Respiratory Care Guide: FiO2, Ventilation, Chest Trauma & More
advertisement

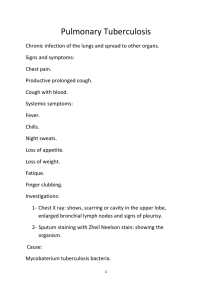
FiO2 Range 21-50% Intervention Titrate the FIO2 to 50% or less as prolonged FIO2 of 50% or greater can lead to oxygen toxicity and atelectasis. FIO2 must be slowly decreased Ventilation Intervention Weaning Administer high – flow oxygen at 100%. Auscultate breath sounds frequently Monitor continuous pulse oximetry Hypoventilation Hyperventilation Blowing off excessive paco2 from hyperventilation results in blowing off excess acid, causing respiratory alkalosis. Bronchoscopy Description Direct visual examination of the larynx, trachea, and bronchi with a fiberoptic bronchoscope. The client receives mild sedation (eg, midazolam) to provide relaxation and promote comfort. A topical anesthetic (eg, lidocaine, benzocaine) is applied to the nares and throat to suppress the hag and cough reflexes, prevent laryngospasm, and facilitate passage of the scope. Pre intervention Maintain NPO. Assess coagulation studies. Remove dentures and eyeglasses. Establish an IV access and administer medication for sedation. Have emergency resuscitation supplies readily available. Post intervention Maintain a semi- fowler’s position. Assess for the return of the gag reflex. Maintain NPO status until the gag reflex returns. Monitor for bloody sputum. Bright red colored sputum indicates hemorrhage. (Blood – tinged sputum is common and not an emergency.) Monitor respiratory status. Monitor for complications, such as bronchospasm or bronchial perforation, indicated by facial or neck crepitus, dysrhythmias, hemorrhage, hypoxemia, and pneumothorax. Expected finding Cough After procedure Dark red sputum which indicated old blood Drowsiness due to the sedative effects of medication given prior to and during the procedure Unexpected finding After procedure Bronchospasm. This can manifest as reports of chest tightness, auscultated wheezing, decreased oxygenation with continual coughing, or audible stridor. Rib fracture Flail chest Pulmonary contusion Pneumothorax 1.Pain, tenderness 1.Paradoxial respirations, Hemoptysis, 1. X ,↓breath sounds affected Description Assessment dyspnea, tachypnea, shallow ↓ breath sounds, 2.↓chest expansion unilaterally 2.Shallow respirations ↑w/ inspiration respiration, ↓breath sounds crackles, wheezes, 3. subcutaneous emphysema 3.Splint chest 2.Severe chest pain ↑bronchial secretion, 4. sucking sound open chest 3.Cyanosis dyspnea, restlessness 5. tracheal deviation affected w/ 4.Tachycardia, hypotension tension pneumothorax 6. tachycardia, hypotension 7. dyspnea, tachypnea 8. cyanosis 9. sharp chest pain Intervention 갈비뼈 자연 붙음 x-ray 진단 파울러자세, 파울러자세, 산소, 기침/심호흡, 파울러자세, 산소, 침상안정, 파울러자세, 통증약물, intercoastal never block 가 통증약물, 침상안정, PEEP 가능 PEEP 가능 nonporous dressing- open chest 능, 가슴지지교육 wound, 산소, chest tube u/ lung expand full Chest tube Description Chest tubes are indicated to drain air or fluid from the pleural space and reestablish negative pressure, which allows for proper lung expansion. Intervention Excessive drainage >100ml, notify When chest tube Auscultate breath sounds to assess the lung has re-expanded and there is no more drainage. Stops abruptly, Have client cough and deep breath. Reposition the client. (Do not milk the chest tube. Milking chest tubes to maintain patency is performed only if prescribed.) When the chest tube Immediately apply a sterile occlusive dressing (eg, petroleum jelly dressing) taped on 3 sides. This action permits air to escape on exhalation and inhibits air is dislodged from the intake on inspiration. client, and air leak sound is heard, If the chest tube Without contamination, wipe the end of the chest tube with an antiseptic and immediately reconnect it. disconnects from the With contamination, and cannot be immediately reattached, or if the chest drainage unit breaks, cracks, or malfunctions, submerge the distal end of the chest drainage tubing, tube 1-2 in (2-4cm) below the surface of a 250 mL bottle of sterile water or saline. Removal of the chest Administer analgesic 30-60 min prior to the procedure. tube Prepare suture removal kit, petroleum gauze, and