Pentasa & Asacol Transit Study: Gamma Scintigraphy in Human Gut
advertisement

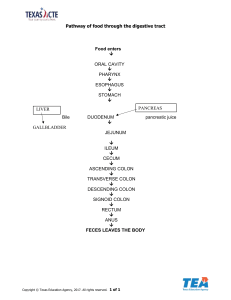
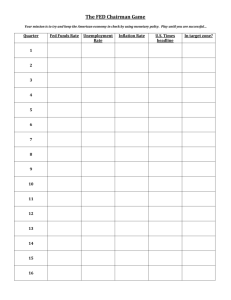
PRACTICAL GASTROENTEROLOGY A Peer Review Journal Supplement to November 1999 A SCINTIGRAPHIC STUDY TO EVALUATE WHAT HAPPENS TO PENTASA® AND ASACOL® IN THE HUMAN GUT by Ian R. Wilding PUBLISHER’S NOTE: The opinions expressed in this publication are those of the author and are not to be attributed to the sponsor or to the publisher or editorial board of Practical Gastroenterology. This research was supported by an unrestricted grant from Roberts Pharmaceuticals. A Scintigraphic Study to Evaluate What Happens to Pentasa® and Asacol® in the Human Gut Ian R. Wilding In order to ensure adequate intra-luminal mesalamine levels at the sites of intestinal lesion in inflammatory bowel disease, prolonged release (eg Pentasa®) and targeted release (eg Asacol®) products have been developed. In this study we have used the imaging technique of gamma scintigraphy to visualize the effect of food on performance of Pentasa® and Asacol® in the human gut in a group of seven healthy volunteers. The research demonstrates that gastrointestinal transit of Pentasa® is largely unaffected by food providing for uniform mesalamine delivery throughout the intestines. However, gastric residence of the enteric-coated Asacol® product was influenced by dosing after food. Interestingly, the site of intestinal delivery for Asacol® was variable in both the fasted and fed condition. Incomplete disintegration was also observed in one individual. The study highlights the importance of recognizing that our understanding of intestinal pH over the last few years has advanced significantly, questioning the relevance of using Eudragit® S coated products for colonic delivery of mesalamine. INTRODUCTION lcerative colitis (UC) is an inflammatory disease of the colonic mucosa with no known cause, which affects in all cases the rectum and possibly more proximal regions of the colon. Crohn’s Dis- U Dr. Ian Wilding is with the niche imaging CRO, Pharmaceutical Profiles, and is also a special lecturer in the Department of Pharmaceutical Sciences at Nottingham University. ease is a transmural inflammatory disease which can affect the small bowel only (30%), the colon only (25%), or both small bowel and colon at the same time (40%). Collectively these conditions are often referred to under the more generic name of inflammatory bowel disease (IBD). The use of the anti-inflammatory agent, mesalamine, to inhibit the effect of inflammatory mediators is one of the main treatment approaches in IBD (1). Mesalamine is poorly absorbed from the disPRACTICAL GASTROENTEROLOGY • NOVEMBER 1999 1 tal bowel (2) and high intra-luminal drug concentrations at the site of inflammatory lesions have been shown to be clinically important. The oral mesalamine products on the market at the present time are either prolonged release (eg Pentasa®) or targeted release (eg Asacol®) formulations. Pentasa® has been designed as a preparation consisting of a myriad of prolonged release mesalamine microspheres of circa 1 mm in diameter. Previous product visualization studies have shown that the microspheres are dispersed throughout the gastrointestinal tract and drug release occurs uniformly in both the small and large bowel (3). Enteric coatings that dissolve at relatively high pH values (eg Eudragit® S) have been used to target mesalamine delivery to the colon, eg Asacol® (4). When these type of systems were first developed, it was under the original belief that pH increased progressively from the stomach (pH 2–3), small intestine (pH 6.5-7) to the colon (pH 7–8) (5). However, subsequent studies using modern pH telemetric technology have demonstrated that the highest pH levels in the gut (pH 7.5 ± 0.5) are found in the terminal ileum (6). On entering into the colon in healthy volunteers, the pH drops to 6.4 ± 0.6 due to the presence of short chain fatty acids arising from the bacterial fermentation of polysaccharides in the right colon. Other researchers (7) have shown that in 25 % of healthy individuals the pH in the gastrointestinal tract never reaches the threshold pH of Eudragit® S (pH7). As a consequence of this new knowledge, a number of researchers have concluded that a change in luminal pH cannot be used reliably and routinely as a mechanism to deliver drugs specifically to the colon (8, 9). Gamma scintigraphy