming to improve productivity in all process phases. Several tools and models have been developed to support this strategy in all core process phases such as ‘‘Just in time’’, ‘‘Total productive maintenance’’, ‘‘Six sigma’’ tools. Thus, several studies have been focused on analyzing how Lean Management could support performance improvement in industrial processes (Shah and Ward, 2003; Melton, 2005; Abdulmalek and Rajgopal, 2007; Bollbach, 2010; Pettersen, 2009; Behrouzi and Wong, 2011; Yang et al., 2011; Vinodh et al., 2011). Few recent works are facing with the integration of safety issues in Lean Management approaches. Several papers regard the construction sector where these concepts seem to be more common. An interesting review analysis about the integration of occupational safety management in the lean construction sector is proposed by Ghosh and Young-Corbett (2009). Court et al. (2009) described positive impacts obtained by an UK construction firm due to an effective integration of lean principles on its health and safety management system. Nahmens and Ikuma (2009) analyzed by a survey analysis the positive perception of practitioners about the application of lean principles in order to enhance both productivity and occupational safety in the construction industry. Finally, Rozenfeld et al. (2010) proposed an innovative method for analysis and assessment hazard designed to support lean construction projects. On the other hand, very few papers analyze this prospective in the manufacturing industry. Positive contributions of Lean Management were analyzed in Brown and O’Rourke (2007): the study outlined how the intensive worker participation – i.e. typical of Lean Management – could support more effective occupational safety management as each employee has to be involved in identifying and solving problems. Moreover, authors pointed out as this feature could also contribute to reduce potential negative impacts due to frequent re-engineering of work procedures usually characterizing lean processes. On the other hand, the new paradigm could also determine potential negative impacts due to technological and organizational re-engineering (Harrisson and Legendre, 2003). Saurin and Ferreira (2009) outlined by an ergonomic study how Lean Management application affected working conditions in an assembly line of an automotive firm. This brief review highlights that new requirements for occupational safety management in Lean Management contexts: the traditional prospective has to be changed in a more proactive one as the safety level of a firm have to be ‘‘pulled’’ by actual system requirement rather than ‘‘pushed’’ uniformly into workers and procedures. The aim of the paper is to discuss an integration of Lean Management concepts in occupational safety: the proposed approach has been applied in the NMS design carried out for a worldwide automotive supplier firm. The paper has been organized as follows: a real Lean Management system is firstly discussed in Section 2 aiming to point out the complexity level of current occupational safety management system; the design of the NMS is detailed in Section 3. First results and critical discussion are in Sections 4 and 5 respectively. 2. Occupational safety management in the Bosch Lean Management system Lean manufacturing concepts were first introduced by Womack et al. (1990) aiming to describe the working philosophy and practices of Toyota, the well-known Japanese vehicle manufacturers. Nowadays, Lean Manufacturing concepts are widespread all over the world in different industrial sectors (EPA, 2000; Aitken et al., 2002; Aberdeen Group, 2006). Several operational methods could be applied in different firm activities starting from production planning to environmental issues. Nowadays, Lean Manufacturing represents a core strategy in the automotive industry: the focus is the elimination of all waste in all firm activities for improving process efficiency (Wu, 2008). The present study has been developed for international company in the automotive supply chain. In detail, the firm analyzed is the Bosch Bari Plant which produces equipment for the automotive supply chain. It is one of Bosch’s largest production sites in Europe and it is the most important Bosch factory in Italy. About 2200 people work in the plant, which produces braking systems, including the ‘common rail’ pump for diesel engines for the whole European automotive market. Few years ago, the company has designed its own Lean Management reference model – the so called Bosch Production System (BPS) – which is currently applied in about 250 plants worldwide. It represents an evolution of the original Toyota Production Systems as new concepts concerning safety and environmental protection have been introduced. Main principles constituting the BPS are depicted in Fig. 2. Differently from traditional process industries, ‘‘pull principles ’’ focus on getting flow into factories by eliminating all source of ‘‘waste’’ in order to reduce costs and guaranteeing quality and time to customers. ‘‘Personal responsibility’’ concept represents one main pillar of the BPS: each employees contribute according to its own competence to improve firm performance as the Author's personal copy 98 M.G. Gnoni et al. / Safety Science 53 (2013) 96–104 Fig. 2. Main pillars of the Bosch Production System (BPS). ‘‘Continuous Improvement Process (CIP) is the firm target. Applying CIP concepts within an organization offers the opportunity for all firm activities (e.g. production, logistics, administration, etc.) to improve day by day effectiveness of operations as synergies derived from all firm functions allow to leverage information within the firm. These ideas also heavily involve the safety management point of view as all employees have to