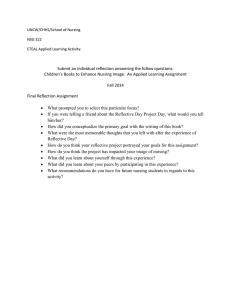
REVIEW A review of evidence-based practice, nursing research and reflection: levelling the hierarchy Stefanos Mantzoukas Methods), P gC ert T&L BS c (Nursing), BS c (Health Studies), MS c, P hD, RGN, P gD ip (Social Research Lecturer in Adult Nursing, Institute of Health & Human Sciences, Thames Valley University, London, UK Submitted for publication: 2 June 2006 Accepted for publication: 17 October 2006 Correspondence: Stefanos Mantzoukas 22 Brentmead Gardens Park Royal NW10 7DS London UK Telephone: þ44 0208 280 5357 E-mail: smantzoukas@hotmail.com 214 M A N T Z O U K A S S ( 2 0 0 8 ) Journal of Clinical Nursing 17, 214–223 A review of evidence-based practice, nursing research and reflection: levelling the hierarchy Aim. This paper examines the evidence-based practice movement, the hierarchy of evidence and the relationship between evidence-based practice and reflective practice. Background. Evidence-based practice is equated with effective decision making, with avoidance of habitual practice and with enhanced clinical performance. The hierarchy of evidence has promoted randomized control trials as the most valid source of evidence. However, this is problematic for practitioners as randomized control trials overlook certain types of knowledge that, through the process of reflection, provide useful information for individualized and effective practice. Method. A literature search was undertaken using CINAHL, medline and Ovid electronic databases in early 2006. The search terms used were: evidence-based practice, research evidence, evidence for practice, qualitative research, reflective practice, reflection and evidence. Other sources included handpicking of books on evidence-based practice, reflection and research. Only material written in English was included. Findings. The hierarchy of evidence that has promoted randomized control trials as the most valid form of evidence may actually impede the use of most effective treatment because of practical, political/ideological and epistemological contradictions and limitations. Furthermore, evidence-based practice appears to share very similar definitions, aims and procedures with reflective practice. Hence, it appears that the evidence-based practice movement may benefit much more from the use of reflection on practice, rather than the use of the hierarchical structure of evidence. Conclusion. Evidence-based practice is necessary for nursing, but its’ effective implementation may be hindered by the hierarchy of evidence. Furthermore, evidence-based practice and reflection are both processes that share very similar aims and procedures. Therefore, to enable the implementation of best evidence in practice, the hierarchy of evidence might need to be abandoned and reflection to become a core component of the evidence-based practice movement. Relevance to clinical practice. Provides an elaborated analysis for clinical nurses on the definition and implementation of evidence in practice. Ó 2007 The Author. Journal compilation Ó 2007 Blackwell Publishing Ltd doi: 10.1111/j.1365-2702.2006.01912.x Review EBP, nursing research and reflection: levelling the hierarchy Key words: evidence-based practice, hierarchy, nurses, nursing, reflection Introduction It is unequivocal that evidence-based practice (EBP) has become an imperative for clinical decision making of contemporary nurses. Furthermore, an explicit link has been drawn between EBP and the findings from randomized control trials (RCT). RCTs are situated at the top of the hierarchy of evidence and are considered to be the most valid form of evidence, whereas other forms of evidences emerging from reflective processes are regulated by being projected as weak or invalid evidences (Ellis 2000, Lake 2006, Morse 2006b, Rolfe & Gardner 2006). This paper will examine if the rationale of a hierarchy of evidence is justified and, perhaps more importantly, if it is useful for nursing practice. Finally, conclusions will be drawn on the role of EBP for nursing and on judging the validity of evidence for practice. Background The aim of EBP from its’ early days in the form of evidencebased medicine was to provide the appropriate means for making effective clinical decisions, for avoiding habitual practice and for enhancing clinical performance (EvidenceBased Medicine Working Group 1992, Davidoff et al. 1995). As nurses increasingly have acquired active participation in decision making in practice the need for effective and justifiable decisions that would lead to enhanced practice via the use of best evidence has been considered crucial. Furthermore, policy, political and professional imperatives have further made EBP a clinical prerequisite for daily practice (Department of Health 1999, Royal College of Nursing 2003, Holleman et al. 2006, Rycroft-Malone 2006). Notwithstanding the imperative of EBP for current nursing, nonetheless, two fundamental questions remain largely unclear about the EBP movement. Firstly, what justifies ‘something’ as evidence and secondly, when practitioners are faced with two opposing sets of evidence, which of the two prevails. For some writers, the first question is considered to be a clear-cut issue suggesting that research findings, clinical expertise, expert knowledge, patient preferences, policy reports and benchmarking data are the constitutional components of evidence (Goode & Piedalue 1999, Ingersoll 2000, Kitson 2002). Furthermore, the second question similarly appears to be answered as well, by arranging the above components into a hierarchy with the findings from systematic reviews of RCTs and single RCTs to be considered as the highest level of evidence and the rest to be considered as lower level evidence (Sackett 1993, McKenna et al. 2000, Page & Meerabeau 2004, Morse 2006a). Hence, in case of a dispute between two opposing sets of evidence, obviously the one higher up the hierarchy will prevail. However, this is problematic for a set of other writers, firstly, because such linearity and orderliness as is prescribed by the hierarchy of evidence does not exist in the reality of daily practice. Daily practice, in contrast to well designed and executed RCTs, is complex and uncertain. The findings of research trials are usually not directly transferable to individual patient cases because of the multiple and diverse characteristics