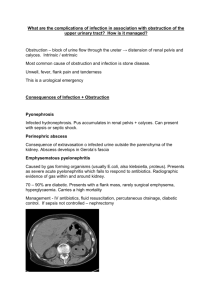
Gastroenterol Clin N Am 35 (2006) 101–112 GASTROENTEROLOGY CLINICS OF NORTH AMERICA Palliation of Malignant Obstructive Jaundice Todd H. Baron, MD Division of Gastroenterology & Hepatology, Mayo Clinic College of Medicine, 200 First Street Southwest, Charlton 8A, Rochester, MN 55905, USA M alignant obstructive jaundice in the patient with incurable malignancy may cause symptoms that reduce quality of life. Palliation of malignant obstructive jaundice leads to improvement in quality of life. Nonsurgical methods using percutaneous and endoscopic methods have supplanted surgical bypass as the primary method for the palliation of malignant obstructive jaundice. This article reviews management strategies for palliation of malignant obstructive jaundice. CAUSES OF MALIGNANT OBSTRUCTIVE JAUNDICE Malignant obstructive jaundice may be caused by various malignancies, most commonly pancreatic carcinoma. Ampullary cancer, primary bile duct cancer (cholangiocarcinoma), and metastatic lesions to the head of the pancreas or porta hepatis also may cause biliary obstruction (Box 1). The location of the obstruction within the biliary tree is important with regards to the palliative approach within each discipline, and it generally is divided into nonhilar and hilar biliary obstruction (see Box 1). In general, it is more difficult both technically and clinically to successfully relieve jaundice from hilar biliary obstruction regardless of the method used to alleviate obstruction. Nonetheless, even patients with metastatic disease as the cause of hilar biliary obstruction usually can be palliated effectively using a nonsurgical approach [1]. SYMPTOMS AND QUALITY OF LIFE Obstructive jaundice can produce various symptoms. Anorexia, usually attributed to cytokines, may be caused by biliary obstruction. Weight loss, another symptom attributed to the tumor itself, may be caused by malabsorption of fat, even in the absence of overt steatorrhea [2]. Additionally, because of the lack of secretion of bile salts into the small intestine, vitamin K malabsorption occurs. This is important for two reasons. First, in patients who are undergoing invasive procedures during the evaluation and treatment of obstructive jaundice, E-mail address: baron.todd@mayo.edu 0889-8553/06/$ – see front matter doi:10.1016/j.gtc.2006.01.001 ª 2006 Elsevier Inc. All rights reserved. gastro.theclinics.com 102 BARON Box 1: Common causes of malignant obstructive jaundice Nonhilar biliary obstruction Pancreatic cancer Metastatic disease to the head of pancreas (renal cell carcinoma, breast cancer) Ampullary cancer Nodal compression Gallbladder cancer Extrinsic masses Hilar obstruction Cholangiocarcinoma Metastatic disease Central intrahepatic masses, primary or secondary Gallbladder cancer the coagulopathy should be reversed to minimize and prevent bleeding complications. Second, in patients who are already on warfarin sodium, excessive anticoagulation may occur and result in severe bleeding complications. Pruritus usually occurs with higher levels of serum bilirubin and may be intractable and disabling. Finally, social embarrassment may occur as a result of the overt physical presence of jaundice. Cholangitis rarely occurs in patients with malignant obstructive jaundice, unless there has been previous instrumentation of the biliary tree. Relief of obstructive jaundice has been shown to improve quality if life [3,4]. METHODS OF PALLIATION There are three methods for palliation of obstructive jaundice: surgical bypass, percutaneous insertion of stents, and endoscopic insertion of stents. Each of these approaches has advantages and disadvantages (Table 1). There are very few comparative studies of outcomes for each of the disciplines, although nonsurgical palliation of obstructive jaundice is preferred in those with poor performance status, intra-abdominal ascites, and/or expected survival of less than 4 to 6 months. Surgical Palliation Surgical palliation of malignant obstructive jaundice is achieved by bypassing the obstructed system through the creation of a choledocho– or hepatico–enterostomy, usually a jejunostomy [5]. Traditionally, biliary bypass was performed using open techniques, but more recently, it has performed laparoscopically [6]. MALIGNANT OBSTRUCTIVE JAUNDICE 103 Table 1 Approaches to palliation of obstructive jaundice Surgical Percutaneous Endoscopic Advantages Disadvantages Life-long palliation usual Simultaneous palliation of gastric outlet obstruction