contribute to improve the safety level at the work place. Thus, employees are encouraged to stop and solve problems when they are found; managers takes the time to help resolve issues with/for employees as they raised. Cross functional cooperation is another key factor aiming to work together. Thus, standardized and transparent processes are key factors to increase the satisfaction and motivation of all actors involved in the supply chain. By an operational point of view, the BPS has spitted up several operational tools where safety issues are directly analyzed: they are Knowledge Sources (KSs) carried out periodically in order to discuss and evaluate the CIP application also by safety management assessment. These information events could be classified in two categories: interactive and static KSs. The first one is characterized by a complete ‘‘pull’’ (i.e. bottom-up) approach where the information flow belongs directly to actors (i.e. workers) involved directly in such a process; the latter is characterized by a ‘‘push’’ (i.e. top-down) approach; the aim is to verify such a condition defined as a target level (e.g. zero injuries in a year). Three KSs belong to the first category: the so called ‘‘Yellow Line’’, ‘‘The Lernstatt’’, and the ‘‘Safety Walk’’ event. The Yellow Line event is an inspection visit carried out by managers in each plant unit once a week. The focus is to monitor about process quality and service levels and to define corrective actions if non-compliance data are verified. This represents the link between the top and the shop floor management as its frequency is very high. General issues concerning safety are also evaluated as the Health and Safety (H&S) department is also involved in the visit. Differently from Yellow Line, the Lernstatt event is a periodic meeting involving only shop floor management: all employees working in each department participate to this event one time every three weeks. Shop floor supervisors – defined as Tele for each single department and Teco for all department involved in the production process of a specific item – participate to the meeting, but they do not determine the discussion as it is based on Open Point Lists (OPLs) proposed by each participants. Main topics are production processes, quality and safety analysis. After OPL analysis, a brainstorming activity will be developed aiming to solve immediately (e.g. in the same meeting or in the next few days) at least 80% of OPL points. Finally, Safety Walk is a tour performed by a member of H&S department within the plant every day in order to verify safety level and safe behaviors. If an unsafe behavior is detected, he immediately runs corrections and, after, he registers data in order to point out common and repetitive actions or behaviors. Furthermore, two KSs belong to the static category, i.e. the so called ‘‘H&S’’ and ‘‘6S’’ audits. The first one is a well-known organizational tool applied in several firms for safety management; the latter represents a tool typical of lean organizations. H&S Audits are scheduled every 6 months in each department; the focus is to verify compliances according to such a standard (defined by a specific legislation or internally by the firm). Furthermore, the 6S Audit aims to verify the actual use of the whole BPS. As reported previously, the BPS have amplified traditional Lean Management concepts – derived from the Toyota Production systems – by introducing safety management as a focal point. Thus, ‘‘6S’’ is an acronym of critical activities, i.e. ‘‘Sort, Straighten, Sweep, Standardize, Sustain, Safety’’; differently from traditional approaches, the last element has been introduced in the BPS strategy. The 6S Audit is an inspection carried out once a month for each department by the 6S operator. A report about compliance to standard is the final output. If a significant non-compliance (e.g. involving directly safety levels) is detected, the 6S supervisor asks for support to HSE department. Main features regarding each KSs are proposed in Table 1. This brief description could support the current Bosch organization as a High Reliability Organization (HRO) according to organizational aspects of safety (Hovden et al., 2010; Saleh et al., 2010). According to Hovden et al. (2010), an HRO is based on three basic concepts: continuous training, use of redundancy, and numerous sources of direct information. Thus, new models and approaches are required for designing an effective and integrated tool for managing occupational safety. Three basic principles have been recently analyzed (Saurin et al., 2008): learning, flexibility and awareness. The first pillar refers to ‘‘learning’’: this idea is typical of Lean Management theory and it becomes critical when occupational safety issues are involved. Innovative theories – such as Cognitive Behavioral Safety Process and Cognitive Systems Engineering – are nowadays been effectively applied for safety management in several industrial complex sectors (Cox et al., 2004; Clarke, 2006; Saw et al., 2010; Fahlbruch and Schöbel, 2011). A recent study (Dechy et al., 2012) proposed an interesting critical analysis about the ‘‘Learning From Experience (LFE)’’ paradigm applied in risk management. This idea has mainly supported the development of the Lernstatt event: the focus is that crews, which are the operational level of an organization, could contribute to define and control their own accident prevention strategies by discussing their work with managers and with other workers. Near-miss Management Systems will represent one another important KS in order to identify proactive strategies to improve dynamically the occupational safety management. This concept will affect the NMS design specifically in assessing effective ways to communicate knowledge