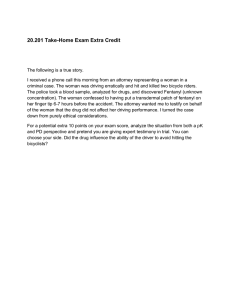
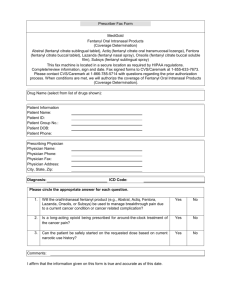
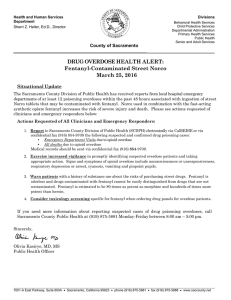
An Analysis of the Duration of Fentanyl and Its Metabolites in Urine and Saliva Jeffrey H. Silverstein, MD*, Michael F. Rieders, PhDZ, Matthew McMullin, Schulman, MD*, and Kenneth Zahl, MD* M S ~ ,Steven Downloaded from https://journals.lww.com/anesthesia-analgesia by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCywCX1AWnYQp/IlQrHD3oaxD/vH2r75cqY/N9Lh8kApVy9arH+izTq2icYQDOpE= on 09/04/2020 *Departmentof Anesthesiology, The Mount Sinai Medical Center, New York, New York and $National Medical Services, Inc., Willow Grove, Pennsylvania This study was undertaken to determine if metabolites of fentanyl might be useful in the detection and monitoring of substance abuse. The presence of fentanyl and two of its metabolites in the urine and saliva of seven female patients receiving small doses (110 ? 56 pg) of fentanyl was studied up to 96 h from the time of administration. Fentanyl and its two metabolites (norfentanyl and despropionylfentanyl) were extracted from samples and analyzed by gas chromatography/ mass spectrometry. Unchanged fentanyl was detectable in urine in all patients immediately postoperatively and in 3 of 7 patients at 24 h. By 72 h, fentanyl U rine testing is presently fundamental to the detection and monitoring of chemically dependent individuals (1). Fentanyl is the drug of choice for addicts in the anesthesia workplace (2). Due to its short elimination half-life (t"P = 219 min) and approximately 90% metabolism (31, fentanyl is difficult to detect in urine. Murphy et al. suggested that norfentanyl would persist in the urine (4), and Hammargren and Henderson, using a difficult extraction and detection method, were able to demonstrate the presence of both fentanyl and norfentanyl in urine (5). The time course of the presence of these compounds in urine or saliva and the feasibility of using these methods as a monitor for substance abuse have not been evaluated. We tested urine and saliva for the presence of fentanyl and two of its metabolites (norfentanyl and despropionylfentanyl) (Figure 1) from individuals receiving less than 400 pg of fentanyl as a component of intravenous analgesia for outpatient surgery. We sought to determine the feasibility of using this method as a surveillance test or screen for ~ ~~~~ ~~ Presented in part at the Annual Meeting of the American Society of Anesthesiologists,San Francisco, California,October 1991. Accepted for publication September 29, 1992. Address correspondenceand reprint requests to JeffreyH. Silverstein, MD, Department of Anesthesiology, Box 1010, Mount Sinai Medicaf Center, I Gustave L. Levy PIace, New York, NY 10029-6574. was undetectable. Norfentanyl was present in larger quantities than fentanyl immediately postoperatively and was detected in all patients at 48 h and in 4 of 7 patients at 96 h. Despropionylfentanyl was not detected in any of the urine specimens tested. Neither fentanyl nor its metabolites could be detected consistently at any time in saliva. Saliva testing does not appear to be a viable alternative to urine testing based on this study. Urinary norfentanyl might be considered as the substance of choicewhen testing for fentanyl abuse. (Anesth Analg 1993;76:618-21) chemically dependent individuals and to determine if saliva would provide a viable alternative for the detection of fentanyl and its metabolites. Methods This study was approved by the Institutional Review Board of The Mount Sinai Medical Center and informed consent was obtained from all participants. ASA I and I1 patients presenting for ovum retrieval were included in this study. Seven female patients who received less than 400 pg of fentanyl for operative analgesia were eligible for participation. The anesthetic regimen for ovum retrieval consisted of intravenous sedative/analgesic technique with incremental bolus doses of fentanyl, midazolam, thiamylal, propofol, lidocaine, and /or droperidol. Medications used in conjunction with fentanyl were not analyzed in the study, but were determined not to interfere with the analytical method (data not shown). Participants were asked to provide urine (10-mLbottles) and saliva (1teaspoon or approximately 4 mL) specimens preoperatively, immediately postoperatively, and subsequently at 