occlusive dressing Instruct the client to take a deep breath, hold it , and bear down (Valsalva maneuver) while the tube is being removed. Perform a post-procedure chest X-ray to ensure there is no re accumulation of air or fluid in the pleural space Tracheostomy Description Post intervention The immediate postoperative priority goal for a client with a new tracheostomy is to prevent accidental dislodgement of the tube and loss of the airway. If dislodgement occurs during the first postoperative weekm reinsertion of the tube is difficult as it takes the tract about 1 week to heal. For this reason, dislodgement is a medical emergency. The priority nursing intervention is to ensure the tube is place securely by checking the tightness of ties and allowing for 1 finger to fit under these ties. Accidental Medical emergency dislodgement If the airway tract is well formed, attempt to open the airway by inserting a curved hemostat to maintain stoma patency and insert a new tracheostomy tube with an obturator. Position that facilitate breathing High fowler’s position How to Orthopneic position Tripod position Sitting in a chair, on the side, or in bed leaning Sitting in a chair leaning forward with hands or over the bedside table, with one or more pillows elbows resting on the knees. under the arms or elbows for support Indication Position Condition High fowler Affected side-lying pneumonectomy Trandelenburg Pursed lip breathing How to Inhale for 2 seconds through the nose with the mouth closed Exhale for 4 seconds through pursed lips. If unable to exhale for this long, exhale twice as long as inhaling Description Acute respiratory failure Acute respiratory distress syndrome (ARDS) ◀↓oxygen is transported to the blood/ A form of acute respiratory failure that occurs as a complication ↓CO2 is removed from the lungs Caused by a diffuse lung injury, critical illness, increased capillary permeability. ▶ compensatory mechanisms fail It results in extravascular lung fluid, pulmonary edema, decreased surfactant production, and acidosis Assessment Intervention 1. Dyspnea, ↑↓ respirations and breath sounds 1. Dyspnea, tachypnea, ↓breath sounds 2. Tachycardia, hypertension, dysrhythmia 2. Pulmonary infiltrates, pulmonary edema, pulmonary hypertension 3. Confusion, ↓consciousness 3. Deteriorating ABG, hypoxemia w/ high oxygen 파울러자세, 파울러자세, 산소(PaO2>60-70mmHg 유지 안될 시 인공호흡기), 산소, 인공호흡기(PEEP), 기관지확장제 물 제한, 이뇨제, 항응고제, 스테로이드제 Sleep apnea Obstructive sleep apnea Description The most common type of breathing disorder during sleep and is characterized by repeated periods of apnea (>10seconds) and diminished airflow (hypopnea). A partial or complete obstruction occurs due to upper airway narrowing that results from relaxation of the pharyngeal muscles or from the tongue falling back on the posterior pharynx due to gravity. During periods of apnea, desaturation (hypoxemia) and hypercapnia occur; these stimulate the client to arouse and breathe momentarily to restore airflow. Assessment Loud snoring, Apnea episodes, Frequent arousal from sleep, Waking with gasping or a choking sensation During the day, client experience morning headaches, Irritability, Excessive sleepiness Description Asthma Chronic obstructive pulmonary disease (COPD) 1.Chronic inflammatory disorder of the airways▶ 1. Airflow obstruction Obstruction in the airways 2. Chronic bronchitis: bronchial tubes ▶inflamed ▶excessive mucus ↑ 2. Marked by airway inflammation, hyperresponsiveness to triggers Emphysema: air sacs in the lungs▶ damaged, enlarged ▶ hyperinflation, 3. in a client with an asthma exacerbation, a high eosinophil count would breathlessness indicate an allergic trigger for the asthmatic response. Risk factors 3. ▶ pulmonary insufficiency, pulmonary hypertension, cor pulmonale Tobacco smoke(active&passive), occupational exposure to chemicals & dust, air pollution, genetics (a1- antitrypsin deficiency) Assessment X, ↓lung sounds Cough wheezing or crackles Exertional dyspnea, accessory muscle breathing, prolonged expiration, accessory muscle breathing orthopena prolonged expiration wheezing and crackles sputum Intervention tachycardia weight loss pulsus