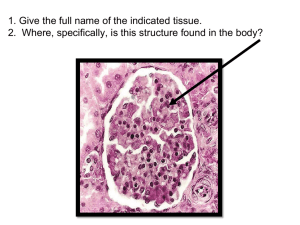
InnovAiT, 8(5), 291–297 DOI: 10.1177/1755738015578935 .......................................................................................................................................................................................................... Bladder problems associated with neurological disease A neurogenic bladder is defined as dysfunction of the bladder secondary to known disease of, or injury to, the central, peripheral or autonomic nervous systems. Neurogenic bladder dysfunction can cause urinary symptoms for the patient as well as increasing the risk of developing recurrent urinary tract infections, bladder calculi and potentially life-threatening complications including sepsis and renal failure. Therefore, it is important for GPs to have a solid understanding of the aetiology, pathophysiology, assessment and management of this condition in order to improve patients’ symptom control and attempt to prevent long-term complications. The GP curriculum and bladder problems associated with neurological disease There is currently no available data on the incidence or prevalence of neurogenic bladder dysfunction in the general population. However, given the prevalence of the causative neurological conditions, the relative risk of each of these for developing neurogenic bladder dysfunction, and the fact that once patients have neurogenic bladder dysfunction they are likely to have it for a long period of time, it is a condition that GPs will encounter on a regular basis in primary care. The symptoms and severity of bladder problems depend upon the location and extent of pathology within the nervous system; however, there is no correlation between the ...................................................... Bladder problems associated with neurological disease are listed as a common and important condition forming part of the knowledge- based Clinical example 3.18: Care of people with neurological problems. GPs should be able to perform the following: . Coordinate care with other primary care health professionals to enable chronic disease management and rehabilitation . Demonstrate empathy and compassion towards patients with disabling neurological conditions . Understand the importance of continuity of care for patients with chronic neurological conditions . Offer health education and accident prevention for people with chronic neurological disorders . Know the functional anatomy of the nervous system relevant to diagnosis . Perform and understand the limitations of a screening neurological examination . Understand the principles of treatment for common conditions that are managed largely in primary care . Make appropriate referrals on behalf of the patient for secondary care investigations and treatment severity of symptoms and risk of long-term complications. It is vital to identify patients suffering from neurogenic lower urinary tract dysfunction early in order to assess their level of risk, with the aim of both managing symptoms and preventing future complications. Nerve supply to the lower urinary tract ........................................................... To understand and manage bladder problems associated with neurological disease it is important to have a good knowledge of the normal innervation of the lower urinary ! The Author(s) 2015. Reprints and permissions: sagepub.co.uk/journalsPermissions.nav Downloaded from ino.sagepub.com at CARLETON UNIV on August 4, 2015 291..................... tract. This allows symptoms to be characterised better and appropriate investigations and treatment initiated. Motor innervation of the bladder Motor innervation to the bladder is supplied by the autonomic nervous system. Parasympathetic nerves supply excitatory input to the smooth muscle of the bladder (detrusor), causing contraction. These parasympathetic nerve fibres originate in spinal segments S2 to S4. They leave the spinal cord through the anterior primary rami and enter the pelvic plexus, where they travel to the bladder and urethra. Sympathetic nerves innervate the smooth muscle of the bladder and exert inhibitory control on muscle contraction. The sympathetic nerve supply to the lower urinary tract varies between males and females. In males, sympathetic nerves innervate the trigone, blood vessels of the bladder, smooth muscle of the prostate and pre-prostatic sphincter. In females there is minimal innervation of the bladder neck or urethra. Sympathetic nerves arise from T10-L2, synapse in the sympathetic chain before travelling to the bladder, urethra and prostate. Afferent innervation of the bladder Afferent neurons, arising from receptors throughout the bladder and urethra, ascend with parasympathetic nerves to the spinal cord, before travelling to the pontine storage centre, micturition centre and cerebral cortex of the brain. They sense bladder-filling. Somatic motor innervation of the urethral sphincter There are two urethral sphincters (Fig. 1): 