of each patient that are not fully compatible to those patients that responded positively in the trial (Franks 2004, Rolfe & Gardner 2006, Jenicek 2006). Secondly, practicing nurses do not always use RCTs to make daily clinical decisions. In fact, the majority of daily nursing decisions are based on various other types of knowledge that do not emerge from RCTs, such as experiential knowledge, personal knowledge, practice knowledge, practical knowledge, aesthetic knowledge and ‘knowing-how’ knowledge (Reed et al. 1997, Edwards 2001, Geanellos 2004). Thirdly, the relevant hierarchy of evidence ignores or discourages the use of various types of research and knowledge because they are considered as ‘weaker’ or ‘lesser’ evidence and an imperative is expressed for the re-conceptualization of evidence and the need to produce new definitions for EBP (Buetow & Kenealy 2000, Jennings & Loan 2001, Gilgun 2006, Morse 2006a). Lastly, current articles are still unclear about the nature of evidence in EBP and continue to ask the question ‘what counts as evidence in EBP’ (Lake 2006, Whalle et al. 2006). Therefore, the aim of this paper is to analyse critically the aims, intentions and processes of the EBP movement, to identify if these aims and intentions are best achieved in nursing by using RCTs and to explore the relationship between the EBP process and the reflective process. Eventually, conclusions will be drawn on the role of the EBP movement for nursing, on the usefulness of the hierarchy of evidence and on the relationship between EBP and reflection. Ó 2007 The Author. Journal compilation Ó 2007 Blackwell Publishing Ltd 215 S Mantzoukas Method A search of the published literature on EBP, nursing research and reflection was conducted in early 2006 using the electronic databases CINAHL, Ovid and Medline. The following keywords were used: EBP, research evidence, evidence for practice, qualitative research and evidence, reflective practice and EBP, reflection and evidence. The search was restricted to English language articles and it yielded 1114 references. Initially the titles of the retrieved material were reviewed and from this initial review approximately 400 articles were rejected, because the keywords were part of a journal’s title, rather than of an article. Consequently, the abstracts were screened and from this process over 500 articles were excluded because the concept of EBP, research and reflection were not the prima foci of the article or because the articles superficially used these terms or because some of the articles were duplicated in the search process. The electronic search was supplemented by search and handpicking of books from the university library on the relevant topics. Eventually, a total of 200 full text articles and 16 book chapters were included in the review. The data were read and re-read by the author as to acquire an in-depth understanding of the phenomena and achieve data saturation, a technique that the literature requires for qualitative reviews as the present one (Booth 2001, JonesLloyd 2004). The data were reduced to a total of 66 articles and book chapters with special attention taken as to include a comprehensive list of seminal articles and articles with conflicting arguments. Findings probably most quoted definition of evidence-based medicine, which is the forerunner of the EBP movement, suggests the de-emphasis of ‘intuition, unsystematic clinical experience and pathologic rationale’ for clinical decision making and instead places emphasis on ‘the examination of evidence from clinical research’ (Evidence-Based Medicine Working Group 1992). The use of up to date research is considered on one hand to be a ‘more scientific’, legitimate and sound approach for clinical decision making and on the other hand it is anticipated that it can eliminate irrational acts or guess work from daily practice (Page & Meerabeau 2004, Rashotte & Carnevale 2004). Eventually, decisions that are based on scientific clinical research are considered to increase effectiveness, to minimize the possibility of error and to standardize practice (Rashotte & Carnevale 2004, Parahoo 2006). Intriguingly, and perhaps ironically, while the initial definition of EBP movement assiduously rejected intuition, routine practice and unarticulated experience, more recent definitions partly re-treat from this initial view to incorporate experiences, individual perceptions and tacit ways of knowing of both health professionals and patients. For instance, Sackett et al. (1996) following the position paper of the EBMWG went on to emphasize that ‘the practice of evidence-based medicine means integrating individual clinical expertise with the best available external clinical evidence from systematic research’ (p. 71). French (2002) moves even further away from the initial EBM definition, to suggest that EBP is ‘the systematic interconnecting of scientifically generated evidence with the tacit knowledge of the expert practitioner’ (p. 253). Equally, Kitson (2002) proposes that: ‘EBP should embrace ways of being able to demonstrate the effective- Defining and implementing evidence-based practice ness of expert knowledge on individual and collective patient decisions; It is avowedly accepted by the nursing literature that EBP is not only a timely catchphrase or mantra (Jenicek 2006, Rycroft-Malone 2006) but, most importantly, it is a phrase associated with science, rationality and best practice and any argument opposing it is seen as irrational, unscientific and potentially dangerous (Walker 2003, Rolfe 2004, RycroftMalone 2006). The literature seems to inextricably align EBP with best practice (Walker 2003, Tolson et al. 2005), with doing the right thing (Muir-Gray 1997), with avoiding harmful interventions (Brocklehurst & McGuire 2005) and with transparent, accountable and legally defensible decisions (Page & Meerabeau 2004, Parahoo 2006). Indeed, advocates for basing practice on evidence have up to a point cogently argued that practice on hearsay, ritual, route and intuition should be avoided. The initial and 216 the impact of existing research and outcomes and the ability to integrate patient experiences into decisions about outcome’ (p. 181). Similarly, MacPhee and Pratt (2005) expand the definition of evidence beyond research data, benchmark data and internal data, to include patient