paradoxus barrel chest, congestion and hyperinflation seen on chest x-ray cyanosis cardiac dysrhythmias ↓O2 Sat ABG: respiratory acidosis, hypoxemia PTT: ↓airflow rates PTT: ↓vital capacity Peak flow 사용 자세 – sitting and leaning foward, tripod 호흡법 - 횡경막/복부/입술오므리기 급성기: 집중 산소 고파울러자세, 앉기 식이 - 고열량, 고단백, 비타민, 조금 자주 식사, 물 섭취 3L 산소, 식이 제한- 가스형성, 매운, 너무 뜨겁거나 차갑거나 같이 있기, 활동 - as tolerated(자주 쉬기) 기관지확장제, 스테로이드제, 마그네슘 약물 - 기관지확장제, 스테로이드제, 점액용해제, 항생제(염증시) 폐청진 피할 것 – 자극 음식, 대중, 감염환자, 자극 온도, 알레르기원, 자극 향기, 담배, 먼지날리기, 청소도구 Oxygen method Venturi mask to supply the most accurate noninvasive oxygen. Description Assessment Bronchitis Emphysema Is a condition in which the bronchial tubes become inflamed and excessive Is a condition in which the air sacs in the lungs are damaged and enlarged, mucus production occurs as a result from irritants or injury resulting in hyperinflation and breathlessness Rhonchi (continuous, low-pitched adventitious breath sounds that occur when Hyperinflation of the lungs thick secretions or foreign bodies obstruct airflow in the upper airways) Flattening of the diaphragm Barrel chest (increased anteroposterior diameter of the chest) Intervention Do not exceed the oxygen flow rate >2L/min (In emphysema, respiratory drive is triggered by low oxygen levels because of long- standing hypercapnia) High fowler position, Postural drainage, Chest physiotherapy, Increase of fluid intake Albuterol Onset 5 mins Peak 45-60 mins Administration Take the medication 30 mins beforehand ensures the medication is actively preventing bronchoconstriction when the client begins exercising. Peak flow meter Description A hand-held device used to measure peak expiratory flow rate and is most helpful for clients with moderate to severe asthma. Peak flow meter uses traffic signal colors to categorize degrees of asthma symptoms. Purpose To assess asthma-related airflow limitation which helps guide treatment decisions. Comparing ongoing results with the best, stable result helps determine medication requirements. Green zone: means asthma is under control and PEF is 80-100% Yellow zone: means caution; even on a return to the green zone after use of rescue medication, further medication or a change in treatment is needed. Red zone: indicates a medical alert and needs for immediate medical treatment if the level does not return to yellow immediately after taking rescue medications. How to use Inhale deeply, place mouthpiece in mouth, and use the lips to create the seal Exhale as quick and forceful as possible through the mouthpiece of the device evaluates the degree of airway narrowing by measuring the volume of air that can be exhaled in one breath. Repeat the procedure 2 more times with a 5- to 10- seconds rest period between exhalation Record the highest of the three measured values in the peak flow log *if the peak flow is less than 80% of the personal best, administer reliever drug and retest in a few minutes. Initially, use the peak flow meter twice a day for at least two weeks when asthma is well-controlled. The peak flow meter is an assessment rather than an intervention. It determines the degree of airflow obstruction and does not improve respiratory functioning. MDI Reduce the risk of oral yeast (thrush) infections because the droplets are not deposited in the mouth. How to use MDI with a spacer MDI without a spacer The number of remaining doses is displayed on the inhaler 1. Shake MDI and remove cap 2. Attach the MDI to the spacer 3. Hold MDI upright 4. Place mouthpiece between teeth and lips 5. Activate (press) the MDI only once 6. Take 5-6 deep and slow breaths 7. Wait for at least 30 seconds before next administration 8. Rinse the mouth after the use of a steroid inhaler/ 1. Exhale completely 2. Place the inhaler between open lips or about two inches from the open mouth. 