derived from event management. Furthermore, the use of flexibility concept in the current system mainly refers to the capability of first-level supervisors to carry out directly several decisions aiming to reduce waiting time unnecessarily for management instructions. This feature will heavily affects the structure of information flow in the NMS as new organizational models have to be evaluated. Finally, the awareness concept represents a basic node for the current system as it affects the CIP use in the firm: Yellow Line and Safety Walk are two innovative examples of its usage. Thus, managers – from shop floor supervisors to top management – have opportunities to assess the actual state of safety level compared with planned one. Its impact in the NMS design will force both the control phase of planned activities (i.e. evaluated after the near-miss reporting and analysis) which will be based on easy and dynamic tools. Author's personal copy 99 M.G. Gnoni et al. / Safety Science 53 (2013) 96–104 Table 1 Main features of Knowledge Sources regarding safety issues defined by the Bosch Production System (BPS). Features Interactive knowledge sources (KSs) Static knowledge sources (KSs) Yellow line Lernstatt H&S Audits 6S Audit Safety Walk Description A visit hold in rotation in each plant area A periodic meeting carried out within each shop floor An audit carried out by a checklist analysis in all areas An audit carried out by a checklist analysis hold in rotation in each plant area A quick tour in all plant areas Participants Top Management, Shop floor supervisors (if required H&S members) H&S members 6S team H&S members Frequency Once a week Shop floor employees. Supervisors and H&S members participate but they are not directly involved in the organization Once a month Every 6 months Once a month Every day Topics Process efficiency and efficacy Production process, quality and safety for applying CIP Occupational Safety and Health risks CIP targets in different areas Occupational Safety and Health risks Output Planned corrective actions and responsible for their actuation and control Open Point List for the next event, information about the state of solution of past analyzed events Statistical report about safety trends and status of application of corrective actions applied Statistical report about efficiency application of Continuous Improvement Process (CIP) strategy Report about observed unsafe event This brief discussion has pointed out both the ‘‘environment’’ where the NMS has to be fully integrated and its basic requirements in order to develop an effective lean occupational safety model. 3. The proposed Near-miss Management System design The previous analysis has outlined that currently there are several KSs where a near-miss event could be reported: on the other hand, a structured system for managing these events does not exist. Thus, the aim of the proposed study is to design an effective Near-miss Management System according to lean strategies. Recently, Oktem et al., 2010 has proposed a reference model to design NMS in the chemical sector; this is a starting point in order to develop the proposed NMS. The main phases are described in Fig. 3. The first step of NMS design is to develop the data management systems: information must be first captured and then shared among those responsible. Two main problems usually affect the Event Identification phase: the first one is to define features characterizing events as a near-miss and the second one is to increase the worker rate of reporting such an event. According to the first point, no standardized and shared definition of near-miss is proposed in the literature and in the practice (Jones et al., 1999; Phimister et al., 2003; BSI, 2007). An effective taxonomy has been provided by Cavalieri and Ghislandi (2008) which defines three types of events such as: Unsafe Act: It involves directly a specific human action. This is an action (a procedure, a task or an activity) made in a way that could cause health and/or safety levels. An example is a worker driving a forklift with an excessive speed or standing up. Unsafe Condition: It regards the state of a working area; thus, it involves indirectly several human actions. This is a condition outlined at the workplace which could cause property damages or personal injury (e.g. the lack of shelter in a machine, a broken emergency button, etc.). Near-Miss Event: This is the most close event to an accident. This is defined as any event related to work, which has the intrinsic potentiality to cause injury or damage to health, but an Fig. 3. Main phases in a NMS design. Author's personal copy 100 M.G. Gnoni et al. / Safety Science 53 (2013) 96–104 Fig. 4. Event definition in the proposed NMS. accidental chain of events has reduced its consequences. An example is that an employee slips down the stairs, but fortunately he has clung to the railing. The dynamic characterization of these three events is described in Fig. 4. Thus, this definition has been adopted for proposed NMS. Next, the second problem affects traditionally also the accident analysis process. Probst and Estrada (2010) have proposed a field analysis which quantified the higher number of unreported accidents compared to the number of reported accidents. Results showed that this phenomenon increases in working environments with poorer organizational safety climate or where supervisor safety enforcement was inconsistent. According to the analysis proposed in the previous chapter, the current organization of the firm will overcome these last two conditions. Thus, the informative flow in the whole NMS has been designed aiming to integrate effectively this system according to the BPS; it involves two phases, i.e. the Reporting and Distribution phases. The first problem