and family preferences and clinical expertise. Lastly, Berwick (2005) also argues for the need to broaden the definition of EBP to include everyday effective problem-solving approaches that are different from formal science which, in the world of clinical care, when used well and consciously, have plausible validity. Ineluctably and in some ways more significantly, the actual implementation of evidence in daily practice has currently acquired greater eminence in the health literature rather than the definitions of EBP. The literature appears to acknowledge that EBP is a prescriptive process of making decisions for Ó 2007 The Author. Journal compilation Ó 2007 Blackwell Publishing Ltd Review Table 1 The process of implementing evidence in practice Simpson (2004) considers evidence-based practice (EBP) to be a four step process involving: (a) the identification of the issue or problem, (b) the search of the literature for research, (c) the evaluation of research, (d) the action based on the evidence. Parahoo (2006) views EBP as a five step process involving: (a) the formulation of a clear question related to policy or practice, (b) the search of relevant research studies, (c) the appraisal of selected studies, (d) the analysis and the synthesis of the findings, (e) the dissemination of results and implementation of evidence. Thomson et al. (2004) suggests that integrating evidence within clinical reality involves a five step process involving: (a) forming clinical question in response to a recognized information need, (b) searching for the most appropriate evidence, (c) critically appraising the retrieved evidence, (d) incorporating the evidence into a strategy for action, (e) evaluating the effects of any decisions and actions taken. Holleman et al. (2006) advocate that the introduction of EBP into daily practice may involve a six step process involving: (a) assessment of the need for practice changes, (b) linking problem interventions and outcomes, (c) synthesis of best evidence, (d) design of practice change, (e) implementation and evaluation of practice change, (f) integration and maintenance of EBP change. patient care and treatment (McKenna et al. 2000, Thomson et al. 2004). The implementation of evidence in the real world of practice as outlined by various authors (Table 1) includes a series of steps or processes. These steps include; (i) the analysis of the clinical reality and the formation of questions from practice that require answering; (ii) search for appropriate research or other literature on the relevant practice issue; (iii) critically analyse, appraise and evaluate these materials; (iv) synthesize or integrate these materials with the context of clinical reality as to act and resolve the specific problematic clinical situation; and (v) evaluate the actions based on the research or literature information and how they impacted (or not) on the resolution of the problematic situation. In summary, the EBP movement purview is understood as a conscious, explicit and logically articulated decision-making process that allows transparency, ensures best practice and avoids errors that are related to rote or habitual practice. Moreover, EBP is viewed as a process that can be compartmentalized in a series of steps that practitioners can follow. Finally, despite that clinical expertise and patient preferences have been incorporated in EBP definitions, nonetheless the EBP, nursing research and reflection: levelling the hierarchy core elements of EBP remain the results from research findings. Moreover, as it will become explicit in the following section, it is the results from a specific type of research, namely those emanating from clinical trials that are considered as the most valid source of evidence. The role of nursing research in evidence-based practice Despite the fact that recent definitions on EBP include personal and professional experience and specific contexts and situations, nonetheless, on closer analysis, it appears that at the crux of the EBP movement is the promotion of research findings as the most (if not only) justifiable form of evidence. A series of authors have argued (either dissenting or consenting) that RCTs and systematic reviews are in essence the corner stone or the crown prince or the golden standard for the EBP movement (Walker 2003, Franks 2004, Mistiaen et al. 2004, Berwick 2005, Rycroft-Malone 2006). Moreover, this is perpetuated by the very idea that a hierarchy has been developed in defining the validity of evidence (Figure 1). At the top of this hierarchy (and hence the most valid source of evidence) are the findings from systematic reviews of RCTs and the next level down the hierarchy are evidence from at least one well conducted RCT. The next three levels down the pyramid are evidence from controlled research that lack randomization, research without a control group and opinions of respected authorities. Interestingly, the last three levels are not recommended to inform practice, thus assuming that they are not sufficient evidence to base practice (Sackett 1993, McKenna et al. 2000, Morse 2006b). Lastly, the introduction of guidelines that are based on the most updated RCTs, the development of RCT databases, the creation of evidence based journals that contain primarily RCT abstracts and the experimentation with computerized decision supporting systems that are based on RCT reviews, further reinforce the dominance of Meta-analysis of RCTs At least one well-conducted RCT Controlled research without randomization Research without experimental study Opinions of respected authorities Figure 1 The hierarchy of evidence. Ó 2007 The Author. Journal compilation Ó 2007 Blackwell Publishing Ltd 217 S Mantzoukas RCTs as the most valid source of evidence (Mistiaen et al. 2004, Brocklehurst & McGuire 2005, Haynes 2005, WalkerDilks 2005). However, the promotion of RCTs as the most valid source of evidence sits uncomfortably with many writers, academics and practitioners in the health field and to such an extent is this discontent, that some go to other side suggesting that the EBP movement should either be re-structured or even discarded (Walker 2003, Geanellos 2004, Hancock & Easen 2004). It is what Forbes (2003) views as the ‘danger of throwing the baby out with the bath water’. The concerns relating to the promulgation of RCTs as the only valid form