12,24,48, 72, and 96 h. Urine and saliva specimens were stored at -4°C (for sanitary reasons) and shipped frozen (-20°C) to one of the authors for analysis. Fentanyl and its two metabolites were extracted from patient samples using pH-controlled acid-base, 01993 by the International Anesthesia Research Society 618 he& Analg 1993;7661€&21 0003-2999/93/$5.00 ANESTH ANALG iw3;76:61azi SILVERSTEIN ET AL. DURATION OF FENTANYL. METABOLITES IN URINE Fentanyl and Metabolites 619 Table 1. Method Validation Fentanyl Norfentanyl 0 Limit of detection (ng/mL) Reporting limit (ng/mL) Run-to-run precision at 10 ng/mL (% coefficient of variance) Accuracy (at 10 ng/mL) Analvte stabilitv at -10°C Fentanyl Norfentanyl Despropionylfentanyl Figure 1. Fentanyl is metabolized in the body to norfentanyl and despropionylfentanyl. Two other metabolites, hydroxyfentanyl and norhydroxyfentanyl, which are found in lower quantities in human serum, were not evaluated in this study. solvent extraction and back extraction (6-8). The extracted internal standard utilized was 8-methoxyloxapine (8-MLOX) (Aldrich Chemical Company, Milwaukee, WI). Aliquots (2 mL) of standards, controls, blanks, and patient samples were placed into tubes. One milliliter of 10% sodium hydroxide and 100 pL of 8-MLOX (10 ng/100 pL) were added to each tube. After equilibration for 5 min, 4 mL of water/ isopropanol (3:2, v/v), plus 6 mL of petroleum ether were added. The tubes were capped and rotomixed for 10 min at 20 rpm, centrifuged for 5 min at 1400 g, and allowed to stand for 10 min. The upper layer was transferred carefully to a tube containing 2 mL of 0.05 N HC1. The tubes were vortexed for 1 rnin, then centrifuged for 5 min at 1400 g. The lower aqueous layer was transferred to a tube containing 0.2 mL of 5%NaOH, and the tubes were briefly vortexed. Final extraction was achieved by adding 0.3 mL of dichloromethane, vortexing for 1min, and then centrifuging for 2 min at 1400 g. The bottom organic layer, containing fentanyl and its metabolites, was transferred to a new tube for analysis. Norfentanyl and despropionylfentanyl were derivatized by adding 5 pL of a mixture of to1uene:butyric anhydride:4-dimethylaminopyridine(catalyst) (90:9:1) to each tube. The tubes were heated at 70°C for 22 min under a stream of nitrogen to prevent oxidation. The residue was reconstituted with 30 pL of toluene and transferred to an auto sampler vial and sealed with a crimp top. Gas chromatographic (GC) analyses were performed with a Hewlett-Packard Model 5890A GC equipped with a nitrogen phosphorus detector (GC/ NP), 7673A liquid auto sampler,and a 3396A integrator. The injections were made in the splitless mode into a 4-mm glass injection port liner, followed by an analytical 15-m X 0.32-mm internal diameter fused silica capillary column with a bonded 0.15-pm DB-17 film U&W 0.1 0.2 5.9 0.1 0.2 6.3 +8.3% >6 mo >6 mo *9.7% Scientific, Folsom, CA). The operating conditions were a helium carrier gas at a head pressure of 10.0 psi, column oven temperature programmed from 150°C to 300°C at 35"C/min, final time 1 min, initial and inlet purge time were both 2 min, injector and detector temperatures were 270°C and 300"C, respectively. The volume injected on the column was 2 pL. Gas chromatographic/mass spectral (GC/MS) analyses were performed on a Hewlett-Packard Model 5988A system using the same chromatographic parameters described above. The electron impact mass spectral data were acquired in the selected ion monitoring mode (SIM) for the following ions (rn/z>:fentanyl, 146, 189, 245; norfentanyl, 132, 158, 231; despropionylfentanyl, 146, 189, 259; 8-MLOX, 247, 287 (5). The manufacturer's certified primary standards utilized were: fentanyl citrate (Janssen Pharmaceutica, Piscataway, NJ), despropionylfentanyl, and norfentanyl (Goldmark Biologicals, Phillipsburg, NJ). Fentanyl, norfentanyl, despropionylfentanyl, and 8-MLOX demonstrated baseline separation in this chromatographic system with typical retention times of 6.85, 6.22, 7.01, and 7.37 min, respectively. All specimens were analyzed by GC/NP. Those specimens that were initially positive for fentanyl and/or its metabolite(s1were analyzed by GC/MS for confirmation of identity and quantitation. A representative sampling of negative patient specimens were run as blank controls along with the positive patient samples for both GC/NPand GC/MS. The validation characteristics for the assays of fentanyl and norfentanyl are presented in Table 1. Results A representative GC/NP chromatogram is presented in Figure 2. Demographicdata and results for each subject are presented in Table 2. The mean fentanyl dose administered was 110 ? 