affecting this activity regards the definition of a lean and smart flow: according to Lean Thinking, it has to both involve directly in event assessment first line supervisors and to guarantee a reliable assessment. Thus, the proposed informative flow starts from ‘‘sentinels’’ (i.e. each employee) that highlight an event (unsafe act or situation, or near-miss); then, the sentinel has to draw up a report, where he/she describes briefly the event. This represents the Reporting phase. Next, the informative flow design will affect the Distribution phase. Information acquired by employees are usually (e.g. in chemical or petrochemical contexts) managed by the H&S department, where safety experts analyze and define priorities of the reported events. After the analysis, the H&S department is responsible for the communication of statistics and trends about reported events in periodic meeting. It has to be noted that this is a typical ‘‘top down’’ logic; it could not be fully integrated in Lean Manufacturing contexts which are heavily based on pull approach where each worker is responsible for controlling its own job. Thus, a ‘‘bottom-up’’ approach has been applied: the event assessment has been assigned directly to the operational level (e.g. the job shop or the first line level) supervisor. Furthermore, the H&S department is not directly involved in the assessment phase, but it could support the supervisor in this activity, if its support is required by the supervisor. The proposed informative flow is detailed in Fig. 5. A worker reports an event by identifying as an unsafe act or condition, or a near-miss event. After information acquisition about the event, the shop floor supervisor classifies the event according to a predefined matrix approach. The H&S department is directly involved only when the supervisor asks a supporting activity in order to define a corrective action. The shop floor supervisor identifies both solutions and persons who will develop actions to realize corrective actions. Information about solutions applied for the near-miss are reported to all workers in different ways: this represents the Dissemination phase. The aim is to define a set of communication initiatives in order to guarantee a high level of transparency. The current application state of evaluated solutions are discussed in the Lernstatt meeting and in the Yellow Line event; statistics and trends have been recorded and analyzed in detail during periodic 6S and H&S audits. Thus, the coordinator of the monthly 6S audit shares and discusses with the H&S department data about the performance of the whole NMS. Finally, a quick communication device – defined as the ‘‘nearmiss blackboard tool’’ – has been developed in order to guarantee a quick communication for both event reporting and solution implementation. An illustrative example is given in Fig. 6. Main pillars of the proposed analysis system are Priorization, Cause analysis and Identification phase. Similarly to accident investigation, the event analysis in NMS represents a critical activity due to several factors (Maimer, 2007; Fahlbruch and Schöbel, 2011). Complex but reliable approaches (e.g. root cause analysis) usually requires a high resource effort (Sepeda, 2006; Koo et al., 2009; Cambraia et al., 2010; Saleh et al., 2010). Furthermore, the number of reported events is expected to increase comparing to traditional industrial sectors where NMS are applied, as the frequency of occupational accidents is higher in the manufacturing industry (Nenonen, 2011). Thus, a simplified assessment model has been proposed to prioritise event based on two factors: cause and consequence of the reported event. The first category is composed by three types: human error; system and procedural fault. Fig. 5. The proposed informative flow in the NMS. Author's personal copy 101 M.G. Gnoni et al. / Safety Science 53 (2013) 96–104 Fig. 6. The near-miss blackboard applied for reporting and communicating event. Consequence impact categories have been defined according to loss of productivity, potential damages to the environment, plant structures and workers. Finally, the control system has been analyzed: it involves the Resolution phase. The main purpose is twofold: defining a quick and easy tool to monitor the state of corrective action application. It has to be noted that identified corrective actions could be applied immediately or require longer time; thus, a check procedure has to be defined. The proposed solution is based on the well-known ‘‘traffic light’’ technique: each near-miss supervisor elaborates on a monthly basis statistics about events which could be classified in three conditions: – Green Status: It is associated to closed events, i.e. an event where prevention actions have been already applied and verified. – Yellow Status: This represents the ‘‘work in progress’’ as it is associated to events which actions have been planned but the due date is not yet reached. – Red Status: This is the most critical one as the due date is passed but actions have not been fully applied. These statistics are discussed during specific KSs as reported previously in this section. 