of evidence can be summarized into three broad aspects, namely: practical, political/ideological and epistemological. The first concern has to do with the impracticality of implementing the findings of RCTs as evidence in daily practice. It is argued that the very nature of RCTs can answer specific and limited questions (McKenna et al. 2003, Maier 2006, Mol 2006). The questions that RCTs can answer are ones of comparison between drugs or treatments and can produce conclusions as to which has better effects, but not necessarily, which is more effective. Effectiveness has to do with meeting the needs and overall aims of the individual in specific and unique contexts. However, because both the individual needs and the contexts are unique, unavoidably clinical aims and goals are also individual and unique. Hence, what is effective treatment for a specific individual in a specific context is determined by their unique aims and goals. The very nature of RCTs necessitate the de-contextualization, homogenization and generalization and can only provide answers to acontextual situations were goals and aims are identical and general (van Meijel et al. 2004, Pearson et al. 2004, Ellis 2005, Mol 2006, Morse 2006c, Rycroft-Malone 2006). Furthermore, practitioners are busy professionals dealing with complex and unique clinical problems that require on the spot decisions to be made. It is, therefore, virtually impossible to stop before every decision is to be made and retreat back to the library to retrieve all relevant RCTs. Hence, either the practitioners will rely on their memory of RCTs that they have read with the fallibility and selectivity that this entails (Newell 1992, Rolfe 2005) or will rely on guidelines as developed from RCTs by opinion leaders with the restrictive effect that this has on practitioners initiative and autonomy (McKenna et al. 2000, Lorenz et al. 2005). The second aspect of concern in promoting RCTs as the most valid form of evidence for practice are the underlying political and ideological assumptions. To put it more bluntly and perhaps fairly cynically, part of the literature propounds that the ideology of professional control and the operation of power, authority and economy has significantly contributed 218 in equating the EBP movement with research emanating from RCTs. Larner (2004) adamantly suggests that it ‘is not a question of evidence or no evidence, but who controls the definition of evidence and which kind is acceptable’ (p. 20). In simple terms, endorsing RCT findings as the most valid source of evidence is to remove the expertise and authority from the practitioners in defining practice and bestowing this expertise and authority to researchers, academics and educationalists. Practitioners do not have the time or the resources and in some cases the expertise to carry out or appropriately critique RCT studies. It is researchers, academics and educationalists that usually carry out RCTs or review and critique them. However, researchers, academics and educationalists are mainly not involved in the reality of daily practice and cannot have control, if the findings of their RCT studies will ever be implemented in practice. Therefore, the only way for these professional groups to make sure that their research will acquire significance is to impose their findings upon practitioners as the only valid form of evidence for clinical decision making (Freshwater & Rolfe 2004, Rolfe & Gardner 2005, Rycroft-Malone 2006). The move towards integrating researchers, academics and educationalists in daily practice reality and involving practitioners with research, education and academia can become a starting point for addressing this covert power game regarding the validity of RCTs. Lastly, this covert political agenda of imposing practice decisions on practitioners is not irrelevant to what Walker (2003) defines as ‘economic rationalism’, but rather an extension of the politics of power. The assumption here is that money is the ‘bottom line’ and the greater the cost effectiveness of daily practice, the better. However, for the most cost-effective practice to be implemented it is required that practitioners are conditioned or controlled as to base their practice on predefined and clear-cut guidelines with predictable and beforehand cost estimations. Interestingly, the people who make the decisions on the distributions of funds are in part the same people who carry out research and develop practice guidelines (Walker 2003, Morse 2006b, Rycroft-Malone 2006). By controlling and standardizing clinical practice, on the one hand, they are able to control in a predicative fashion the expenditure of money and on other hand, they can make sure that they impose their research findings in practice. Finally, the third concern in promoting RCTs as the most valid form of evidence for practice relates to epistemological contentions. It is suggested that RCTs are not suitable for practitioners because practice is complex, uncertain, contextual and practitioners rely on more than one type of knowledge, which RCTs are unable to accommodate Ó 2007 The Author. Journal compilation Ó 2007 Blackwell Publishing Ltd Review (Geanellos 2004, Tarlier 2005, Rycroft-Malone 2006). In very simple terms, this argument takes the form of positivism vs. non-positivism debate. RCTs are considered to follow the canons of the positivist paradigm aimed at acquiring the objective facts, the single ‘right’ answer and the general and unchangeable laws of nature and society (Mantzoukas 2004). This is achieved by applying strict methodological rules of objectivity and stringent control of contextual variables (Mantzoukas 2005, Weaver & Olson 2006). The end result is generalized knowledge based on explanations of objectively identified phenomena (Forbes et al. 1999). However, it is debated that the manifold variables of the practice environment cannot be controlled and practitioners cannot be objective because the kernel of practice is human interactions and the understanding of subjective perceptions (Edwards 2001, Rolfe et al. 2001). Moreover, practitioners cannot acquire absolute or single ‘correct’ answers because answers and solutions for daily practice need to be constructed or fabricated as to fit individual cases. Thus, RCTs whilst very useful when the aim is to acquire factual knowledge, objective answers and