56 pg. The specimens were collected at the times requested 2 2 h as reported by the participants. The reporting limit for this assay is 0.2 ng/mL for both fentanyl and norfentanyl. Samples reported as negative represent levels <0.2 ng/mL. Fentanyl was detected in all immediate postoperative urine specimens, in 3 of 7 specimens at 12 and 24 h, and 620 -TI4 SLVERSTEIN ET AL. DURATION O F FENTANYL METABOLITES IN URINE ANALG 1993;7661&21 Table 2. Demographic Data and Results Urine norfentanyl (ng/mL) Urine fentanyl (ng/mL) Other Age (yr)" Fentanyl ( p g ) b medications' Postop 12 h 24 h 48 h 72 h 96 h Postop 12 h 24 h 48 h 72 h 96 h 35 43 200 170 32 100 38 100 40 100 38 50 42 50 M 4 mg M 4 mg D1.25 M 4 mg L 25 mg T 250 mg M 2 mg P 90 mg L 50 mg M 2 mg D 0.25 mg T 250 mg M 4 mg P 100 mg D 1.25 mg M 4 mg P 150 mg D 1.25 mg 0.8 2.0 0.2 0 0 0.2 0.9 0 0 0 0 5.8 5.4 13.8 3.7 5.3 1.9 4.7 2.6 1.3 0.2 0.3 0 0.9 0 0 0 0 0 11.5 10.2 3.1 1.7 0.7 0.7 0.5 0 0 0 0 0 10.9 7.6 0 0.5 0 0 4.7 0.4 0.4 0 0 0 10.0 23.0 3.3 0.8 0.6 0.5 1.9 0.3 0.6 0 0 0 8.5 20.0 12.0 0.4 0.7 0 0.8 0 0 0 0 0 10.0 0.6 0.4 0.6 1.1 0 0 , Average age = 38.3 i 3.9 yr. Average fentanyl dose = 110 i 56 pg. M = midazolam; P = prupofol; T = thiamylal; D = droperidol; L = Lidocaine. in one specimen at 48 h. Fentanyl could not be detected at 72 or 96 h. By contrast, norfentanyl was detected in greater quantities at all times and in 4 of 7 samples at 96 h (Figure 3). Despropionylfentanylwas not detected in any of the urine specimens. Initial screening of the preoperative specimen from one patient was positive by GC/NP for norfentanyl (0.7 ng/mL), but GC/MS analysis did not confirm the initial positive GC/NP screen. The requested quantities of saliva, 5 mL, proved difficult to obtain and quantities of 1-2 mL were typically produced. Neither fentanyl nor despropionylfentanyl were detected in any saliva specimens. Norfentanyl was detected in two saliva specimens from one patient who received 100 pg of fentanyl, but could not be detected in any of the other 43 specimens. II f Q l - I I/ a Figure 2. Gas chromatographic/nitrogen phosphorus chromatograph showing separation of fentanyl and three metabolites and 8-methoxyloxapine (8-MLOX), the internal standard. The numbers represent retention times on the chromatographiccolumn. Discussion In this study, seven female patients undergoing ovum retrieval received analgesia with 1200 pg of fentanyl. Urine and saliva specimens were analyzed for the presence of fentanyl and two of its metabolites, norfentanyl and despropionylfentanyl. Our results are consistent with the known disposition of fentanyl in humans which involves excretion of approximately 90% of an administered dose as metabolites (5).At 72 h, fentanyl could not be detected in any urine sample, but norfentanyl was detected in 86% of samples. Despropionylfentanyl was not detected at any time in any of the urine specimens in this study. Hammargren and Henderson described a different extraction and detection procedure for fentanyl and norfentanyl(5). They evaluated an unspecified number of individuals, but did not determine the time course of the presence of these normetabolites in urine. McClain and Hug (3) and Murphy et al. (4)suggested that norfentanyl would persist in urine as confirmed by our results. The doses of fentanyl used in this study (50-200 pg) are small compared to the quantities that may be used by a fentanyl addict. Our interest is the monitoring of the recovering addict as well as the detection of the early addict. The doses studied are appropriate to these situations. Fentanyl metabolism and excretion into urine were highly variable among individuals. There was no discernible relationship between the administered fentanyl dose and the levels SKVERSTEIN ET AL. DURATION OF FENTANYL METABOLITES I N URINE Duration of Norfentonyl a n d Fentanyl in Urine 20 means i S D . 18 0 Norfentonyl 16 Fentoriyi c.1 4 E \ y 12 c .? 