4. The application and first results The proposed model for NMS design has been applied in the firm. After a preliminary training period when H&S experts have explained main features characterizing the NMS and its procedures, the NMS has started to work in one assembly department of the Bosch Bari Plant on September 2011; at December 2011, all production departments at Bosch Bari Plant were subsequently involved; the total number of workers involved in the project were about 750. The application has revealed effective as employee participation rate is quite high. Thus, the total number of reported event from September 2011 to February 2012 are 67; the distribution is in Fig. 7. Unsafe Conditions (UCs) event represents the largest category (i.e. with a total number of 42 events) of reported event. Unsafe Act (UA) and Near-Miss (NM) reported evens are quite similar (i.e. 12 and 13 respectively). Reported information about factors applied for event priorization are not reported in this study for confidential issues; furthermore, data have been analyzed according to two main factors: the source and type of hazards estimated for the reported event. In detail, work equipment, work procedure and safety devices have been defined as the three main sources of hazard by analyzing the total number of reported events. Four main typologies of hazards have been outlined: instability (e.g. an heavy weight in a forklift), layout (e.g. a not accurate localization of a fire extinguisher), dangerous substances (e.g. a loss of Fig. 7. Distribution of events reported from September 2011 to February 2012 at Bosch Bari Plant. Table 2 Data about reported event classified according to event type, source and type of estimated hazard categories. Safety devices Unsafe Act (UA) Instability Layout Dangerous substances Fault Total Unsafe Conditions (UC) Instability Layout Dangerous substances Fault Total Near-Miss (NM) Instability Layout Dangerous substances Fault Total Work equipment Work procedure 0 0 0 1 0 6 0 1 0 1 1 2 9 1 2 0 2 0 12 11 0 0 5 0 3 5 8 31 1 6 0 0 0 2 2 1 3 0 0 1 1 4 9 0 3 oil near to machine), and faults (e.g. a breakdown of an emergency button). Data are reported in Table 2 for each type of event. According to hazard type, ‘‘Layout’’ and ‘‘Fault’’ represent the largest categories with a percentage about of 31% of the total reported events; a little lower value (about 27%) characterizes ‘‘instability’’. The higher number of reported events under the category ‘‘layout’’ could be Author's personal copy 102 M.G. Gnoni et al. / Safety Science 53 (2013) 96–104 due to the crowded layout usually characterizing manufacturing firms. The category ‘‘instability’’ refers mainly to finished or semi-finished product transportation within different plant areas. The presence of dangerous substances is the last category characterized by a reduced value (i.e. about 11%). This is mainly due to the type of process (i.e. an assembly plant) where usually the presence of hazardous substances is not frequent as chemical or petrochemical sectors. Furthermore, ‘‘work equipment’’ represents the largest category of hazard source with about 73% of the total reported events: thus, machines and work tools represent the first source of potential hazard in the firm. This condition is also confirmed by a more detailed analysis based on each single type of event: ‘‘work equipment’’ represents for both unsafe act, conditions and near-miss the largest category of hazard source. Furthermore, a good performance of the current safety management system is outlined by both the relative low percentage (about 16%) due to ‘‘work procedure’’ and the score obtained by ‘‘safety devices’’ with a percentage about 11%. By crossing data about type and source of hazards, several interesting results could be outlined. The most estimated hazardous condition is due to instability of a work equipment (i.e. 15 of total 67 events), which confirms the previous analysis; fault and layout also reveal as significant categories for this hazard source. By evaluating each hazard source, the major hazard type for safety device is due by fault; layout represents the second one. Thus, proactive strategies aiming to increase safety device availability could contribute heavily to control risk level of safety devices. Layout represents the major hazard type category for work procedures. Medium or long term decisions aiming to optimize the layout design could contribute to reduce this potential hazardous conditions. Next, data have been analyzed according to each type of event, i.e. unsafe act, condition or near-miss. For Unsafe Condition, the general statement is confirmed as instability of work equipment represents the most hazardous reported event. Differently from the previous analysis, the largest reported category for unsafe acts is due to the presence of dangerous substances close to a work equipment. The largest category for near-miss is due to fault of a work equipment which is quite in line with general results; on the other hand, data shows a (relative) relevant criticality to work procedure. Finally, a statistical analysis has been carried out aiming to assess relative influences between hazard type and source. As the number of total observed events is not too high (i.e. less than 70) and no assumptions about the distribution of the data could be carried out, the Friedman test (Friedman, 1937; Wasserman, 2006) has been applied to compare data: it is a non-parametric test (distribution-free) applied similarly to ANOVA test with two factors if a parametric test will be applied. Like many non-parametric tests, it uses the ranks of the data rather than their raw values to calculate the statistic. Ranking values obtained based on hazard type cate- Table 3 Absolute observed values and their estimated ranking (in brackets) according to hazard type. Hazard type (N) Hazard source (k) Safety devices Work equipment Work procedure Instability Layout Dangerous substances Fault 0 (1) 2 (1) 0 (1.5) 15 (3) 13 (3) 7 (3) 3 (2) 6 (2) 0 (1.5) 5 (2) 14 (3) 2 (1) Total 7 (5.5) 49 (12) 11 (6.5) Table 4 Absolute observed values and their estimated ranking (in brackets) according to hazard source. Hazard source (N) Hazard Type (k) Instability Layout Dangerous substances Fault Safety devices Work equipment Work procedure 0 (1.5) 15 (4) 3 (3) 2 (3) 13 (2) 6 (4) 0 (1.5) 7 (1) 0 (1) 5 (4) 14 (3) 2 (2) Total 18 (8.5) 21 (9) 7 (3.5) 21 (9) gory are reported in Table 3; values estimated according to hazard source category are in Table 4. Thus, the test procedure first ranks the values in each matched set (i.e. each row) from low to high. Each row is ranked separately. It then sums the ranks in each group (i.e. column). The aim of the test is to verify the null hypothesis (H0): the distributions are the same across repeated observations. Next, the Fr index has to be evaluated according to Eq. (1): Fr ¼ k X Ti i¼1 Nðk þ 1Þ 2 2 ð1Þ where k represents the column index (which refers to treatments), n represents the row index (which refers to blocks). N represents the row index (which refers to blocks) value; and Ti is the absolute value derived from observations. Finally, Fr values have to be compared to critical ones (defined by Friedman): if Fr < FrCR, the H0 hypothesis is true; thus, the k treatments do not affect the distribution of observed block (N-th)values. By referring to Table 3 where hazard source represents the ‘‘treatment’’, k is equal to 3 and N is equal to 4: expected Ti value is equal to 8; the estimated Fr value is 24.5. According to values defined by Friedman, the critical FrCR value is 26 with a probability value a = 0.05. Thus, the H0 hypothesis is confirmed: there is no statistical difference between the three hazard sources. Indexes have been calculated based on hazard type: now, k is equal to 4 and N is equal to 3 as reported in Table 4. The expected Ti value is equal to 7.5; the calculated Fr value is 21.5 and the FrCR is equal to 37 with a probability value a = 0.05. The estimated Fr value is again lower than the critical one: thus, hazard type does not affect the hazard source. It has to be noted that this brief statistical analysis has been carried out on a reduced sample of observations; further development could be oriented to apply parametric statistical models when more observations will be available. 5. Discussion The application of the proposed model has provided several discussion points. First of all, innovative features introduced in the proposed system are analyzed. Unlike from traditional NMSs, a ‘‘pull’’ logic has been fully applied in all phases of the system design: this is a compulsory requirement in order to integrate the NMS into the Lean Management systems developed in the plant. Thus, the most innovative feature is due to the informative flow structure proposed in the NMS: a comparison between traditional structures versus the proposed one is in Fig. 8. The H&S department usually carries out the near-miss analysis as the assessment process is carried out by safety expert. This structure does not be well-suited with Lean Management which requires a high level of worker involvement starting from the operational level. Thus, the assessment phase will be carried out directly by an operative level such as shop floor managers and the HSE department will be involved only if a more specialist support is needed in order Author's personal copy M.G. Gnoni et al. / Safety Science 53 (2013) 96–104 103 Fig. 8. Proposed versus traditional organization of the analysis phase in the NMS design. to evaluate such a solution. This proposed solution will guarantee a higher level of awareness of both shop-floor supervisors and workers in event management. On the other hand, this also represents a limit characterizing the proposed system: this organization requires a great time effort in training supervisors – who are usually not safety experts – to carry out event analysis. Furthermore, a simplified model for cause analysis has been proposed: further developments could be oriented to re-design the model aiming to acquire more knowledge from reported events. A software tool that could integrate reporting and analysis phase will be helpful especially due to the large volume of events reported in the firm. Furthermore, LFE approach has been fully integrated in the proposed NMS by defining different knowledge sources, such as periodic audits and meetings (e.g. the 6S audit and the Lernstatt) together with visual interactive tools (e.g. the Near-miss blackboard tool). The aim of the proposed model is to fully involve all stages of the organization in managing information derived from each event thus improving knowledge sharing than traditional systems. This represents an innovative feature as dissemination activities in traditional NMS are usually carried out by the H&S department during formal periodic meetings. A potential pitfall of this system is that it requires a huge effort of the firm management (Gnoni and Lettera, 2012): this system could be effective only with a full involvement of all levels of management from top managers to first live supervisors in monitoring day by day the system performance. As an example, at Bosch Bari Plant, the plant manager is informed about each reported event in the NMS Furthermore, an intensive training period carried out by H&S safety experts has been implemented in rotation with each production department in order to train and inform each form and inform workers about how to recognize and report an event. In this application, these issues have been not so critical as the Lean Thinking is now fully integrated in each worker thinking as it has been applied for three years; thus, this new way of thinking has been acquired starting from top manager to employee level. Much effort could be required in different production environment where lean philosophy is not yet applied. 