predictive generalized theories, nevertheless it is of limited use when practitioners aim at understanding individual patient perception, acquiring personal knowledge and carrying out specific activities as to care and cater for specific patient needs (Forbes et al. 1999, Edwards 2001, Rolfe 2006, Weaver & Olson 2006). In fact, it is propounded that even the implementation of the objective and generalized results of RCTs, paradoxically require the subjective interpretation of the individual practitioner. Practitioners are required to use their subjective judgement to identify the similarities between the subjects that participated in the study and the patient they are caring for and interpret the benefits and harms of the specific treatment (Lake 2006). Hence, it is assumed that, epistemologically, daily practice is much closer to the interpretive or postmodern paradigms and that the validity and value of evidence ought to be considered by the criteria of these paradigms (Rolfe 2004, De Simone 2006). In summation, the EBP movement has been identified to have a very close relation with research and specifically with RCTs and systematic reviews of RCTs. In fact, it is projected and has come to be accepted that RCTs are the most, if not the only, valid form of evidence. This has been achieved by various mechanisms, most important of which is the development of a hierarchy of evidence. Nonetheless, the equation of evidence with RCTs makes not only for uncomfortable reading in some quarters of the literature, but most importantly for potentially ineffective practice. Firstly, it is impractical for practitioners to base the majority of clinical decisions on RCTs because daily practice EBP, nursing research and reflection: levelling the hierarchy primarily requires on the spot decision making that RCTs cannot facilitate. Most importantly, RCTs can only provide limited information for practitioner as they can only inform on which drug or treatment has better effects, if compared with another drug or treatment, but not which is more effective for a specific patient. Secondly, the EBP movement is seen as a suspect enterprise where the politics or ideology of power and economics are the ones that have defined RCTs as the golden standard of research and the most valid form of evidence and not their capacity for best practice. Thirdly, it is considered that the imposition of RCTs as the only valid form of evidence for practice revokes previous and well rehearsed debates on epistemological issues and represents nothing other than an attempt of the positivistic paradigm to impose its’ methods on practitioners. However, this remains problematic because, on the one hand, the positivistic epistemology cannot explain the complexity of daily practice and on the other hand, the reality of practice appears to be much closer to the interpretive and postmodern paradigms. Therefore, for daily practice the concept of evidence carries subjective and interpretive connotations that seem to have a direct linkage with reflective methods of practising, rather than with findings from RCTs. Reflective practice and evidence The epistemological uneasiness that positivism introduces via the use of RCTs as the only valid form of evidence has been rehearsed before and in another forum, namely that of reflection and reflective practice. The disassociation of theory from action and practice, whereby theory is developed by strict methodological canons of research to dictate actions or practice has been problematic for a series of philosophers, such as Marx, Dewey and Rorty. For these philosophers knowledge is not something that should correspond to some antecedent truth, super-imposed reality or predefined description of the world, but rather knowledge is something emergent that is always in a dialectical interplay with experience and action and as such requires continuous interpretation or re-description. In simple words, knowledge is inextricably linked with action and in specific with good action, with what works and with what is effective. Therefore, knowledge should not enclose an absolutely true picture of the world acquired through methodological rigor of control and randomization, but instead it should open up the possibility of various descriptions of practice experiences and actions that would identify the most useful or most effective experience or action. Essentially they suggest that knowledge and advancement of knowledge emerges from our interpretive Ó 2007 The Author. Journal compilation Ó 2007 Blackwell Publishing Ltd 219 S Mantzoukas descriptions of the effectiveness or not of our experiences and actions (Gallagher 1964, Eagleton 1999, Calder 2003). It is this concept that knowledge emerges from actions and practice experiences that spearheaded writers as Schon (1983) to develop the concept of reflection as means for acquiring and developing professional knowledge. Schon (1983, 1987) was concerned that research based knowledge encapsulated in theories provided linear, certain and clear-cut solutions, but practice reality is non-linear, uncertain, complex and conflicting. Therefore, research based knowledge as expressed by positivism does not provide answers to practitioners and does not guarantee best practice. According to Schon, practitioners need to implement reflective techniques to name and frame unique problematic situations and from there on, to find a workable unique solution to their problems. Furthermore, Schon advocated that, by consciously analysing the problematic situation and the implemented actions, lessons can be learned that can be used to inform future practice on what works and what is more effective. Following from this health professional in general and nursing in specific, incorporated reflection as means for explicating practice, analysing the decision-making processes and ensuring the provision of unique and best care. Moreover, the nursing literature has alleged from its conception as a profession that it utilizes various types of knowledge, such as practical knowledge, personal knowledge, aesthetic knowledge and experiential knowledge (Carper 1979, Benner 1984). Whilst, these types of knowledge were considered essential for providing information necessary to treat patients in a unique, holistic and individualistic manner, nonetheless they were largely ignored because on one