Uploaded by
AQI LA
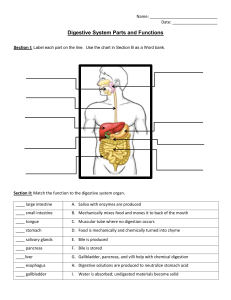
Digestive System: Organs, Functions & Processes

DIGESTIVE SYSTEM identify the main structures including organs that make up the digestive system. Identify the two groups of digestive system. describe the functions of the structures and organs of digestive system. describe the structures of the lower gastrointestinal organs. explain the actions and functions of the lower gastrointestinal organs. describe the structures of the accessory organs of the Digestive system. Explain the functions of the accessory organs of the digestive system. explain the six processes of food breakdown in the digestive system describe the phases of the digestive system. explain the implications occurring due to problems of the digestive system. INTRODUCTION The digestive system takes in food (ingests food) breaks it down physically and chemically into nutrient molecules (digests it) and absorbs the nutrients into the bloodstream. Then it rids the body of the indigestible remains (defecates). The organs of the digestive system can be separated into 2 main groups: 1. alimentary canal 2. accessory digestive organs The alimentary canal performs the whole menu of digestive functions; ingests, digests, absorbs and defecates. Organs of the Alimentary Canal Also called the gastrointestinal (GI) tract. A continuous coiled, hollow muscular tube that winds through the ventral body cavity and is open at both ends. Its organs are the Mouth Pharynx Oesophagus Stomach Small intestine Large intestine anus In a cadaver, the alimentary canal is approximately 9 meters (30 feet) long, but in a living person, it is considerably shorter because of its relatively constant muscle tone. The Accessory Organs The accessory organs are the: Teeth Salivary glands Pancreas Liver and Gallbladder The accessory organs assist the process of digestive breakdown in various ways. P a g e 1 | 11 THE ALIMENTARY CANAL MOUTH Food enters the digestive tract through the mouth, or oral cavity, a mucous-membrane lined cavity. The lips (labia) protect its anterior opening. The cheeks form its lateral walls. The hard palate forms its anterior roof and the soft palate forms its posterior roof. The uvula is a fleshy fingerlike projection of the soft palate which extends inferiorly from the posterior edge of the soft palate. The space between the lips and cheeks externally, and the teeth and gums internally is the vestibule. The muscular tongue occupies the floor of the mouth. The tongue has several bony attachments – two of these are to the hyoid bone and the styloid processes of the skull. The lingual frenulum, a fold of mucous membrane, secures the tongue to the floor of the mouth and limits its posterior movements. At the posterior end of the oral cavity are paired masses of lymphatic tissue, known as the palatine tonsils. The lingual tonsil covers the base of the tongue just beyond. Having tonsils at the oral entrance to the pharynx provide a protective value because: The mouth is a favoured site of body entry by bacteria and the presence of tonsils, lymphocyte-and -macrophage filled organs is very effective in preventing many pathogens from getting further into the digestive tract. As food enters the mouth, it is mixed with saliva and masticated The cheeks and the closed lips hold the food between the teeth during chewing. The nimble tongue continuously mixes food with saliva during chewing and initiates swallowing. Papillae containing taste buds, or taste receptors, are found on the tongue surface. Besides it food manipulating function, the tongue allows us to enjoy and appreciate the food as we eat. PHARYNX The pharynx is subdivided into: Nasopharynx –part of the respiratory passageway Oropharynx–posterior to the oral cavity Laryngopharynx–continuous with the oesophagus below. P a g e 2 | 11 From the mouth, food passes posteriorly into the oropharynx and laryngopharynx, both of which are common passageways for food, fluids and air. Walls of pharynx contain two skeletal muscle layers: The cells of the inner layer run longitudinally the outer layer (the constrictor muscles) run around the wall in a circular fashion. Alternating contraction of these two muscle layers propel food through the pharynx into the oesophagus below. OESOPHAGUS The oesophagus or gullet, runs from the pharynx through the diaphragm to the stomach. About 25cm (10 inches) long, it is essentially a passageway that conducts food to the stomach. The walls of the alimentary canal organs from the oesophagus to the large intestine are made up of 4 basic layers, or tunics: 1. The mucosa is the innermost layer, a moist membrane that lines the cavity, or lumen of the organ. It consists primarily of a surface epithelium, plus a small amount of connective tissue (lamina propria) and a scanty smooth muscle layer. 