Simultaneous palliation of pain (intraoperative nerve block) Nonsurgical Most invasive Morbidity and mortality Nonsurgical Relatively painless Outpatient treatment possible Pain, bleeding External drains Stents may occlude Expertise variable Complications (perforation, pancreatitis, bleeding) Most of the data for surgical bypass are derived from the treatment of distal biliary obstruction caused by pancreatic cancer. Palliative surgical bypass may be performed at the time of laparotomy for attempted curative resection. If the patient is found to be unresectable, a surgical palliative approach may be undertaken. Alternatively, patients deemed inoperable based upon extent of disease, comorbid medical illnesses, or advanced age are referred for nonsurgical palliation. Since the evolution of better preoperative staging modalities (endoscopic ultrasound, thin section CT, and MRI) and the improvement in nonoperative palliative strategies, it appears that fewer patients are undergoing operative palliation. Nonetheless, surgical palliation has the advantage of allowing simultaneous palliation of biliary and gastric outlet obstruction and pain control in one setting [5]. Lifelong palliation of biliary obstruction without the need for further procedures usually is obtained. The average postoperative length of hospital stay for patients who undergo surgical palliation is less than 15 days. The average survival of patients who receive surgical palliation alone for nonmetastatic, unresectable pancreatic cancer is approximately 8 months [5]. The disadvantage of surgical palliation is the morbidity, especially in those with advanced disease. Surgical palliation of distal biliary obstruction Surgical palliation is performed using a biliary–enteric bypass, most commonly the bile duct to the jejunum (choledocho–jejunostomy). The use of the gallbladder as a conduit (cholecysto–jejunostomy) is utilized rarely, because premature occlusion of the cystic duct by tumor growth leads to subsequent loss of palliation and need for additional palliative procedures [7]. Successful palliation of jaundice is achieved in nearly all patients. Complications include wound infection, pneumonia, and bleeding. Surgical palliation of hilar biliary obstruction Surgical palliation is performed infrequently for palliation of hilar biliary obstruction. The bypass is created by sewing intrahepatic ducts to the jejunum 104 BARON (hepatico–jejunostomy) [8,9]. The success rate for relief of jaundice is lower; the complication rate is higher, and the recurrence of jaundice is more likely with hilar obstruction than with distal biliary obstruction [5,10]. Biliary enteric anastomosis specifically for hilar cholangiocarcinoma carries a morbidity and mortality as high as 50% and 12%, respectively [10]. One serious complication is the development of an anastomotic bile leak. Nonsurgical Palliation Nonsurgical palliation of malignant obstructive jaundice is achieved with stent placement by means of the percutaneous, endoscopic, or rarely combined percutaneous–endoscopic approaches. For nonsurgical techniques, biliary stents used are composed of plastic (Fig. 1) or metal materials. Plastic stents occlude, because the formation of bacterial biofilm and plant materials [11] results in recurrent jaundice, frequently with cholangitis, and necessitates repeat procedures with stent replacement. Self-expandable metal stents (SEMS) have combined the advantage of a small predeployment delivery system with a large postdeployment stent diameter (Fig. 2). Additionally, they are less likely to occlude than plastic stents. Metal stents still may occlude because of tumor ingrowth through the mesh, tumor overgrowth (tumor growing beyond the ends of the stent), or tissue hyperplasia (excessive normal tissue growth in response to the stent). SEMS may be uncovered or covered. Covered SEMS resist occlusion from tumor ingrowth or tissue hyperplasia, although they are Fig. 1. Examples of 10Fr plastic biliary stents. MALIGNANT OBSTRUCTIVE JAUNDICE 105 Fig. 2. Examples of deployed self-expanding metal biliary stents. Note the third stent from the left is covered. more likely to migrate. They cannot be used across the bifurcation, because the covering prevents drainage of intrahepatic bile ducts. Percutaneous Palliation Percutaneous therapy is performed by interventional radiologists by means of a transhepatic approach (percutaneous transhepatic cholangiography, PTC). The intrahepatic bile ducts initially are accessed with a skinny needle