hand they could not be formally developed or taught and on the other hand they remained in the realm of unconscious doing and intuitive practice. However, reflection and reflective techniques of practice provided the epistemological justification of the worthiness of these types of knowledge. Most importantly, reflection provided structure and guidance to transpose these unconscious and intuitive types of knowledge into conscious types and allowed for linkages to be developed with previous knowledge, formal theories and research knowledge. In this way, a repertoire of cases could be build that would enable justification of practice (Johns 1995, Rolfe 1996, Mantzoukas 2002, Jasper 2003, Johns & Freshwater 2005). Furthermore, the literature acknowledges that knowledge emerging from reflective analysis is a process that can be compartmentalized in a series of steps that practitioners can follow (Table 2). These steps include: (i) the description or framing of feelings, situations and context; (ii) the analysis and evaluation of the situation by using various types of 220 Table 2 The process of implementing reflection in practice FitzGerald and Chapman (2000) consider that reflection is a self awareness process that requires a series of steps: (a) describe experiences, (b) critically analyse situations, (c) develop new perspectives, (d) evaluate the learning process. Gibbs (1988) model of reflection also suggests that reflection is a process with distinct steps to be followed: (a) the description of what happened and of the practitioner feelings, (b) the evaluation of what was good or about the experience, (c) the analysis or sense making of the situation, (d) the conclusions and potential alternatives in dealing with the situation, (e) the action plan for future practice. Burnard (2000) views reflection as a process that entails the following steps: (a) identifying the context, (b) locating the element by focusing on a particular event, (c) reflecting on the element, (d) disclosing, verbalizing and writing down thoughts, comments and reactions, (e) discuss other aspects of the activity and consider implications, (f) summarize the process as to function as an aide memoir for future practice. Rashotte and Carnevale (2004) consider reflection a decision making model that is characterized by five steps: (a) recognition of each case as unique, (b) framing the parameters of the unique case, (c) drawing on experience-based repertoire of examples in order to identify elements of the case that are familiar and unfamiliar, (d) conducting rigorous on the spot experiments that examine competing hypothesis, (e) maintaining an openness towards rejecting ones prior conclusions. knowledge; (iii) verbalizing understandings, drawing conclusions and developing a hypothesis or an action plan about the specific situation; (iv) implementing the action plan; (v) evaluating the outcomes of the action plan and integrating the unique situation with other types of knowledge and experiences. In summary, reflection is viewed as a process of transforming unconscious types of knowledge and practices into conscious, explicit and logically articulated knowledge and practices that allows for transparent and justifiable clinical decision making. Thus, reflection is considered to enable individualistic and holistic treatment of patients by providing best practice and avoiding unfruitful and unnecessary interventions. The underpinning element of reflection is primarily the experiences the practitioner possesses and the individual patient with the specific needs. Equally, important is the conscious effort of the practitioner to link this reflective Ó 2007 The Author. Journal compilation Ó 2007 Blackwell Publishing Ltd Review knowledge with other types of knowledge and consequently, develop a set of case repertoires. Eventually, reflection is viewed as a process that can be compartmentalized in a series of steps that practitioners can follow. Discussion Three key issues can be extrapolated from the heretofore analysis of EBP, nursing research and reflection. Firstly, the EBP movement is not only here to stay (Jenicek, 2006), but it is a responsible, accountable and professional manner for nurses to carry out their practice. However, the actual implementation of the EBP rhetoric in practice requires some attention as to identify what counts as evidence and how practitioners will judge the validity of the various types of evidence. As Forbes (2003) suggests EBP on its own is neither bad, nor good, but it is the way it is conceptualized and used that makes it useful or not. The very idea that EBP can lead to best practice through conscious and logical decision-making processes that would eventually secure maximum effectiveness for patient care is something that no health professional can or is willing to argue against. Thus, the fundamental aims of the EBP movement are useful, necessary and beneficial for both practitioners and patients and it seems appropriate for EBP to become a core component of the nursing profession. The second key issue that emerges is that, while findings from RCTs have been venerably projected as the only warrantable form of evidence for practice, nonetheless an unwitting (or not) misconception, overestimation and overall distortion of the value of RCTs as evidence is apparent. Despite that, RCTs can be used as a form of evidence, nonetheless, their value is severely curtailed by the practical limitations they pose, by the epistemological diversity and plurality of practice that RCTs cannot accommodate for and by the political and ideological implications of devaluing and limiting practitioners’ autonomy and initiative. Therefore, projecting RCTs as the most valid source of evidence is not only illusionary, but potentially dangerous, as it does not secure best practice, most effective care and optimal treatment. The third and possibly most important issue that emerges is that reflective practice and EBP are not very dissimilar ways of practising. In fact, some nurses have come to realize that reflection can provide not only valid evidences for practice, but possibly is positioned in a better place to provide more practical, useful and effective evidences (Malterud 2002, Forbes 2003, Rolfe 2005). The broadened definitions of EBP recognize that EBP is a decision-making process that enables the