3. Start inhaling, then press down on the canister while continuing to inhale. Hold for 10 seconds. Pneumonia Description Histoplasmosis Sarcoidosis Pulmonary opportunistic fungal infection cause by spores of histoplasma capsulatum Inhalation of spores, which commonly are found in contaminated soil. Spores also are usually found in bird droppings. Immune deficiency African americans Young adults Unknown, but a high titer of Epstein-barr virus may be noted Assessment Shortness of breath, Dyspnea with ambulation, Signs and symptoms are similar to pneumonia. Confusion Nonspecific respiratory symptoms: Cough, Sputum, fever, chill Cough, flu like symptoms, dyspnea, and fever. Crackles, coarse crackles, wheezes Chest pain, pleuritic pain with inspiration Dullness, Unequal chest expansion Intervention The majority of cases resolve without treatment. Severe cases require the use of antifungal medication. Perfusion Position client to good side down Education for Avoid the use of over-the-counter cough discharging client suppressant medications Schedule a follow-up with the HCP and chest X-ray Use a cool mist humidifier in your bedroom at night. Continue using the incentive spirometer at home. Drink 1-2L of water a da. Notify HCP of any increase in symptoms Avoid tobacco smoke Eat a balanced diet Pleurisy Description Pleural effusion Inflammation of the visceral and parietal membranes; may be caused by pulmonary infarction or pneumonia. The visceral and parietal membranes rub together during respiration and cause pain. Pleurisy usually occurs on 1 side of the chest, usually in the lower lateral portions in the chest wall. Assessment Pleural friction rub heard on auscultation Knife- like sharp pain in inspiration which is aggravated on deep breathing and coughing dyspnea Intervention Monitor lung sounds Administer analgesics Apply hot or cold applications Encourage deep breathing and coughing Lie on the affected side to splint the chest Pulmonary embolism Description PE is usually caused by a dislodged thrombus that travels through the pulmonary circulation, becomes lodged in a pulmonary vessel, and causes and obstruction to blood flow in the lung Assessment Sudden pleuritic chest pain (eg, sharp lung pain while inhaling) New-onset dyspnea and hypoxemia Tachypnea and cough (dry or productive cough with bloody sputum) Hemoptysis (bloody sputum) Tachycardia Anxiety Unilateral leg swelling, erythema, or tenderness related to deep vein thrombosis Intervention Carbon monoxide poisoning Description Epidemiology Smoke inhalation, Defective heating system, Gas motors operating in poorly ventilated areas Manifestations Mild-moderate Headache, confusion, Malaise, dizziness, nausea Severe Seizure, syncope, coma, Myocardial ischemia, arrythmia Diagnosis ABG , ECG, cardiac enzymes Treatment High flow 100% oxygen using a nonrebreather mask, Intubation/ hyperbaric oxygen Tuberculosis Description 약 시작 2주 후 전염력 사라진다. 하지만 직장, 학교 복귀는 더 필요. 9개월 이상 약복용. 매 2-4주 가래검사. Risk factors Immunosuppression, age<5y, elderly, lower socioeconomic group, minority, frequent contact with untreated/undiagnosed individual, alcohol, IV users, drinking infected unpasteurized milk Transmission Airborne route by droplet infection, 2-3w treatment▶↓risk transmission Client history Past exposure of TB, live/travel TB region, recent history of respiratory disease, recent BCG vaccine Clinical manifestation Maybe asymptomatic in primary infection fatigue, lethargy, anorexia, weight loss, low fever, chills, night sweats, persistent cough w/ mucopurulent sputum – occasionally streaked with blood chest tightness, dull/aching chest pain w/ cough Chest assessment QuantiFERON—TB Gold test Sputum cultures Identifying M. tuberculosis confirms the diagnosis, 3 sputum cultures negative→ no longer infectious Tuberculin skin test Positive reaction→ previous exposure to TB or presence of inactive disease. But does not mean that active disease is present If skin test positive→ chest x-ray to rule out active TB or old head lesions The hospitalized client Airborne isolation precautions - negative pressure room, 6 exchanges of fresh air/ hour, n95 mask, (surgical mask for moving client) Client education Client will need to be isolated for at least 2 weeks. Client has to take medication for at least 9 months. Multiple drugs are used to treat the disease. Sputum test every 2-4weeks Once have tuberculosis, the test results will always be positive. Relapse of tuberculosis may occur later when the client is under stress or sick.