under fluoroscopic guidance and an anterograde approach. Three possible outcomes may occur following attempted percutaneous drainage. The least desirable is termed external drainage. This occurs when the bile ducts are entered, but there is a failure to traverse the stricture to place catheters and guide wires into the duodenum. Thus, the only route for bile drainage is externally, through the percutaneous tube (Fig. 3). The second possible scenario is called internal–external drainage. This occurs when the stricture is traversed, and a catheter is passed into the duodenum; the external portion exits the skin (Fig. 4). Bile can drain internally and externally, and eventually the external tube can be capped or completely internalized. Usually, the most desirable outcome is internal drainage, whereby the entire drainage is within the patient by means of an internal stent. Some patients may have internalization on the first attempt, or rarely, stages of advancement may occur from external to internal. For example, one procedure may be required for initial external tube placement and another for internalization to a stent. Uncommonly, internalization is not technically possible, and the patient is left with an external drain. Prior to the advent of SEMS, the percutaneous tract through the liver required dilation to accommodate large-bore plastic stents. This was associated with a higher incidence of postprocedural pain and bleeding. Because SEMS have a small predeployment delivery system, the tract through the liver requires less dilation. The main disadvantage of percutaneous therapy is the pain felt as a result of the catheter placement procedure through body wall and the liver 106 BARON Fig. 3. Radiograph of external biliary drain (arrowheads). The stricture below the catheter was not traversable at the time of percutaneous transhepatic cholangiography. capsule, and the subsequent unpleasantness of having one’s biliary secretions visible as a reminder of their illness. Percutaneous palliation of distal biliary obstruction Percutaneous insertion of plastic or metal stents is achievable in nearly all patients with distal bile duct obstruction. With the advent of endoscopic Fig. 4. Radiograph of patient with internal–external biliary drain. Note the external portion (arrowheads) leads to the skin. Bile flows through the drain into the duodenum, where the distal end is coiled (arrow). MALIGNANT OBSTRUCTIVE JAUNDICE 107 palliation, percutaneous therapy has become less commonly performed and is used when endoscopic techniques fail or when the papilla is inaccessible because of duodenal invasion by tumor or because of postsurgical anatomy. There is only one randomized, prospective trial comparing percutaneous and endoscopic therapy for the palliation of distal malignant obstructive jaundice. This landmark study showed that the endoscopic method had a significantly higher success rate for relief of jaundice (81% versus 61%) and significantly lower 30-day mortality (15% versus 33%). The higher mortality in the percutaneous group was caused by complications associated with liver puncture (bleeding and bile leaks) [12]. This study is dated, because it was performed using plastic stents prior to the development of expandable metal stents, the insertion of which is less likely to require aggressive dilation of the percutaneous tract through the liver, which in turn decreases bleeding and bile leakage [13,14]. Nonetheless, more recent studies have shown that major complications following percutaneous SEMS placement are still more common than major complications following endoscopic stent placement [15]. Percutaneous stent placement, however, is effective in most patients who have failed attempts at endoscopic stent placement [16]. Additionally, in centers without expertise in endoscopic retrograde cholangiopancreatography (ERCP), percutaneous therapy is used as the primary method of nonsurgical palliation of malignant obstructive jaundice. Overall, the technical success rate of percutaneous expandable metal stent placement is high, with a high rate of clinical resolution of jaundice [17]. In addition to primary tumors of the biliary tree, metastatic disease to the biliary system may occur. Successful palliation is also achievable in this group using the percutaneous approach [18]. Percutaneous palliation of hilar biliary obstruction Palliation of hilar obstruction is more difficult because of the inability to place one stent to drain the entire liver. Indeed, the early