1. The bladder neck, which is under autonomic (nonvoluntary) control 2. A distal (external) urethral sphincter, which is under voluntary control The distal urethral sphincter is located in the mid-urethra in females and just distal to the apex of the prostate in males. This sphincter consists of three layers, extrinsic skeletal muscle, smooth muscle within the wall and intrinsic striated muscle. The intrinsic striated muscle forms a U-shape around the urethra and is absent posteriorly. It produces urethral occlusion by kinking the urethra, rather than circumferential compression and is supplied by the pudendal nerve (S2-4). The smooth muscle within the wall is tonically active. The extrinsic skeletal muscle forms the outermost layer (the pubo-urethral sling) and is part of the levator ani muscle. Urine storage The bladder is highly compliant. During filling, the pressure within the bladder remains low despite significant 292 ................... ................................................................................................................................................................................................................................................... .............................................................................................................................................................................................................................. Figure 1. Nerve supply to the lower urinary tract. Permission obtained from De Tijdstroom Uitgeverij ß Boon, T. A. Basisboek Urologie (De Tijdstroom, Netherlands, 2001). increases in volume. This is due to the elastic properties of the connective tissues of the bladder and the ability of detrusor smooth muscle cells to increase in length without any change in tension. Micturition Micturition is created by a spino-bulbar-spinal reflex coordinated in the pontine micturition centre of the brainstem. This reflex results in simultaneous detrusor muscle contraction and urethral relaxation, allowing micturition. Receptors within the bladder wall sense increasing tension as the bladder fills. This information is relayed by afferent neurons to the dorsal horn of the sacral cord. Neurons then pass to the peri-aqueductal grey matter of the pons. The peri-aqueductal grey matter and other areas of the brain, such as the orbitofrontal cortex and limbic system, input into the pontine micturition centre and determine whether it is appropriate to start micturition. The system is a positive feedback loop such that contraction is maintained until the bladder is empty. Symptoms ........................................................... Symptoms of neurogenic bladder dysfunction will depend upon the causative neurological pathology and more specifically the site and severity of disease within the nervous system. A summary of the causes of neurogenic bladder are listed in Table 1 and associated symptoms in Table 2. Patients have abnormal bladder or sphincter function and more commonly dysfunction of both. Both the bladder and sphincter may be over- or underactive and any Downloaded from ino.sagepub.com at CARLETON UNIV on August 4, 2015 InnovAiT .......................................................................................................................................................................................................... Table 1. Causes of a neurogenic bladder. Site within nervous system Causes Examples Peripheral nervous system Peripheral neuropathy Diabetes Alcohol abuse Vitamin B12 deficiency Iatrogenic Guillain Barré syndrome Genital herpes Porphyria Syphilis Heavy metal poisoning Iatrogenic Pelvic surgery Regional spinal anaesthesia Space-occupying lesions Brain tumours (24%) Spinal cord tumours Basal ganglia pathology Parkinson’s disease Shy–Drager syndrome Demyelination Multiple sclerosis Vascular Stroke Dementia Alzheimer’s disease Pick’s disease Other Spina bifida Encephalitis Cerebral palsy Cauda equina syndrome Central nervous system Table 2. Symptoms associated with a neurogenic bladder. Type of bladder dysfunction Site of injury/disease Symptoms High pressure (spastic) Central nervous system Spinal cord injury/disease (above T12) Retention Incontinence Nocturia Frequency Urgency Leakage of urine (spasms) Low pressure (hypotonic) Peripheral nervous system Spinal cord injury/damage (S2–S4) Retention Incontinence (overflow) Hesitancy Erectile dysfunction Mixed Central nervous system Peripheral nervous system Combinations of above symptoms Downloaded from ino.sagepub.com at CARLETON UNIV on August 4, 2015 293 .................... combination may co-exist. Symptoms will therefore depend upon the balance between detrusor and sphincter function and activity. Detrusor hyper-reflexia (high pressure) Detrusor hyper-reflexia is bladder over-activity secondary to an underlying neurological problem and is most commonly seen in patients suffering from a disease of the central nervous system or a spinal cord injury above