6. Conclusions Near-miss Management Systems (NMSs) are widespread in sectors characterized by Major Accident Hazards, MAH, (e.g. the chemical or petrochemical industry) as they are usually compulsory for these firms. Few applications are developing in other industrial sectors; they are currently rare in the manufacturing industry mainly due to legislative compulsory is not required and no reference standard is defined. On the other hand, NMSs represent an effective tool to apply Learning From Experience (LFE) concepts in occupational safety management. Consequently, designing a NMS for a manufacturing company is quite a complex problem as several factors have to be evaluated. First of all, traditional models applied for MAH sector could not be applied ‘‘as is’’ in the manufacturing industry: several features are quite different starting from risk type and their frequency to the firm organization and structure. In brief, occupational safety management system requires different approaches and expertise. This becomes imperative when Lean Management paradigm is fully applied. The paper proposed an application of lean occupational safety paradigm in the design process of a NMS. The system has been developed for an automotive supplier firm which has settled its own reference model to apply lean strategies. The application has revealed effective as the proposed structure of the NMS have been fully applied in all firm departments. First encouraging results have been obtained by the firm in order to support continuous improvement process for its own occupational safety management system. Acknowledgments Authors are grateful for suggestions supplied by anonymous reviewers. References Abdulmalek, F.A., Rajgopal, J., 2007. Analyzing the benefits of lean manufacturing and value stream mapping via simulation: a process sector case study. Int. J. Prod. Econ. 107, 223–236. Aberdeen Group, 2006. The Lean Supply Chain Report. Lean Concepts Transcend Manufacturing through the Supply Chain. Agnello, P., Ansaldi, S.M., Bragatto, P.A., 2012. Plugging the gap between safety documents and workers perception, to prevent accidents at seveso establishments. Chem. Eng. Trans. 26, 291–296. Aitken, J., Christopher, M., Towill, D., 2002. Understanding, implementing and exploiting agility and leanness. Int. J. Logist.: Res. Appl. 5 (1), 59–74. Behrouzi, F., Wong, K.Y., 2011. An investigation and identification of lean supply chain performance measures in the automotive SMEs. Sci. Res. Essays 6 (24), 5239–5252. Bird, F.E., Germain, G.L., 1966. Damage Control. American Management Association, New York. Bollbach, M., 2010. Implementing Lean manufacturing techniques in China A consideration of country-specific barriers to implementing lean manufacturing in China. In: 21st Chinese Economic Association Annual Conference, UK. Brown, G.D., O’Rourke, D., 2007. Lean manufacturing comes to China: a case study of its impact on workplace health and safety. Int. J. Occup. Environ. Health 13, 249–257. British Standards Institution (BSI), 2007, OHSAS 18001:2007 – Occupational Health and Safety Management Systems. Requirements. Cambraia, F.B., Saurin, T.A., Formoso, C.T., 2010. Identification, analysis and dissemination of information on near-misses: a case study in the construction industry. Safety Sci. 48 (1), 91–99. Author's personal copy 104 M.G. Gnoni et al. / Safety Science 53 (2013) 96–104 Cavalieri, S., Ghislandi, W.M., 2008. Understanding and using near-misses properties through a double-step conceptual structure. J. Intell. Manuf. 21 (2), 237–247. Clarke, S., 2006. Contrasting perceptual, attitudinal and dispositional approaches to accident involvement in the workplace. Safety Sci. 44, 537–550. Court, P.F., Pasquire, C.L., Gibb, A.G.F., 2009. A lean and agile construction system as a set of countermeasures to improve health safety and productivity in mechanical and electrical construction. Lean Construction Journal, 61–76. Cox, S., Jones, B., Rycraft, H., 2004. Behavioural approaches to safety management within UK reactor plants. Safety Sci. 42, 825–839. Dechy, N., Dien, Y., Funnemark, E., Roed-Larsen, S., Stoop, J., Valvisto, T., Vetere Arellano, A.L., 2012. Results and lessons learned from the ESReDA’s accident investigation working group introducing article to ‘‘Safety Science’’ special issue on ‘‘Industrial Events Investigation’’. Safety Sci. 50 (6), 1380–1391. Environmental Protection Agency (EPA), 2000. Pursuing Perfection: Case Studies Examining Lean Manufacturing Strategies, Pollution Prevention, and Environmental Regulatory, Management Implications. Fahlbruch, B., Schöbel, M., 2011. SOL – Safety through organizational learning: a method for event analysis. Safety Sci. 49 (1), 27–31. Friedman, M., 1937. The use of ranks to avoid the assumptions of normality implicit in the analysis of variance. J. Am. Stat. Assoc. 32, 675–701. Ghosh, S., Young-Corbett, S., 2009. Intersection between lean construction and safety research: a review of the literature. In: Proceedings of the 2009 Industrial Engineering Research Conference, Miami, Florida, May 30–June 3. Gnoni, M.G., Lettera, G., 2012. Near-miss management systems: a methodological comparison. J. Loss Prev. Process Ind. 25 (3), 1–8. Grabowski, M., Ayyalasomayajula, P., Merrick, J., Harrald, J.R., Roberts, K., 2007. Leading indicators of safety in virtual organizations. Safety Sci. 45, 1013–1043. Harrisson, D., Legendre, C., 2003. Technological innovations, organizational change and workplace accident prevention. Safety Sci. 41, 319–338. Heinrich, H.W., Petersen, D., Roos, N.R., Hazlett, S., 1980. Industrial Accident Prevention: A Safety Management Approach, fifth ed. Mc-Graw Hill, New York. Hovden, J., Albrechtsen, E., Herrera, I.A., 2010. Is there a need for new theories, models and approaches to occupational accident prevention? Safety Sci. 48 (8), 950–956. Jones, S., Kirchsteiger, C., Bjerke, W., 1999. The importance of near-miss reporting to further improve safety performance. J. Loss Prev. Process Ind. 12, 59–67. Koo, J., Kim, S., Kim, H., Kim, Y., Yoon, E.N., 2009. A systematic approach towards