has been described as an “elegant technique for phase I investigation of the locality of in vivo release” (10) and has “become the method of choice for investigating the fate of pharmaceutical dosage [forms] in the body” (11). The ability to visualize the drug delivery process in a non-invasive manner acts to fill a significant void in current understanding. In this study, we have used gamma scintigraphy to visualize the gastrointestinal performance of two mesalamine formulations: Pentasa® and Asacol®. The objectives of the research were to investigate the effect of food on the transit of both products 2 PRACTICAL GASTROENTEROLOGY • NOVEMBER 1999 and also to assess the site of tablet disintegration for the targeted mesalamine product (Asacol®). MATERIALS AND METHODS Radiolabelling of Formulations Asacol® tablets (400 mg mesalamine) were radiolabelled by the insertion of 5 mg of 111In-labelled resin (1 MBq) into each tablet through a drilled microhole which was subsequently sealed with a cyanoacrylate adhesive. In vitro dissolution testing demonstrated that there was no significant change in the disintegration properties of the treated versus non-treated tablets. The Pentasa® capsules (250 mg mesalamine) were radiolabelled by replacing a small quantity of the capsule fill weight (circa 5% w/w) with 111In-radiolabelled ethylcellulose coated non-pareil pellets. The surrogate radiolabelled microspheres were the same size, diameter and surface coating as the currently marketed Pentasa® microspheres. Study Design & Procedures Seven healthy male and female volunteers provided written informed consent to participate in the four-way randomized crossover study. The investigation was approved by the Quorn Research Review Committee and the administration of the radiolabelled product was authorized by the Department of Health. Subjects were dosed with the radiolabelled formulation on four occasions, a minimum of 72 hours apart. On two occasions the volunteers received either the Asacol® or Pentasa® product after a 10-hour overnight fast. The remaining crossover legs involved the same product being dosed immediately after the subjects had consumed a standard breakfast (circa 2500 KJ). Time lapse photography of the gastrointestinal performance of the products was obtained via gamma scintigraphy with images being acquired every 10 minutes for 8 hours post-dose. Subsequently, images were obtained every 30 minutes until 16 hours post-dose; a final picture was also obtained at 24 hours post-dose. The scintigraphic pictures were subsequently analyzed in accordance with validated procedures (3,11). Standard meals were provided at 4 and 9 hours post-dose. RESULTS The individual transit profiles for the Pentasa® microsphere formulation have been characterized by the halflife (T50%) for gastric emptying, small bowel transit and colon arrival in both the fed and fasted state (Table 1). Gastrointestinal transit of the radiolabelled Asacol® product is provided in Table 2 and the disintegration properties are highlighted in Table 3. A sequence of scintigraphic images showing key stages of gastrointestinal performance are shown for Asacol® and Pentasa® in Figures 1 and 2, respectively. DISCUSSION a) Gastrointestinal Transit The major factor influencing the gastric emptying of oral drug delivery systems is whether they are administered with or without food. In the fasted state, drug preparations are typically retained in the stomach until they are removed by the phase III contractions of the migrating myoelectric complex (MMC). Gastric emptying occurred on average at 0.3 ± 0.1 and 0.9 ± 0.9 hours post-dose for the Pentasa® and Asacol® preparations, respectively. These data demonstrate that the two formulations were discharged from the stomach well within the 120–140 minute MMC cycle following administration in the fasted state. In the fed state the rate of stomach emptying is such that the number of calories delivered to the duodenum tends to be constant with time. Therefore, one typically sees less agitation early after high fat dosing whilst the stomach becomes accustomed to the calorific content of the ingested meal. Then agitation and mixing commence with the gradual emptying of material of appropriate particle size from the stomach. As a consequence it is not surprising that the gastric emptying of both the Asacol® and Pentasa® formulations was generally slower following post-prandial administration. However, it