reports of percutaneous drainage showed that only 50% of patients achieved either fair or good palliation [19]. More recently, the use of expandable stents has produced better results, although when compared with nonhilar tumors, the outcome is inferior. For example, one study comparing the outcome of 58 patients who underwent percutaneous intervention for palliation of hilar and nonhilar tumors showed that relief of jaundice was significantly less in hilar tumors and that the long-term patency of expandable stents was significantly lower in the presence of hilar involvement [20]. It appears from the literature that only one side of the liver (ie, one stent or tube) is required to palliate jaundice in most patients [9,10,21]. Endoscopic Endoscopic palliation of distal biliary obstruction ERCP and biliary stent placement (Fig. 5) has been shown in randomized trials to be an acceptable alternative to palliative surgical bypass [22]. Biliary stents 108 BARON Fig. 5. Illustration of endoscopic placement of plastic biliary stent for relief of jaundice from malignant biliary obstruction. (Courtesy of Wilson-Cook Medical, Winston-Salem, NC; with permission.) can be placed safely in an outpatient setting [23]. The comparative studies of endoscopy and surgery for palliation of distal biliary obstruction were performed using plastic stents prior to the advent SEMS. As previously mentioned, the main limitation to plastic stent placement is stent occlusion as a result of bacterial biofilm. Thus, in the comparative trials of surgery and endoscopy, the lower initial hospital stay in the endoscopy group was offset by the need for subsequent hospitalization and need for subsequent ERCP to manage stent occlusion. The median time for stent occlusion for standard large-bore stents is approximately 3 months. Stent occlusion results in recurrent jaundice, usually with cholangitis. Expandable metal stents have overcome the problem of bacterial biofilm, and randomized controlled trials have shown superior patency rates to plastic stents [24]. Because the cost of expandable metal stents is much greater than that of plastic stents, they are cost-effective only if the patient lives greater than 3 to 6 months. Therefore, projected life expectancy should be considered when choosing between plastic and metal stents [25]. Other factors to be considered include patient compliance, ability to return for care, and early stent occlusion of plastic stents. Metal stent occlusion generally is managed easily with placement of a plastic stent or another metal stent within the existing metal stent (Fig. 6) [26]. More recently, covered metal stents have been developed to overcome occlusion caused by tumor overgrowth and tissue hyperplasia. Early comparative studies have shown prolonged patency with covered metal stents compared with uncovered stents [27]. MALIGNANT OBSTRUCTIVE JAUNDICE 109 Fig. 6. (A) Endoscopic photo of occluded metal stent caused by tissue hyperplasia and/or tumor. (B) Same patient. Plastic stent (blue) has been inserted through the metal stent. Endoscopic palliation of hilar biliary obstruction Hilar strictures may be caused by cholangiocarcinoma or metastatic diseases. The clinical success rates for achieving adequate palliation for hilar tumors is less than that for distal tumors [28]. Furthermore, technical success rates for bilateral endoscopic stent placement (right and left hepatic ducts) are also lower. Most patients with hilar obstruction will be palliated adequately when only one side of the liver (unilateral drainage) is drained, assuming only one side has been accessed [9]. Patients who have had contrast instilled in both systems require stenting of both systems to prevent progressive cholangitis [29]. It is not as firmly established that metal stents offer superior prolongation of palliation compared with plastic stents, as is seen in distal strictures. In a prospective, single-arm pilot study of metal stent placement in 17 patients with Bismuth type II and III obstruction, however, median stent patency was 12 months [30]. A more recent noncomparative, single-arm study showed that Wallstent insertion is safe and feasible, and achieves successful palliation without the need for further biliary reintervention in most (69%) patients with nonresectable hilar cholangiocarcinoma [31]. This suggests that metal stents may offer the same benefits in hilar biliary obstruction as in distal biliary obstruction. Recently, photodynamic therapy (PDT) has been used for palliation of patients with unresectable hilar cholangiocarcinoma who did not resolve their jaundice after adequate endoscopic stent placement [32]. Significant improvement in cholestasis, quality of life, and survival (as compared with historical controls) has been demonstrated in one study [33]. In another study, improvement in cholestasis, performance, and quality of life was seen and maintained for an extended period [34]. These studies were performed outside of the United States, where smaller, more flexible laser fibers are available. Currently, passage of laser fibers available for the treatment of esophageal cancer into the biliary system is difficult, but feasible. 