accident analysis and prevention. Korean J. Chem. Eng. 26 (6), 1476–1483. Maimer, H., 2007. Learning from events – experience with an electronic tool supporting the report of events, evaluation, analysis, and the corrective action program. In: 8th IEEE Conference on Human Factors and Power Plants, pp. 1–3. Manuele, F.A., 2011. Reviewing Heinrich dislodging two myths from the practice of safety. Prof. Saf., 52–61. Marsh, P., Kendrick, D., 2000. Near miss and minor injury information – can it be used to plan and evaluate injury prevention programmes? Accid. Anal. Prev. 32, 345–354. Masimore, L., 2007. Proving the Value of Safety Justification and ROI of Safety Programs and Machine Safety Investments, Rockwell Automation. Mason, E., Roberts, K., Bea, R., 1995. Reduction of Tanker Oil and Chemical Spills: Development of Accident and Near-Miss Databases. Available at <http:// nsgd.gso.uri.edu/cuimr/cuimrt95003.pdf> (accessed 10.10.11). Meel, A., O’Neill, L.M., Levin, J.H., Seider, W.D., Oktem, U., Keren, N., 2007. Operational risk assessment of chemical industries by exploiting accident databases. J. Loss Prev. Process Ind. 20 (2), 113–127. Melton, T., 2005. The benefits of lean manufacturing. What lean thinking has to offer the process industries. Chem. Eng. Res. Des. 83 (A6), 662–673. Muermann, A., Oktem, U., 2002. The near-miss management of operational risk. J. Risk Finance (Fall), 25–37. Nahmens, I., Ikuma, L.H., 2009. An empirical examination of the relationship between construction and safety in the industrialized housing. Lean Constr. J., 1–12. Nenonen, S., 2011. Fatal workplace accidents in outsourced operations in the manufacturing industry. Safety Sci. 49 (10), 1394–1403. View publication stats Nielsen, K.J., Carstensen, O., Rasmussen, K., 2006. The prevention of occupational injuries in two industrial plants using an incident reporting scheme. J. Safety Res. 37, 479–486. Nivolianitou, Z., Konstandinidou, M., Kiranoudis, C., Markatos, N., 2006. Development of a database for accidents and incidents in the Greek petrochemical industry. J. Loss Prev. Process Ind. 19 (6), 630–638. Organisation for Economic Cooperation and Development (OECD), 2008. Guidance on Developing Safety Performance Indicators Related to Chemical Accident Prevention, Preparedness and Response, Series on Chemical Accidents, No. 18. Oktem, G., 2003. Near-miss: a tool for integrated safety, health, environmental and security management. In: 37th Annual AIChE Loss Prevention Symposium (March 30–April 3). Oktem, G., Wong, R., Oktem, C., 2010. Near-Miss Management: Managing the Bottom of the Risk Pyramid, Risk & Regulation-Magazine of the ESRC Centre for Analysis of Risk and, Regulation, pp. 12–13. Pasman, H.J., 2009. Learning from the past and knowledge management: are we making progress? J. Loss Prev. Process Ind. 22 (6), 672–679. Pettersen, J., 2009. Defining lean production: some conceptual and practical issues. Total Qual. Manage. J. 21 (2), 127–142. Phimister, J.R., Oktem, U., Kleindorfer, P.R., Kunreuther, H., 2003. Near-miss incident management in the chemical process industry. Risk Anal. 23, 445–459. Probst, T.M., Estrada, Armando X., 2010. Accident under-reporting among employees: testing the moderating influence of psychological safety climate and supervisor enforcement of safety practices. Accid. Anal. Prev. 42 (5), 1438– 1444. Rozenfeld, O., Sacks, R., Rosenfeld, Y., Baum, H., 2010. Construction job safety analysis. Safety Sci. 48 (4), 491–498. Saleh, J.H., Marais, K.B., Bakolas, E., Cowlagi, R.V., 2010. Highlights from the literature on accident causation and system safety: Review of major ideas, recent contributions, and challenges. Reliab. Eng. Syst. Safety 95 (11), 1105– 1116. Saurin, T.A., Ferreira, C.F., 2009. The impacts of lean production on working conditions: a case study of a harvester assembly line in Brazil. Int. J. Ind. Ergon. 39 (2), 403–412. Saurin, T.A., Formoso, C.T., Cambraia, F.B., 2008. An analysis of construction safety best practices from a cognitive systems engineering perspective. Safety Sci. 46 (8), 1169–1183. Saw, J.L., Wilday, J., Harte, H., 2010. Learning organisations for major hazards and the role of the regulator. Process Safety Environ. Prot. 88 (4), 236–242. Sepeda, A.L., 2006. Lessons learned from process incident databases and the process safety incident database (PSID) approach sponsored by the center for chemical process safety. J. Hazard. Mater. 130, 9–14. Shah, R., Ward, P.T., 2003. Lean manufacturing: context, practice bundles, and performance. J. Oper. Manage. 21 (2), 129–149. Van de Schaaf, T.W., 1995. Near-miss reporting in the chemical process industry: an overview. Microelectron. Reliab. 35 (9–10), 1233–1243. Vinodh, S., Arvind, K.R., Somanaathan, M., 2011. Tools and techniques for enabling sustainability through lean initiatives. Clean Technol. Environ. Policy 13 (3), 469–479. Wasserman, L., 2006. All of Nonparametric Statistics. Springer Science, New York, USA. Womack, J.P., Jones, D.T., Roos, D., 1990. The machine that changed the world. Sloan Manage. Rev.. Wu, T., 2008. Responsive lean supply chain. Case study in a Japanese vehicle manufacturer in the UK. In: 19th Annual Conference POMS (May 2008). Wu, W., Yang, H., Chew, D.A.S., Yang, S., Gibb, A.G.F., Li, Q., 2010a. Towards an autonomous real-time tracking system of near-miss accidents on construction sites. Automat. Constr. 19 (2), 134–141. Wu, W., Gibb, A.G.F., Li, Q., 2010b. Accident precursors and near-misses on construction sites: an investigative tool to derive information from accident databases. Safety Sci. 48 (7), 845–858. Yang, M., Hong, P., Modi, S.B., 2011. Impact of lean manufacturing and environmental management on business performance. An empirical study of manufacturing firms. Int. J. Prod. Econ. 129 (2), 251–261.