is important to distinguish between the effect of food on the rate of gastric emptying for the Asacol® and Pentasa® formulations. Gastric emptying of the Asacol® tablet occurred on average over 2 hours later when the dosage form was administered after food, with the gastric residence time of the formulation ranging from 2.2 to 4.4 hours post-dose following post-prandial dosing. In comparison, gastric emptying of the Asacol® tablet when dosed to fasted subjects occurred within 1 hour of dosing in five of the seven volunteers, and the duration of Table 1. The Effect of Food on the Gastrointestinal Transit (T50%) of the Labelled Microsphere Formulation (time in hours) Subject Number Fed 01 02 03 04 05 06 07 1.6 1.5 1.8 1.3 1.6 0.9 1.7 Mean SD Median n= 1.5 0.3 1.6 7 Gastric Emptying Fasted Small Intestinal Transit Fed Fasted Fed Colon Arrival Fasted 0.3 0.3 0.3 0.5 0.2 0.4 0.4 4.2 6.2 * 3.2 3.8 4.8 3.3 4.3 11.1 5.5 3.0 7.2 4.0 6.7 5.8 7.7 * 4.5 5.4 5.7 5.1 4.5 11.4 5.8 3.6 7.4 4.3 7.0 0.3 0.1 0.3 7 4.3 1.1 4.0 6 5.9 2.7 5.5 7 5.7 1.1 5.6 6 6.3 2.7 5.8 7 *T50% colon arrival did not occur during the 16-hour imaging period PRACTICAL GASTROENTEROLOGY • NOVEMBER 1999 3 Table 2. The Effect of Food on the Gastrointestinal Transit of Asacol® (time in hours) Subject Number Fed 01 02 03 04 05 06 07 3.2 3.5 2.5 2.4 2.2 4.4 3.5 Mean SD Median n= 3.1 0.8 3.2 7 Gastric Emptying Fasted Small Intestinal Transit Fed Fasted Fed Colon Arrival Fasted 0.6 0.4 2.0 0.2 0.7 0.2 2.3 4.1 * 6.3 3.9 2.7 * 3.6 6.4 9.0 4.9 3.2 6.8 3.5 5.5 7.3 * 8.8 6.3 4.9 * 7.1 7.0 9.4 6.9 3.3 7.5 3.6 7.8 0.9 0.9 0.6 7 4.1 1.3 3.9 5 5.6 2.0 5.5 7 6.9 1.4 7.1 5 6.5 2.2 7.0 7 *Tablet disintegration occurred in the small bowel Table 3. The Effect of Food on the In Vivo DIsintegration Properties of Asacol® (time in hours) Fed Subject Number Initial Disintegration Time Location 01 02 03 04 05 06 07 7.5 * 6.0 5.4 3.2 5.7 9.2 Mean SD Median n= 6.2 2.1 5.8 6 AC * SI SI SI SI AC Fasted Complete Disintegration Time Location Initial Disintegration Time Location 8.2 4.8 ** 10.9 12.8 6.8 19.9 6.5 3.4 7.4 3.8 12.2 9.6 4.6 HF SI ** AC SF SI SF 10.6 5.4 9.6 6 6.8 3.2 6.5 7 *Initial disintegration could not be confirmed **Complete tablet disintegration did not occur during the study period SI = Small intestine, AC = ascending colon, HF = hepatic flexure, TC = transverse colon, SF = splenic flexure 4 PRACTICAL GASTROENTEROLOGY • NOVEMBER 1999 SI SI AC AC TC HF SI Complete Disintegration Time Location 14.6 9.4 19.9 7.2 14.2 19.6 20.2 15.0 5.3 14.6 7 HF AC SF AC SF TC SF Figure 1. Gastrointestinal transit of the labelled Asacol® tablet following fed dosing in subject 3. PRACTICAL GASTROENTEROLOGY • NOVEMBER 1999 5 Figure 2. Gastrointestinal transit of the labelled microspheres (Pentasa®) following fed dosing in subject 3. 6 PRACTICAL GASTROENTEROLOGY • NOVEMBER 1999 residence ranged from 0.4 to 2.3 hours. Gastric emptying of the Pentasa® formulation (T50%) was slightly slower following fed dosing. However, the overall rate of gastric emptying in the presence of food was generally faster than that seen for the Asacol® tablet, with gastric emptying (T50%) of the Pentasa® formulation occurring within 2 hours of dosing on all except one occasion following fed dosing. This suggests that although the presence of food may have delayed the onset of gastric emptying for the Pentasa® product, the overall rate of gastric emptying remained rapid following post-prandial administration of the dosage form. Small intestinal transit data for the two formulations in either the fed or fasted state were, broadly speaking, comparable; circa 5 hours. Previous studies have shown that the small bowel transit of pharmaceutical products ranging from pellets to tablets is not affected by the ingestion of food (12). The Pentasa® microspheres were observed to disperse fully within the colon in the majority of individuals (Figure 2). This finding is in good agreement with previous scintigraphic studies on the Pentasa® tablet preparations (3,13). These studies showed drug release from the Pentasa® formulation occurred throughout the gastrointestinal tract allowing for topical delivery of mesalamine to a range of inflammatory lesions in the bowel. b) Pentasa® Capsule Disintegration The hard gelatin capsule containing the labelled microspheres rapidly disintegrated in the stomach releasing the prolonged release multiple dose units. Previous studies have shown that mesalamine release