practitioner to consciously and explicitly choose the best treatment option for individual patients. This definition is EBP, nursing research and reflection: levelling the hierarchy very similar, if not identical, with definitions for reflection and reflective practice. Moreover, EBP and reflection are considered to be based on a series of successive steps or procedures that includes; clear description of issues and contexts, critical analysis of all variables affecting the patient situation, the development of an action plan, the implementation of the action plan and the evaluation of the action plan. Lastly, but possibly more importantly, the individual practitioner, for both EBP and reflection, remain the most important element for achieving best practice through the rational, contiguous and logical justification of choices made. Conclusion Therefore, it is suggested that the aims of the EBP movement are important and necessary aspiration for nursing practice. Moreover, the hierarchy of evidence with RCTs as the most valid form of evidence is not only in many ways flawed, but most importantly unsuitable for health practitioners. Lastly, EBP and reflection are both considered processes that share very similar aims, procedures and mechanisms. Therefore, it seems appropriate that health professionals abandon the hierarchy of evidence as it is portrayed by the literature and integrate EBP with reflective practice. In other words, the levelling or abandoning of the hierarchy of evidence will enable practitioners to practice in a reflective manner and, therefore, base their practice on conscious, justifiable and explicit evidences. References Benner P (1984) From Novice to Expert: Excellence and Power in Clinical Nursing Practice. Addison-Wesley, Menlo Park, CA. Berwick DM (2005) Broadening the view of evidence-based medicine. Quality and Safe Health Care 14, 315–316. Booth A (2001) Cochrane or cock-eyed? How should we conduct systematic reviews of qualitative research?. Available at: http:// www.leeds.ac.uk/educol/documents/00001724.htm (accessed 7 January 2006) Brocklehurst P & McGuire W (2005) Evidence based care. British Medical Journal 330, 36–38. Buetow S & Kenealy T (2000) Evidence-based medicine: The need for a new definition. Journal of Evaluation in Clinical Practice 6, 85–92. Burnard P (2000) Learning Human Skills: An Experiential and Reflective Guide for Nurses, 3rd edn. Butterworth-Heinemann, Oxford. Calder G (2003) Rorty. Wiedenfeld & Nicolson, London. Carper AB (1979) Fundamental patterns of knowing in nursing. Advances in Nursing Science 1, 13–23. Davidoff F, Haynes B, Sackett D & Smith R (1995) Evidence-based medicine: a new journal to help doctors identify the information they need. British Medical Journal 310, 1085–1086. Ó 2007 The Author. Journal compilation Ó 2007 Blackwell Publishing Ltd 221 S Mantzoukas De Simone J (2006) Reductionist inference-based medicine, i.e. EBM. Journal of Evaluation in Clinical Practice 12, 445–449. Department of Health (1999) Making a Difference: Strengthening the Nursing, Midwifery and Health Visiting Contribution to Health and Healthcare. HMSO, London. Eagleton T (1999) Marx. Phoenix, London. Edwards DS (2001) Philosophy of Nursing: An Introduction. Palgrave, Basingstoke. Ellis J (2000) Sharing the evidence: clinical practice benchmarking to improve continuously the quality of care. Journal of Advanced Nursing 32, 215–225. Ellis C (2005) Evidence-based practice: a personal journey from scepticism to pragmatism. Journal of Psychiatric and Mental Health Nursing 12, 739–744. Evidence-Based Medicine Working Group (1992) Evidence based medicine: a new approach to teaching the practice of medicine. JAMA 268, 2420–2425. FitzGerald M & Chapman Y (2000) Theories of reflection for learning. In Reflective Practice in Nursing: The Growth of the Professional Practitioner, 2nd edn (Burns S & Bulman C eds). Blackwell Science Ltd, Oxford, pp. 1–22. Forbes A (2003) Response to Kim Walker: why evidence-based practice now? A polemic. Nursing Inquiry 10, 156–158. Forbes D, King K, Kushner KE, Letourneau N, Myrick AF & Profetto-McGrath J (1999) Warrantable evidence in nursing science. Journal of Advanced Nursing 29, 373–379. Franks V (2004) Evidence-based uncertainty in mental health nursing. Journal of Psychiatric and Mental Health Nursing 11, 99–105. French P (2002) What is the evidence on evidence-based nursing? An epistemological concern. Journal of Advanced Nursing 47, 250–257. Freshwater D & Rolfe G (2004) Deconstructing Evidence Based Practice. Palgrave, Basingstoke. Gallagher TK (1964) The Philosophy of Knowledge. Sheed and Ward, New York. Geanellos R (2004) Nursing based evidence: Moving beyond evidence-based practice in mental health nursing. Journal of Evaluation in Clinical Practice 10, 177–186. Gibbs G (1988) Learning by Doing: A Guide to Teaching and Learning Methods. Further Education Unit, Oxford Polytechnic, Oxford. Gilgun JF (2006) The four cornerstones of qualitative research. Qualitative Health Research 16, 436–443. Goode CJ & Piedalue F (1999) Evidence-based clinical practice. Journal of Nursing Administration 29, 15–21. Hancock HC & Easen PR (2004) Evidence-based practice: an incomplete model of the relationship between theory and professional work. Journal of Evaluation in Clinical Practice 10, 187–196. Haynes BR (2005) Of studies, summaries, synopses and systems: The 4S evolution of services for finding current best evidence. Evidence Based Nursing 8, 4–6. Holleman G, Eliens A, van Vliet M & van Achterberg T (2006) Promotion of evidence-based practice by professional nursing associations: literature review. Journal of Advanced Nursing 53, 702–709. 