110 BARON Overall, in patients with unresectable cholangiocarcinoma who are undergoing ERCP for palliation, unilateral stenting should be performed with contrast injection confined to one lobe. A pre-ERCP abdominal CT may reveal atrophy of one lobe, and this lobe specifically is avoided, because contamination will require drainage to prevent cholangitis but likely will not add to palliation. Alternatively, MRI can define the anatomy prior to ERCP. One stent, plastic or metal is usually adequate to achieve palliation [35]. PDT for cholangiocarcinoma should be performed in select centers until randomized trials (currently underway in Europe) clearly demonstrate superiority of PDT over stents alone. Brachytherapy is yet another approach to palliation of hilar cholangiocarcinoma, although it is used infrequently and in very few centers. Brachytherapy is performed by placing Iridium92 catheters into the biliary tree so as to deliver high-dose intraductal radiation therapy. Combined Percutaneous and Endoscopic Approach to Biliary Obstruction In some situations in which endoscopic therapy fails to access the bile and/or traverse the stricture, a percutaneous approach is performed to facilitate the endoscopic procedure [10]. The advantage of this approach versus the completion of the entire procedure percutaneously may be realized in selected situations [36]. SUMMARY Palliation of obstructive jaundice can be achieved in most patients using various approaches. The method chosen should be individualized to the patient and based upon performance status, patient preferences, and available expertise. The best approach ideally should be determined by a multi-discipline approach with endoscopists, interventional radiologists, oncologists, and surgeons. References [1] Van Laethem JL, De Broux S, Eisendrath P, et al. Clinical impact of biliary drainage and jaundice resolution in patients with obstructive metastases at the hilum. Am J Gastroenterol 2003;98(6):1271–7. [2] Wakasugi H, Hara Y, Abe M. A study of malabsorption in pancreatic cancer. J Gastroenterol 1996;31(1):81–5. [3] Ballinger AB, McHugh M, Catnach SM, et al. Symptom relief and quality of life after stenting for malignant bile duct obstruction. Gut 1994;35:467–70. [4] Abraham NS, Barkun JS, Barkun AN. Palliation of malignant biliary obstruction: a prospective trial examining impact on quality of life. Gastrointest Endosc 2002;56(6):835–41. [5] House MG, Choti MA. Palliative therapy for pancreatic/biliary cancer. Surg Clin North Am 2005;85(2):359–71. [6] Date RS, Siriwardena AK. Laparoscopic biliary bypass and current management algorithms for the palliation of malignant obstructive jaundice. Ann Surg Oncol 2004;11(9):815–7. [7] Urbach DR, Bell CM, Swanstrom LL, et al. Cohort study of surgical bypass to the gallbladder or bile duct for the palliation of jaundice due to pancreatic cancer. Ann Surg 2003;237(1): 86–93. MALIGNANT OBSTRUCTIVE JAUNDICE 111 [8] Jarnagin WR, Burke E, Powers C, et al. Intrahepatic biliary enteric bypass provides effective palliation in selected patients with malignant obstruction at the hepatic duct confluence. Am J Surg 1998;175(6):453–60. [9] Freeman ML, Sielaff TD. A modern approach to malignant hilar biliary obstruction. Rev Gastroenterol Disord 2003;3(4):187–201. [10] Singhal D, van Gulik TM, Gouma DJ. Palliative management of hilar cholangiocarcinoma. Surg Oncol 2005;14(2):59–74. [11] van Berkel AM, van Marle J, Groen AK, et al. Mechanisms of biliary stent clogging: confocal laser scanning and scanning electron microscopy. Endoscopy 2005;37(8):729–34. [12] Speer AG, Cotton PB, Russell RC, et al. Randomised trial of endoscopic versus percutaneous stent insertion in malignant obstructive jaundice. Lancet 1987;2(8550):57–62. [13] Inal M, Aksungur E, Akgul E, et al. Percutaneous placement of metallic stents in malignant biliary