2. The submucosa is found just beneath the mucosa. It is a soft connective tissue layer containing blood vessels, nerve endings, mucosa-associated lymphoid tissue, and lymphatic vessels. 3. The muscularis externa is a muscle layer typically made up of an inner circular layer and an outer longitudinal layer of smooth muscle cells. 4. The serosa is the outermost layer of the wall. It consists of a single layer of flat, serous fluidproducing cells, the visceral peritoneum. The visceral peritoneum is continuous with the slick, slippery parietal peritoneum, which lines the abdominopelvic cavity by way of a membrane extension, the mesentery. P a g e 3 | 11 When the peritoneum is infected, a condition called peritonitis, the peritoneal membranes tend to stick together around the infection site. This helps to seal off and localize many intraperitoneal infections (at least initially) providing time for macrophages in the lymphatic tissue to mount an attack. The alimentary canal wall contains 2 important intrinsic nerve plexuses: 1. Submucosal nerve plexus 2. Myenteric nerve plexus These networks of nerve fibres are actually part of the autonomic nervous system. They help regulate the mobility and secretory activity of GI tract organs. STOMACH The J-shaped stomach is on the left side of the abdominal cavity, nearly hidden by the liver and diaphragm. Different regions of the stomach have been named: the cardiac region (named for its position near the heart) surrounds the cardioesophageal sphincter through which food enters the stomach from the oesophagus. The fundus is the expanded part of the stomach lateral to the cardiac region. The body is the midportion, and as it narrows inferiorly, it becomes the pyloric antrum, and then the funnel shaped pylorus, the terminal part of the stomach. The pylorus is continuous with the small intestine through the pyloric sphincter or valve. P a g e 4 | 11 Stomach varies from 15 to 25cm (6-10”) in length. But diameter and volume depend on how much food it contains, can hold about 4 litres (1 gallon) of food. When empty it collapses inward on itself, and its mucosa is thrown into large folds called rugae. The stomach act as a temporary storage tank for food as well as a site for food breakdown. The stomach has longitudinal, circular and oblique muscle layers which not only move food along the tract but also to churn, mix, pummel the food and physically breaking it down to smaller fragments. The mucosa of the stomach is composed many cells: 1. mucus cells - produce bicarbonate rich alkaline to protect stomach wall from being damaged by acid and digested by enzymes. 2. Chief cells – produce protein digesting enzymes called pepsinogen. 3. Parietal cells –produce hydrochloric acid, making stomach contents acidic and activates enzyme for conversion of pepsinogen to pepsin by HCL. The smooth lining of stomach has million deep gastric pits leading into gastric glands secreting gastric juice. After food has been processed in the stomach, it resembles heavy cream called chyme. The convex lateral surface of stomach is the greater curvature and concave medial surface is the lesser curvature. A double layer of peritoneum extends from the liver to the lesser curvature known as the lesser omentum. Another extension of peritoneum drapes downward and covers the abdominal organs like a lacy apron before attaching to the posterior body wall called greater omentum. The greater omentum is riddled with fat, which helps to insulate, cushion and protect the abdominal organs and has large collections of lymphoid follicles containing macrophages and defensive cells of the immune system. P a g e 5 | 11 SMALL INTESTINE The small intestine is a muscular tube extending from pyloric sphincter to the large intestine. The longest section of alimentary tube, an average length of 2 to 4m (7 to 13 feet). The small intestine has three subdivisions: 1. Duodenum 2. Jejunum 3. Ileum Ileum meets large intestine at ileocecal valve which joins them. The small intestine is able to process only small amount of food. The pyloric sphincter controls food movement into the small intestine from the stomach from being overwhelmed. The duodenum joins with the pancreatic and bile ducts to form hepatopancreatic ampulla. The wall of the small intestine has 3 structures that allow food absorption: 1. Microvilli 2. Villi 3. Circular folds Microvilli –tiny projections of plasma membrane giving cell surface fuzzy appearance referred as brush border, producing enzymes that complete protein and carbohydrates digestion in the small intestine. Villi –finger like projections giving velvety appearance. Within each villus, is a rich capillary bed and lymphatic capillary called lacteal, where foods are absorbed. LARGE INTESTINE The large intestine is much longer in diameter than the small intestine, but shorter in length. About 1.5m (5 feet) long, extending from ileocecal valve to the anus. It absorbs water and dry out digestible food and eliminate the residues from body as feces. It frames small intestine on 3 sides and has subdivisions: 1. Cecum –saclike, 1st part of large intestine. 