the level of T12. In this group of patients, the bladder intermittently contracts during filling, resulting in an inappropriate high pressure. Symptoms commonly include leakage of urine, urgency, frequency, retention and incontinence. Detrusor areflexia (low pressure) Detrusor areflexia or underactive bladder is seen in patients who have a disease of the peripheral nervous system or a spinal injury at the level of S2–S4. In this group of patients, the bladder is unable to generate high pressures during voiding. Symptoms commonly include retention, incontinence (overflow), hesitancy and erectile dysfunction in men. Detrusor external sphincter dyssynergia Detrusor-external sphincter dyssynergia occurs when involuntary contractions of the external urethral sphincter occur during involuntary contractions of the detrusor muscle and is caused by diseases of the central nervous system. Patients with detrusor over-activity combined with detrusor sphincter dyssynergia are at significant risk of vesicoureteric reflux and subsequent renal damage. ..................................................................................................................................................... .............................................................................................................................................................................................................................. It is therefore vital to identify such patients in order to try and prevent long-term complications. Diagnosis ........................................................... A thorough history and physical examination is vital in diagnosing a neurogenic bladder. It is important to examine both the central and peripheral nervous systems and the bladder itself. In most cases the diagnosis is suspected from the patient’s history and is often reinforced by a large post-void residual volume or palpable bladder. The bladder may be contractile, or there may be an outflow obstruction of the bladder. Both cases will most likely result in urinary retention with overflow incontinence (Rackley, Vasavada, Firoozi, & Ingber 2011). If suspected, initial useful investigations in primary care include urinalysis and routine blood tests, including urea and creatinine levels. Urinary tract infection must be considered and ruled out. An ultrasound of the kidneys, ureters and bladder should be requested to monitor for any hydronephrosis and a request made at the same time for a post-micturition volume to be measured. Urgent referral to urology is recommended in cases of patients with recurrent urinary tract infections, renal failure, obstructed urinary system on imaging, or simply persistent symptoms which fail to resolve despite appropriate initial management (Pannek et al., 2011). For those patients who are not severely debilitated (e.g. are able to go to the bathroom or are able to self-catheterise) further investigations in secondary care are usually endorsed. Table 3 highlights common diagnostic procedures that may then be used to further guide diagnosis and treatment (Rackley et al., 2011). Table 3. Common investigations for suspected neurogenic bladder. 294 ................... Procedure Benefits Cystoscopy Allows discovery of bladder lesions such as inflammation, cancer or bladder stones. May influence treatment decisions according to the cause of incontinence. Cystogram Evaluates the capacity of bladder and detects vesicoureteral reflux. It can help confirm the presence of stress incontinence and the degree of urethral motion. Cystometrogram A filling cystometrogram can determine the bladder volume and pressure. It can also help evaluate detrusor functional capacity and assess the presence of phasic contractions of the bladder (detrusor instability). A voiding cystometrogram can assess the bladder contractility and the extent of a bladder outlet obstruction by simultaneously recording the rate of flow and detrusor pressure. Urodynamics Shows whether there is coordination between bladder contraction and sphincter relaxation. Allows accurate diagnosis of detrusor sphincter dyssynergia, which is common in spinal cord injuries. Uncoordinated voiding occurs due to failure of urethral relaxation during contraction of the bladder. Downloaded from ino.sagepub.com at CARLETON UNIV on August 4, 2015 InnovAiT Management ........................................................... Managing bladder problems associated with neurological disease can be very challenging. The aim of treatment is to protect the upper urinary tract, improve continence, restore function and improve the patient’s quality of life. Adequate support and education is required for both the patient and his or her carers. As always, initial conservative management can often be attempted prior to implementing more definitive medical or surgical treatments. Throughout treatment, it is essential to monitor a patient’s symptoms regularly in addition to 6-monthly renal function and