10 0 c 8 6 4 2 0 I 1 v ~ POST-OP 1 2 HOURS 24 HOURS 48 HOURS 72 HOURS 9 6 HOURS Collection Time Figure 3. Utilizing an assay with a reporting limit of 0.2 ng/mL, norfentanyl was detected in 4 of 7 samples at 96 h. Fentanyl levels approached the reporting limit by 12 h. of fentanyl and norfentanyl detected in urine. Some of the variability may be attributable to differences in urine specific gravity or creatinine clearance. The effect, if any, of the other coadministered drugs on fentanyl metabolism and excretion is not known. Although the present study included only female subjects, there are no data to suggest that fentanyl metabolism is significantly different in males. Other medications coadministered for sedation (Table 2) were not monitored or analyzed in this study. It was determined, however, that neither these substances nor other common substances of abuse interfere with the quantitative identification of fentanyl or its metabolites (data not shown). Because individuals who abuse drugs frequently abuse more than one substance, the detection of fentanyl or its metabolites among the mix of other drugs and metabolites represents realistic conditions. Situations leading to urine fentanyl or fentanyl metabolite concentrations of less than 0.2 ng/mL will result in a false negative finding. False positive results are unlikely because the method requires that the GC retention time index and the MS ion ratios be within restricted limits. False positives can result, however, from sample mix up, unexpected carryover ("ghosting") from a previous high concentration sample, and other erroneous analytical and handling techniques. The presence of norfentanyl on the initial screening (by GC/NP) for one patient highlights the necessity of 621 careful confirmation procedures in urine drug testing. This patient denied use of fentanyl or other analgesics, and GC/MS analysis made clear that the substance was not norfentanyl.She was the same patient for which the saliva norfentanyl samples also were positive. We have no explanation for the differences in this patient's results. Although the GC/NP screen will identify a substance that has similar chromatographic characteristics as, in this example, norfentanyl, the molecular structure was distinctly different than norfentanyl, as resolved by mass spectrometry. Saliva proved difficult to collect according to the patients studied. Four samples contained volumes insufficient to analyze. Norfentanyl was detected in two saliva specimens from one patient at 12 h (0.6 ng/mL) and at 72 h (1.9 ng/mL). Fentanyl and despropionylfentanyl were not detected in any saliva sample. Thus, it would appear that saliva sampling is not a good alternative to urine sampling. Norfentanyl is detectable in the urine for a considerably longer period of time than fentanyl. Drug testing programs either for monitoring recovering addicts or screening health care professionals with access to fentanyl might consider testing for norfentanyl rather than fentanyl. The ability to detect norfentanyl from 48 to 96 h postadministration will enhance the quality and utility of monitoring programs. Further, larger scale studies should be undertaken to better understand the implications of urine testing for fentanyl and its metabolites. Radioimmunoassays under development will require similar confirmation. References 1. Canavan DI. Screening: urine drug tests. Md Med J 1987;36: 229-33. 2. Ikeda R, Pelton C. Diversion programs for impaired physicians. West J Med 1990;152:617-21. 3. McClain DA, Hug CC Jr. Intravenous fentanyl kinetics. Clin Pharmacol Ther 1980;28:106-14. 4. Murphy MR, Hug CC Jr,McClain DA. Dose-independent pharmacokinetics of fentanyl. Anesthesiology 1983;59:53740. 5. Hammargren WR, Henderson GL. Analyzing normetabolites of the fentanyls by gas chromatography/electron capture detection. J Anal Toxicol 1988;12:183-91. 6. Van Rooy HH, Vermeulen MI', Bovill JG.The assay of fentanyl and its metabolites in plasma of patients using gas chromatography with alkali flame ionisation detection and gas chromatography-mass spectrometry. J Chromatogr 1981;223: 85-93. 7. Goromaru T, Matsuura H, Yoshimura N, et al. Identification and quantitative determination of fentanyl metabolites in patients by gas chromatography-mass spectrometry. Anesthesiology 1984;61:73-7. 8. Gillespie TJ,Gandolfi AJ,Maiorino RM, Vaughan RW. Gas chromatographic determination of fentanyl and its analogues in human plasma. J Anal Toxicol 1981;5133-7.