2. Appendix –hanging from cecum, wormlike. 3. Colon –ascending, transverse, descending and sigmoid colon. 4. Rectum –Sigmoid colon join the rectum and anal canal. 5. Anal canal –ends at anus that open to exterior. It has internal anal sphincter(involuntary) external anal sphincter (voluntary). Ordinarily the sphincters closed except during defecation. Anal mucosa produces alkaline mucus that act as lubricant to ease passage of feces. P a g e 6 | 11 THE ACCESSORY ORGANS TEETH The teeth tear and grind the food, breaking it down into smaller fragments by mastication or chewing. By age 21 two sets of teeth have been formed: 1. Deciduous teeth or baby/milk teeth –begin to erupt at 6 months. Full set (20 teeth) complete by the age of 2 years. 1st teeth to appear, lower central incisors. 2. Permanent Teeth as it enlarged and develop, roots of milk teeth are reabsorbed. Between ages 6 –12 years the teeth loosen and fall out. All permanent teeth erupt by end of adolescence, except 3rdmolars, the wisdom teeth that emerge between ages 17 and 25, but sometimes fail to erupt at all. Complete full set of permanent teeth are 32. Teeth are classified according to the shape and function: Incisors –chisel shaped, adapted for cutting Canines –fanglike for tearing and piercing Premolar and Molars –broad crowns with rounded cusps (tips) best suited for grinding. Teeth consist of 2 major regions the crown and root. Both connected by the neck. The exposed part of the tooth above gingiva or gum is the enamel. Enamel is the hardest substance in the body, is fairly brittle because its heavily mineralized with calcium salt. The outer surface of the root is covered by a substance called cement, which attaches the tooth to the periodontal membrane(ligament). The ligament holds the tooth in place in the bony jaw. Dentine, a bonelike material underlies the enamel and forms the bulk of the tooth. The dentine surrounds the pulp cavity, containing number of structures, collectively called pulp. Pulp supplies nutrients to the tooth tissues and provides for tooth sensations. SALIVARY GLANDS There are 3 pairs of salivary glands: Parotid glands –lie anterior to the ears. Inflammation of parotid glands can cause Mumps, a common childhood disease. Submandibular glands and Sublingual glands –empty their secretions into the floor of the mouth, through tiny ducts. The product of salivary glands, saliva is a mixture of mucus and serous fluids which helps to moisten and binds food together into a mass called bolus, so that chewing and swallowing will be easier. Saliva contains the enzyme salivary amylase for digestion of starch in the mouth. Saliva also contains lysozyme and antibodies that inhibit bacteria. Saliva dissolves food chemicals so they can be tasted. P a g e 7 | 11 PANCREAS Pancreas is a soft pink, triangular gland that extends across the abdomen from the spleen to the duodenum. The function of Pancreas is to produce pancreatic enzymes, secreted into the duodenum in an alkaline fluid that neutralizes the acidic chyme. Pancreas produce the hormones insulin and glucagon. LIVER & GALL BLADDER Liver is the largest gland in the body, suspended from the diaphragm and abdominal wall by a delicate mesentery cord, falciform ligament. Liver produces bile which leaves the liver through the common hepatic duct and enters duodenum through the bile duct. Bile is a yellowish to green, watery solution containing bile salts, bile pigments (bilirubin, a breakdown product of hemoglobin), cholesterol, phospholipids and a variety of electrolytes. Bile does not contain enzymes, but its bile salts emulsify fats by breaking large fat globules into smaller ones, for fat-digesting enzymes to work on. Gall bladder is a small, thin walled green sac that snuggles in a shallow fossa in the inferior surface of the liver. When food digestion is not occurring, bile backs up the cystic duct and enters the gall bladder. Function of gallbladder; Gallbladder stores bile and causes bile to be concentrated by removing the water. When fatty food enters the duodenum, a hormonal stimulus prompts the gallbladder to contract and spurt out stored bile making it available to the duodenum. FUNCTIONS OF THE DIGESTIVE SYSTEM The essential activities of the Gastrointestinal (GI) tract include the following 6 processes: 1. Ingestion 2. Food breakdown: mechanical digestion 3. Food breakdown: chemical digestion 4. Propulsion 5. Absorption 6. Defecation P a g e 8 | 11 What is INGESTION Food must be placed into the mouth before it can be acted on. This is an active, voluntary process called ingestion. MECHANICAL & CHEMICAL DIGESTION Once food is in the mouth, both mechanical and chemical digestion begin to break down the food through chewing and mixing with saliva. What is Mechanical digestion: Mechanical digestion prepares food for further degradation through chewing. The food is physically fragment into smaller particles. Degradation is carried out by the enzymes. What is chemical digestion? The sequence of steps in which large food molecules are broken down to their building blocks by enzymes which are protein molecules that act as catalyst. These reactions are called hydrolysis reactions because a water molecule is added to each bond to be broken. Water is also necessary as a dissolving medium and a softening agent for food digestion. The salivary amylase begins chemical digestion of starch breaking it down into maltose. (Note: Chewing bread longer before swallowing will make it taste sweeter as sugars are released). Saliva is secreted continuously to keep the mouth moist, but as food enters the mouth, larger amounts of saliva pour out. Some stimuli can make the mouth watery due to parasympathetic fibres in cranial nerves. What is PROPULSION The action of pushing forward to the next part. Because food must be processed by more than one digestive organs, hence it must be propelled from one organ to the next. In order to move the food from the mouth to the organs internally, swallowing (deglutition) has to take place. Swallowing is a complex process involving the coordinated activity of several structures Tongue soft palate pharynx and oesophagus. Deglutition or swallowing depend largely on propulsive process called peristalsis for food movement. Peristalsis is involuntary and involves alternating waves of contraction and relaxation of muscles in the organ wall. The effect is to squeeze the food along the tract. Involve 2 phases of swallowing: 1. The voluntary buccal phase. 2. The involuntary pharyngeal oesophageal phase. What is buccal phase? The voluntary phase that occurs in the mouth. Once the food has been chewed and well mixed with saliva it becomes a bolus or food mass and forced into the pharynx by the tongue. As food enters the pharynx it passes out of our control and into the realm of reflex activity. What is pharyngeal oesopharyngeal phase? The involuntary phase that transports food through the pharynx and oesophagus. The Vagus nerves controls this phase and promotes the mobility of digestive organs from this point on. Food is moved through the pharynx and then into the oesophagus below by wavelike peristaltic contractions of their muscular wall, first the longitudinal muscles contract and then the circular muscles contract. As food enters, the tongue blocks off the mouth, soft palate closes off the nasal passages, larynx rises and covered with epiglottis. If we try to talk while swallowing, food may enter the respiratory passages which can trigger a protective reflex-coughing-during which air rushes upward from the lungs in an attempt to expel the food. P a g e 9 | 11 Food moved through the pharynx by peristalsis, an involuntary alternating wave of contraction and relaxation of the muscles in the organ wall. The net effect is to squeeze the food along the tract. The pharynx and oesophagus have no digestive function as they only provide passageways to carry food to the next processing site, the stomach. Once food reaches distal end oesophagus, it presses against the cardioesophageal sphincter, causing it to open and the food enters the stomach. Sometimes cardioesophageal sphincter fails to close tightly and gastric juice from the stomach backs up into the oesophagus resulting in a characteristic pain known as heartburn. Activities of the stomach As food enters and fills the stomach, its wall begins to stretch, at the same time gastric juices are secreted. The muscles of stomach walls compress and pummel the food, breaking it apart physically and continuously mixing the food with enzyme-containing gastric juice so that semifluid chyme is formed. Little chemical digestion occurs in the stomach. Chemical digestion involves sequence of steps, where large food molecules are broken down to their building blocks by enzymes. Protein are digested to their building blocks, which are amino acids. The products of protein digestion are polypeptides and peptides. When food has been well mixed, a rippling peristalsis begins in the upper half of the stomach and the contractions increase in force as the food approaches the pyloric valve. The pylorus of the stomach holds about 30mls of chyme. Because