annual ultrasound scan to monitor the upper urinary tracts. Conservative management Conservative measures include controlling daily fluid intake (drinking small amounts throughout the day rather than a large quantity at one time) and managing diet by avoiding spicy food, citrus fruit and caffeinated drinks which can all irritate the bladder. There is good evidence for recommending pelvic floor exercises with the reported successful reduction on incontinence ranging from 56-95% (Rickwood, 2002). Strengthening the levator ani muscles maintains urinary continence by preventing pelvic prolapse. In addition, a voiding diary can be used to record the patient’s daily bladder activity (National Institute for Heath and Care Excellence (NICE), 2012). A pattern is created by recording daily fluid intake and the number of urination attempts. This can help the patient to know when he or she should be near a toilet and when to attempt urination next, gradually gaining better control of bladder function. Absorbent undergarments should be advised to help prevent wetness and odours while protecting the skin and clothes. Bed pads can protect sheets and mattresses for patients who wet the bed. Patients should also be put in contact with support groups and educated about the symptoms of urinary tract infections so that they present early should an infection develop. All patients should have their renal function monitored regularly. Medical management If conservative measures fail to improve symptoms, the next step that can be taken in primary care is the use of medication to control bladder function (NICE, 2012). Certain medications can reduce bladder spasms and tremors, effectively managing the symptoms of the patient. Oxybutynin, tolterodine tartrate and trospium chloride are anticholinergic medications that help relax the smooth muscle of the bladder, preventing spasms. These antispasmodics increase bladder capacity and decrease urge incontinence. In patients with incomplete emptying, clean intermittent self-catheterisation (CISC) ................................................................................................................................................................................................................................................... .......................................................................................................................................................................................................... should be commenced prior to starting anticholinergic medication. Complete bladder emptying avoids residues in the bladder and consequent risk of infection. Antidepressants such as amitriptyline and imipramine also have a similar effect, as they exhibit anticholinergic and direct muscle relaxant effects on the bladder (Pannek et al., 2011). If a trial of these medications in combination with conservative measures fails to improve symptoms, the patient should be referred to secondary care for a urology opinion (Pannek et al., 2011). Following further specialist assessment, alternative medication may be trialled, such as Bethanecol, a parasympathomimetic choline carbamate that selectively stimulates muscarinic receptors. It subsequently increases the contractility of the bladder muscle, improving the ability to urinate. Oestrogen derivatives such as Premarin can be used by post-menopausal women with mild-to-moderate stress incontinence. The up-regulation of alpha-adrenergic receptors increases the tone of urethral muscles, whereas the pelvic muscles are strengthened from the enhanced alpha-adrenergic contractile response (Rackley et al., 2011). The improved urethral mucosal-seal effect prevents the intrinsic sphincter deficiency, which can help alleviate the symptoms of incontinence in patients with neurogenic bladder dysfunction. The human bladder contains 3 beta-adrenoceptors, of which 97% are beta3-adrenoceptors (B3-AR). The stimulation of these receptors inhibits detrusor contractions from the urothelium. A number of clinical trials involving various selective B3-AR agonists have shown promising preliminary results for treating overactive bladders. Catheterisation Once referred to secondary care, catheters will often be advised as an adjunct to conservative and medical treatments (NICE, 2012). In those patients with increased post-residual volumes, CISC is often taught; it also helps reduce the risk of urinary tract infections and improves symptoms. However, patients must have the dexterity to carry out the procedure, which they may need to perform several times a day. If physically or mentally impaired, occasionally a carer or healthcare professional can perform the procedure for the patient; however, these patients will usually require an indwelling catheter (Buckley & Grant, 2009). Indwelling catheters and suprapubic catheters are an option to decompress the bladder in all patients; however, CISC is preferable due to a lower risk of urinary tract infections, urethritis