obstruction: one-stage or two-stage procedure? Predilate or not? Cardiovasc Intervent Radiol 2003;26(1):40–5. [14] Beissert M, Wittenberg G, Sandstede J, et al. Metallic stents and plastic endoprostheses in percutaneous treatment of biliary obstruction. Z Gastroenterol 2002;40(7):503–10. [15] Pinol V, Castells A, Bordas JM, et al. Percutaneous self-expanding metal stents versus endoscopic polyethylene endoprostheses for treating malignant biliary obstruction: randomized clinical trial. Radiology 2002;225(1):27–34. [16] Doctor N, Dick R, Rai R, et al. Results of percutaneous plastic stents for malignant distal biliary obstruction following failed endoscopic stent insertion and comparison with current literature on expandable metallic stents. Eur J Gastroenterol Hepatol 1999;11(7):775–80. [17] Kaskarelis IS, Papadaki MG, Papageorgiou GN, et al. Long-term follow-up in patients with malignant biliary obstruction after percutaneous placement of uncovered wall stent endoprostheses. Acta Radiol 1999;40(5):528–33. [18] Kaskarelis IS, Minardos IA, Abatzis PP, et al. Percutaneous metallic self-expandable endoprostheses in biliary obstruction caused by metastatic cancer. Hepatogastroenterology 1996;43(10):785–91. [19] Gibson RN, Yeung E, Hadjis N, et al. Percutaneous transhepatic endoprostheses for hilar cholangiocarcinoma. Am J Surg 1988;156(5):363–7. [20] Becker CD, Glattli A, Maibach R, et al. Percutaneous palliation of malignant obstructive jaundice with the wall stent endoprosthesis: follow-up and reintervention in patients with hilar and non-hilar obstruction. J Vasc Interv Radiol 1993;4(5):597–604. [21] Inal M, Akgul E, Aksungur E, et al. Percutaneous placement of biliary metallic stents in patients with malignant hilar obstruction: unilobar versus bilobar drainage. J Vasc Interv Radiol 2003;14(11):1409–16. [22] Taylor MC, McLeod RS, Langer B. Biliary stenting versus bypass surgery for the palliation of malignant distal bile duct obstruction: a meta-analysis. Liver Transpl 2000;6(3):302–8. [23] Cvetkovski B, Gerdes H, Kurtz RC. Outpatient therapeutic ERCP with endobiliary stent placement for malignant common bile duct obstruction. Gastrointest Endosc 1999;50(1):63–6. [24] Levy MJ, Baron TH, Gostout CJ, et al. Palliation of malignant extrahepatic biliary obstruction with plastic versus expandable metal stents: an evidence-based approach. Clin Gastroenterol Hepatol 2004;2(4):273–85. [25] Arguedas MR, Heudebert GH, Stinnett AA, et al. Biliary stents in malignant obstructive jaundice due to pancreatic carcinoma: a cost-effectiveness analysis. Am J Gastroenterol 2002;97(4):898–904. [26] Bueno JT, Gerdes H, Kurtz RC. Endoscopic management of occluded biliary wall stents: a cancer center experience. Gastrointest Endosc 2003;58(6):879–84. [27] Isayama H, Komatsu Y, Tsujino T, et al. A prospective randomised study of covered versus uncovered diamond stents for the management of distal malignant biliary obstruction. Gut 2004;53(5):729–34. [28] Liu CL, Lo CM, Lai EC, et al. Endoscopic retrograde cholangiopancreatography and endoscopic endoprosthesis insertion in patients with Klatskin tumors. Arch Surg 1998;133:293–6. 112 BARON [29] Chang WH, Kortan P, Haber GB. Outcome in patients with bifurcation tumors who undergo unilateral versus bilateral hepatic duct drainage. Gastrointest Endosc 1998;47:354–62. [30] Peters RA, Williams SG, Lombard M, et al. The management of high-grade hilar strictures by endoscopic insertion of self-expanding metal endoprostheses. Endoscopy 1997;29:10–6. [31] Cheng JLS, Bruno MJ, Bergman JJ, et al. Endoscopic palliation of patients with biliary obstruction caused by nonresectable hilar cholangiocarcinoma: efficacy of self-expandable metallic wall stents. Gastrointest Endosc 2002;56:33–9. [32] Ortner MA, Liebetruth J, Schreiber S, et al. Photodynamic therapy of nonresectable cholangiocarcinoma. Gastroenterology 1998;114:536–42. [33] Ortner M. Photodynamic therapy for cholangiocarcinoma. J Hepatobiliary Pancreat Surg 2001;8:137–9. [34] Wiedmann M, Berr F, Schiefke I, et al. Photodynamic therapy in patients with nonresectable hilar cholangiocarcinoma: 5-year follow-up of a prospective phase II study. Gastrointest Endosc 2004;60(1):68–75. [35] Costamagna G, Tringali A, Petruzziello L, et al. Hilar tumours. Can J Gastroenterol 2004;18(7):451–4. [36] Wayman J, Mansfield JC, Matthewson K, et al. Combined percutaneous and endoscopic procedures for bile duct obstruction: simultaneous and delayed techniques compared. Hepatogastroenterology 2003;50(52):915–8.