the pyloric sphincter barely opens, each contraction of the stomach muscle squirts 3mls or less of chyme into the small intestine. The contraction also closes the valve, so the rest (about 27mls) is propelled backward into the stomach for more mixing, a process called retropulsion. Generally, it takes about 4 hours for the stomach to empty completely after the person eats and about 6hrs or more if the meal has a high fat content. How vomiting may occur Local irritation of stomach from bacterial food poisoning may activate emetic center in the brain causing vomiting. Vomiting is due to contraction of abdominal muscles and diaphragm and increase pressure in the abdominal organs. The emetic centre may also be activated through disturbance of the equilibrium apparatus of the inner ear when a person spins for a long period going on a boat ride on the rough water. What is ABSORPTION The digestive end products are transported from the lumen of the gastrointestinal tract to the blood or lymph. For absorption to occur, the digested foods must first enter the mucosal cells by active or passive transport processes. The small intestine is the major absorptive site. Absorption -activities of the small intestine Chemical food digestion is accelerated in the small intestine as the food takes a rather wild 3-6 hours journey through the looping coils and twists. The small intestine is the major absorption site of water and end products of digestion. When chyme enters small intestine, secretin and cholecystokinin hormones influence the release of pancreatic juice from pancreas and bile from liver. If either bile or pancreatic juice are absent, no fat digestion or absorption goes on, causing fatty bulky stools. Most substances are absorbed through the intestinal cell plasma membranes by the process of active transport. P a g e 10 | 11 They enter the capillary beds in the villi to be transported in the blood to the liver via hepatic portal vein except lipids or fats that are absorbed by the process diffusion. Lipid breakdown products enter capillary beds and lacteals in villi and are carried to liver by blood and lymphatic fluids. At the end of ileum, all that remains is some water, indigestible food materials (plant fibres such as cellulose) and large amounts of bacteria. Cellulose is important because it provides fibre which is important for moving faeces along the colon and ease the action of defecation. This debris enters large intestine through ileocecal valve by peristalsis with rhythmic segmental movements produce by local constrictions of the intestine. What is DEFECATION This is the elimination of indigestible residues from the gastrointestinal tract via the anus in the form of faeces. Mass movements are long, slow moving but powerful contractile waves force the contents toward the rectum. Activities of the large intestine Large intestine does not produce digestive enzymes. It aids with defecation. What is finally delivered to the large intestine contains few nutrients, but that residue still has 12 to 24 hours more to spend there. The resident bacteria that live in the lumen of the colon, metabolize some of the remaining nutrients, releasing gases (methane and hydrogen sulphide) that contribute to odor of feces. About 500mls of gas (flatus) is produced each day and much more when certain carbohydrate rich foods (such as beans) are eaten. Feces, the more or less solid product delivered to the rectum, contain undigested food residues, mucus, millions of bacteria and just enough water to allow their smooth passage. When there is food residue, the colon begins contractions which are quite slow, known as the haustral contractions. This is a segmenting movement lasting about 1 min, that occur every 30mins or so. Bulk or fiber in the diet increases the strength of colon contractions and soften stools allowing colon to act as a well-oiled machine. As feces are forced through anal canal, messages reach the brain giving us time to decide whether external voluntary sphincter should open or constricted to stop passage of feces. Defecation can be delayed temporarily and with the next mass movement, defecation reflex is initiated again. Watery stools or diarrhoea occur as a result from irritation of the colon by bacteria or any condition that rushes food residue through large intestine before the organ has sufficient time to absorb the water. Because fluids and ions are lost from the body, prolonged diarrhoea may result in dehydration and electrolyte imbalance and if severe can be fatal. However, constipation may occur if there is a lack of fiber in the diet, poor bowel habits and laxative abuse, where feces remain in large intestine for extended period, water is absorbed, stool becomes hard and difficult to pass. P a g e 11 | 11