and prostatitis. Patients with long-term urethral catheters will often develop traumatic hypospadias or patulous urethras and therefore patients with neuropathic bladders who require indwelling catheters are usually offered suprapubic catheter placement. Downloaded from ino.sagepub.com at CARLETON UNIV on August 4, 2015 295 .................... It should be noted that a suprapubic catheter does not reduce the risk of urinary tract infection compared with a urethral catheter, however, is often beneficial to patient comfort. In all patients with indwelling catheters, symptoms must be monitored closely. These patients are at increased risk of urinary tract infection compared with those without a catheter or performing CISC and any symptomatic infection must be identified and treated quickly. Indwelling catheters also increase the risk of bladder calculus formation, which may cause patients to present with increased bladder spasm or catheter bypassing. Any suspicion of bladder calculi should result in referral for a urology opinion. Surgical management Surgical treatment is the last resort if conservative and medical measures fail. The choice of the surgical procedure to be performed will depend on patient symptoms and performance status. Overactive neurogenic bladders that are not responsive to medical therapy can be treated with an intravesical injection of botulinum toxin (BotoxÕ ) into the detrusor muscle via a rigid or flexible cystoscope. This blocks postsynaptic muscarinic receptors to prevent involuntary detrusor muscle contractions (Pannek et al., 2014). It is vital to perform a full urodynamic evaluation prior to treatment in order to confirm the diagnosis. If effective, reinjection with botulinum toxin is needed every 9–12 months. There is a 5–10% risk of developing urinary retention in the first 2 months, in which case urinary catheterisation becomes necessary. This can become problematic for patients with neuropathic bladders who are trying to avoid CISC and indwelling catheters. The risk of urinary retention must be discussed with the patient before initiating intravesical botulinum toxin treatment. Other reported side effects of botulinum toxin injection include haematuria, infection and allergic reactions. Other surgical procedures are available; however, they do have a higher risk of complications. In men, external urethral sphincterotomy can be performed to create an open draining channel. This decreases the outlet resistance, which in turn lowers the intravesical pressure removing the need for an indwelling catheter (Utohmo, Groen, & Block, 2014). Artificial sphincters and urethral slings can be beneficial and bladder augmentation (cystoplasty) is occasionally used. This involves increasing the bladder capacity using sections of small or large bowel. Along with the increased volume, the percentage of bladder involved in contraction is also reduced, creating lower internal pressures in the bladder during urination (Ginsberg, 2013). It is also possible to create urinary diversion through either an ileal conduit or ureterostomy, whereas a 296 ................... ................................................................................................................................................................................................................................................... .............................................................................................................................................................................................................................. neurosurgical procedure known as sacral rhizotomy can effectively convert a spastic bladder to a flaccid one by selectively destroying the S3 and S4 nerve roots of the spinal cord. Electrical stimulatory therapy in treating neurogenic bladder is a recent advance. Through a minor surgical procedure, a number of electrodes are placed near targeted nerves and a small stimulator is implanted beneath the skin. Painless electric shocks stimulate the levator ani muscle causing contraction of the external urethral sphincter while inhibiting bladder contraction (Radziszewski, 2013). This act of neuro-modulation can be trialled prior to more invasive procedures such as cystoplasty or reconstructive surgery. Considerations in primary care Patients with neurogenic bladders are commonly seen in primary care. Neurogenic bladder dysfunction causes significant problems to patients with associated urinary symptoms and complications that can reduce the patient’s quality of life. It is vital for GPs to be able to identify patients suffering from neurogenic lower urinary tract dysfunction early in order to assess their level of risk with the aim of both managing symptoms and preventing future complications. Simple investigations and treatment options can be undertaken in primary care with appropriate referrals to secondary care made when symptoms fail to improve or complications develop. Key points . Patients with neurogenic bladder are often seen in primary care . Thorough history and examination are essential to diagnosis . Conservative measures and anticholinergic medication, if appropriate, should be started in primary care . At each review, assess for complications including urinary tract infection, sepsis and renal failure . If symptoms fail to improve or complications develop, consider referral to secondary care References and further information . Bors, E., & Turner, R. D. (1960). History and physical examination in neurological urology. Journal of Urology, 83, 759–767. Retrieved from www.ncbi. nlm.nih.gov/pubmed/13802958 . Buckley, B., & Grant, A. M. (2009). What is the most effective management of neurogenic bladder dysfunction? British Medical Journal, 338, 659. doi: 10.1136/bmj.b659 . Ginsberg, D. (2013). Optimizing therapy and management of neurogenic bladder. American Journal of Managed Care, 19(10), S197–S204. Retrieved Downloaded from ino.sagepub.com at CARLETON UNIV on August 4, 2015 InnovAiT . . . . . from www.ajmc.com/publications/supplement/ 2013/ace012_jul13_ngb/ace012_jul13_ngb_ginsberg2_s197/1 Igawa, Y., Aizawa, N., & Homma, Y. (2010). Beta3adrenoceptor agonists: Possible role in the treatment of overactive bladder. Korean Journal of Urology, 51(12), 811–818. Retrieved from www.ncbi.nlm.nih.gov/pmc/articles/PMC3016425 Madersbacher, H. (1990). The various types of neurogenic bladder dysfunction: An update of current therapeutic concepts. Paraplegia, 28(4), 217–229. doi: 10.1038/sc.1990.28 NICE. (2012). Urinary incontinence in neurological disease. Retrieved from www.nice.org.uk/guidance/CG148 Pannek, J., Blok, B., Castro-Diaz, D., del Popolo, G., Groen, J., Karsenty, G.,. . .Stohrer, M. (2014). European Association of Urology. Guidelines on neuro-urology. Retrieved from www.uroweb.org/ gls/pdf/21%20Neuro-Urology_LR.pdf Pannek, J., Stohrer, M., Blok, B., Castro-Diaz, D., del Popolo, G., Kramer, G.,. . .Wyndaele, J. J. (2011). European Association of Urology. Guidelines on neurogenic lower urinary tract dysfunction. Retrieved from www.uroweb.org/gls/ pdf/20_Neurogenic%20LUTD_LR.pdf .......................................................................................................... .......................................................................................................................................................................................................... . Rackley, R., Vasavada, S. P., Firoozi, F., & Ingber, M. S. (2011). Neurogenic bladder. Retrieved from www.emedicine.medscape.com/article/453539 . Radziszewski, K. (2013). Outcomes of electrical stimulation of the neurogenic bladder: Results of a two-year follow-up study. NeuroRehabilitation, 32(4), 867–873. Retrieved from www.ncbi.nlm. nih.gov/pubmed/23867413 . RCGP. Clinical example 3.18: Care of people with neurological problems. Retrieved from www.rcgpcurriculum.org.uk/pdf/curr_3_18_Neurological _problems.pdf . Rickwood, A. M. (2002). Assessment and conservative management of the neuropathic bladder. Seminars in Pediatric Surgery, 11(2), 108–119. Retrieved from www.ncbi.nlm.nih.gov/pubmed/ 11973763 . Utomo, E., Groen, J., & Blok, B. (2014). Surgical management of functional bladder outlet obstruction in adults with neurogenic bladder dysfunction. Cochrane Database of Systematic Reviews, 5. art. no.: CD004927. doi: 10.1002/14651858.CD004927.pub4 Mr Thomas J Smith, Dr Victoria Andrews, Dr Seok Cho, Mr Nicholas Drinnan and Mr William Dunsmuir St Peter’s Hospital, Ashford and St Peters NHS Trust Email: thomas.smith@doctors.org.uk DOI: 10.1177/1755738015580701 ............................................................................................................................................................ Single best answer question You are seeing an 18-month-old boy at midnight while doing an out-of-hours shift. The parents tell you that he had a fever and barking cough all day. About 2 hours ago he started to develop noisy breathing that is keeping him awake. The child’s parents have tried paracetamol and steaming with little effect. You feel that the most likely diagnosis is croup and you find no signs of respiratory distress on examination. ...................................................... AKT question relating to wheezy children The most appropriate course of action is: A. To explain the diagnosis to parents, reassure them and discharge him home B. To give the child a dose of oral prednisolone and discharge him home with advice to see his own GP in the morning C. To give the child a dose of oral dexamethasone and discharge him home with advice to see his own GP in the morning D. To refer him to the on-call paediatrician E. To send him as an emergency to hospital with a blue light ambulance Answer DOI: 10.1177/1755738015580702 Dr Yasser Abdel Kerim GP Partner, Banks and Bearwood Medical Centre, Bournemouth Downloaded from ino.sagepub.com at CARLETON UNIV on August 4, 2015 297 ....................