for the product is essentially complete during total GI transit time (14). Therefore any microspheres found in the stools on defecation will have released most of their available drug. c) Asacol® Tablet Disintegration Initial tablet disintegration occurred, on average, 6 hours post-dose following fasted and fed dosing. However, in the fasted state, onset of disintegration typi- cally occurred more distally in the intestine, eg n = 4 in the colon, whereby following post-prandial administration start of break-up occurred in the upper bowel in four individuals. Complete disintegration occurred more rapidly following fed administration; 10.5 ± 5 hours post-dose, compared to 15.0 ± 5.3 hours following fasted dosing. The site of complete disintegration also varied between regimens, with complete disintegration occurring in the colon following all seven administrations in the fasted state. However, in comparison, only six of the seven tablets dosed following fed administration completely disintegrated; the tablet for Subject 3 did not completely disintegrate during the 24 hour imaging period (Figure 1). Complete disintegration occurred in the small intestine in two subjects and the colon in the remaining four subjects receiving this regimen. It is therefore clear from these findings that the site of intestinal mesalamine delivery for the Eudragit® S coated Asacol® product is variable. In some individuals complete drug release occurred in the small bowel (eg Subjects 2 and 6 in the fed state) whilst in Subject 5, in the fasted state, drug release only started in the transverse colon. In addition, incomplete release of drug in Subject 3 following post-prandial dosing supports the anecdotal reporting of intact Asacol® tablets being observed in the stools of some patients (15). Previous scintigraphic studies have also demonstrated highly variable in vivo release properties for Eudragit® S coated tablets (16). Variation in intestinal pH is the logical explanation for the poor targeting specificity of Eudragit® S coated products in these healthy volunteers studies (6). However, it is also important to recognize that there is now a growing body of evidence to suggest that in patients with active UC there is the potential for intraluminal pH levels to be lowered considerably. Intraluminal gastrointestinal pH was assessed by Fallingborg et al, in patients with active UC (17). In half the individuals, very low pH levels (pH 2–3) were recorded in the proximal colon. In the research by Raimundo et al, the right sided luminal colonic pH in acute UC and UC in remission was found to be significantly lower than in healthy volunteers (18). Examination of the individual small intestinal pH findings in UC patients showed that in 24% of individuals a luminal pH of 7.0 or greater was PRACTICAL GASTROENTEROLOGY • NOVEMBER 1999 7 sustained for less than 30 minutes. The authors speculate that suboptimal mesalamine release from Asacol® may occur in a small proportion of UC patients. The results of our scintigraphic findings are in good accord with their concern about the variability of Asacol® ’s disintegration properties. CONCLUSION In summary, the transit results of this study indicate that administration of Asacol® following a meal can lead to increased gastric residence which ultimately delays arrival of the product at the target area for drug action. However, in comparison, the gastrointestinal transit of the multiparticulate Pentasa® formulation was less affected by the presence of food which correlates with previous food effect studies on pellet preparations. In addition, the disintegration of the Asacol® preparation was variable with complete break up of the tablet occurring in many different parts of the gut ranging from small intestine to splenic flexure. The results of the study are therefore consistent with previous research which has suggested that the Eudragit® S coating should not be used to reliably deliver drugs specifically to the colon. Pentasa®, on the other hand, performed much more consistently. Disintegration of the capsule occurred in the stomach. The microspheres then dispersed throughout the entire gastrointestinal tract from the small intestine through the distal colon in both the fasted or fed conditions. ■ References 1. Khan AZ, Piris J, Truelove SC: An experiment to determine the active therapeutic moiety of sulphasalazine. Lancet 1977;ii:892895. 8 PRACTICAL GASTROENTEROLOGY • NOVEMBER 1999