222 Ingersoll GL (2000) Evidence-based nursing: what it is and what it isn’t. Nursing Outlook 48, 151–152. Jasper M (2003) Beginning Reflective Practice: Foundations in Nursing and Health Care. Nelson Thornes Ltd, Cheltenham. Jenicek M (2006) The art of soft science: evidence-based medicine, reasoned medicine or both?. Journal of Evaluation in Clinical practice 12, 410–419. Jennings BM & Loan LA (2001) Misconceptions among nurses about evidence-based practice. Journal of Nursing Scholarship 33, 121–127. Johns C (1995) The value of reflective practice for nursing. Journal of Clinical Nursing 4, 23–30. Johns C & Freshwater D (2005) Transforming Nursing Through Reflective Practice, 2nd edn. Blackwell Publishing, Oxford. Jones-Lloyd M (2004) Application of systematic review methods to qualitative research: practical issues. Journal of Advanced Nursing 48, 271–278. Kitson A (2002) Recognising relationships: reflections on evidencebased practice. Nursing Inquiry 9, 179–186. Lake APJ (2006) EBM for the future. Journal of Evaluation in Clinical Practice 12, 433–437. Larner G (2004) Family therapy and the politics of evidence. Journal of Family Therapy 26, 17–39. Lorenz AK, Ryan WG, Morton CS, Chan SK, Wang S & Shekelle GP (2005) A qualitative examination of primary care providers’ and physician managers’ uses and views of research evidence. International Journal for Quality in Health Care 17, 409–414. MacPhee M & Pratt P (2005) Evidence-based practice. Journal of Pediatric Nursing 20, 396–398. Maier T (2006) Evidence-based psychiatry: understanding the limitations of a method. Journal of Evaluation in Clinical Practice 12, 325–329. Malterud K (2002) Reflexivity and metapositions: strategies for appraisal of clinical evidence. Journal of Evaluation in Clinical Practice 8, 121–126. Mantzoukas S (2002) Exploring and Understanding Reflection, Knowledge and Everyday Practice in the Medical Wards. Unpublished PhD thesis, University of Portsmouth, Portsmouth. Mantzoukas S (2004) Issues of representation within qualitative inquiry. Qualitative Health Research 14, 994–1107. Mantzoukas S (2005) The inclusion of bias in reflective and reflexive research: a necessary prerequisite for securing validity. Journal of Research in Nursing 10, 279–295. McKenna H, Cutcliffe J & McKenna P (2000) Evidence-based practice: demolishing some myths. Nursing Standards 14, 39–42. McKenna H, Ashton S & Keeney S (2003) Barriers to evidence based practice in primary care: a review of the literature. International Journal of Nursing Studies 41, 369–378. van Meijel B, Gamel C, van Swieten-Duifjes & Grypdonck MHF (2004) The development of evidence-based nursing interventions: methodological considerations. Journal of Advanced Nursing 48, 84–92. Mistiaen P, Poot E, Hickox S & Wagner C (2004) The evidence for nursing interventions in the Cochrane database of systematic reviews. Nurse Researcher 12, 71–80. Mol A (2006) Proving or improving: on health care research as a form of self-reflection. Qualitative Health Research 16, 405–414. Ó 2007 The Author. Journal compilation Ó 2007 Blackwell Publishing Ltd Review Morse MJ (2006a) Reconceptualizing qualitative evidence. Qualitative Health Research 16, 415–422. Morse MJ (2006b) The politics of evidence. Qualitative Health Research 16, 395–404. Morse MJ (2006c) It is time to revise the Cochrane criteria. Qualitative Health Research 16, 315–317. Muir-Gray JA (1997) Evidence-Based Health Care. Churchill Livingstone, Edinburgh. Newell R (1992) Anxiety, accuracy and reflection: the limits of professional development. Journal of Advanced Nursing 17, 1326– 1333. Page S & Meerabeau L (2004) Hierarchies of evidence and hierarchies of education: reflections on a multiprofessional education initiative. Learning in Health and Social Care 3, 118–128. Parahoo K (2006) Nursing Research: Principles, Process and Issues, 2nd edn. Palgrave Macmillan, Basingstoke. Pearson MG, Barnes N, Thomas M, Tate H & Simnett S (2004) Evaluating the effectiveness of asthma treatment in real-life practice. Journal of Evaluation in Clinical Practice 10, 297–305. Rashotte J & Carnevale FA (2004) Medical and nursing clinical decision making: a comparative epistemological analysis. Nursing Philosophy 5, 160–174. Reed J, Ground I & Dunlop M (1997) Philosophy of Nursing. Arnold, London. Rolfe G (1996) Closing the Theory Practice Gap: A New Paradigm for Nursing. Butterworth-Heinemann Ltd, Oxford. Rolfe G (2004) Do we really want a modern and dependable health service?. Journal of Nursing Management 12, 79–84. Rolfe G (2005) The deconstructing angel: nursing, reflection and evidence-based practice. Nursing Inquiry 12, 78–86. Rolfe G (2006) Judgements without rules: towards a postmodern ironist concept of research validity. Nursing Inquiry 13, 7–15. Rolfe G & Gardner L (2005) Towards a nursing science of the unique: evidence, reflexivity and the study of persons. Journal of Research in Nursing 10, 297–310. Rolfe G & Gardner L (2006) Towards a geology of evidence-based practice: a discussion paper. International Journal of Nursing Studies 43, 903–913. EBP, nursing research and reflection: levelling the hierarchy Rolfe G, Freshwater D & Jasper M (2001) Critical Reflection for Nursing and the Helping Professions: A User’s Guide. Palgrave, Basingstoke. Royal College of Nursing (2003) Defining Nursing. Royal College of Nursing, London. Rycroft-Malone J (2006) The politics of the evidence-based practice movements. Journal of Research in Nursing 11, 95–108. Sackett DL (1993) Rules of evidence and clinical recommendations. Canadian Journal of Cardiology 9, 487–489. Sackett DL, Rosenberg WMC & Gray JA (1996) Evidence based medicine: what it is and what it isn’t. British Medical Journal 312, 71–72. Schon D (1983) The Reflective Practitioner. Temple Smith, London. Schon D (1987) Educating the Reflective Practitioner. Jossey-Bass, San Francisco. Simpson LR (2004) Evidence-based nursing offers certainty in the uncertain world of healthcare. Nursing Management 35, 10–12. Tarlier D (2005) Mediating the meaning of evidence through epistemological diversity. Nursing Inquiry 12, 126–134. Thomson C, Cullum N, McCaughan D, Sheldon T & Raynor P (2004) Nurses, information use and clinical decision making – the real world potential for evidence-based decisions in nursing. Evidence Based Nursing 7, 68–72. Tolson D, McAloon M, Hotchkiss R & Schofield I (2005) Progressing evidence-based practice: an effective nursing model?. Journal of Advanced Nursing 50, 124–133. Walker T (2003) Why evidence-based practice now?: a polemic. Nursing Inquiry 10, 145–155. Walker-Dilks C (2005) Contribution of the Cochrane library to the evidence-based journals. Evidence Based Nursing 8, 7. Weaver K & Olson KJ (2006) Understanding paradigms used for nursing research. Journal of Advanced Nursing 53, 459–469. Whalle AL, Sinclair M & Parahoo K (2006) A philosophic analysis of evidence-based nursing: recurrent themes, metanarratives and exemplar cases. Nursing Outlook 54, 30–35. Ó 2007 The Author. Journal compilation Ó 2007 Blackwell Publishing Ltd 223