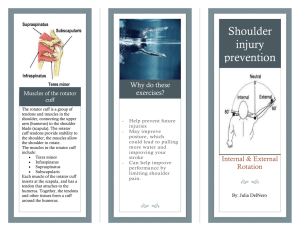
Dr. RAGHAVENDRA RAJU INTRODUCTION In 1834, Smith - first description of a rupture of the rotator cuff tendon . Among most common causes of shoulder pain and instability. Incidence 5-40% with increasing with advancing age ( >40 years). Normal senescence process ANATOMY- ROTATOR CUFF Made up of 4 interrelated muscles arising from the scapula and attaching to the tuberosities of humerus. supraspinatus infraspinatus teres minor subscapularis Long head of biceps – functional part ROTATOR CUFF MUCLES BIG BALL AND SMALL SOCKET JOINT Function of rotator cuff The rotator cuff is the Dynamic stabilizer of the glenohumeral joint. Normal function of the shoulder is a balance between mobility and stability. Function of rotator cuff Stabilisers of shoulder mainly anterior and posterior cuff providing fixed fulcrum for concentric rotation of the humeral head. Neutralises shearing forces of deltoid in early abduction. Initiation of abduction. Rotation of shoulder. ETIOLOGY IMPINGEMENT( MC ) TRAUMA ATTRITION - AGING ISCHEMIC TENDON LACK OF NUTRITION TO JOINT IATROGENIC Different shapes of acromia (Biglianni et al) -anterior slope Type 1 - Flat ( 3 % of cuff tears) Type 2 - Curved (24 % of cuff tears) Type 3 - Hooked ( 73 % of cuff tears) PATHOLOGY Torn Rotator Cuff Can not Counterbalance the upward pull of the deltoid on the humerus Not able to Hold the head of the humerus secure in the glenoid AHD <6mm Leads to abutement of humeral head against acromion Acetabulization: Concave deformity of under surface of Acromion Narrowing & Arthritis of Gleno-Humeral Joint Last stage of Cuff tear arthropathy with collapse of humerus head Hamada and Fukuda Stages of Cuff Arthropathy CLASSIFICATION DURATION – ACUTE OR CHRONIC 2. DEGREE OF TEAR- PARTIAL OR FULL THICKNESS TEAR. 3. ETIOLOGY- TRAUMATIC OR DEGENERATIVE. 4. COFIELD – BASED ON SIZE OF TEAR 1. SIZE OF TEAR DEGREE <1 cm SMALL 1- 3 cms MEDIUM 3-5cms LARGE >5 cms MASSIVE ELLMANS CLASSIFICATION 1.ARTICULAR 2.BURSAL 3.INTERSTITIAL Crescent Trapezoidal Reverse ‘L’ Full Thickness Tear ‘L’ Shaped Massive tear SYMPTOMS Pain on the lateral aspect of the shoulder may radiate to deltoid insertion anterior (acromion )with impingement +/- biceps tendonitis Stiffness Cannot lie affected side. Weakness, instability, crepitus. Assessing shoulder pain Components of the assessment include Focused history physical examination Tests/studies 21 Focused History Questions Onset of Pain When symptoms started* History of trauma/injury 23 Focused History Questions Mechanism of Injury Helps predict injured structure Example: Fall directly onto anterior/superior shoulderAC joint injury (shoulder separation) Example: Arm forcefully abducted and externally rotated subluxation or anterior dislocation Example: If chronic pain, note activity that triggers pain, such as the cocking phase of throwing or the pull-through phase of swimming 24 Focused History Questions Mechanism of Injury, continued Can determine radiological needs Likelihood of specific conditions varies Setting (work, recreation, sports, traumatic, atraumatic) Age of the patient* 25 Focused History Questions Location of pain* Anterior Lateral Superior Posterior Radiation of pain Rotator cuff problems often include pain radiating to upper arm If pain starts in neck and radiates to shoulder, consider cervical spine disease 26 Focused History Questions Consider sources of referred pain Cervical spine – spondylolysis, arthritis, disc disease Cardiac - myocardial ischemia Diaphragmatic irritation Thoracic outlet syndrome Gallbladder disease Complex regional pain syndrome (a.k.a, reflex sympathetic dystrophy) 28 Focused History Questions Characteristics of pain Night pain when lying on affected Rotator cuff tear side, muscle atrophy < 30 yo Biomechanical, inflammatory > 45 yo, Hx of trauma Rotator cuff tear - 35% of pts Painful arc (60-120°abduction) Pain > 120° abduction Catching, popping, clicking Subacromial impingement Acromioclavicular joint GH or AC joint arthritis, labral tear 29 Focused History Questions History of instability Glenohumeral subluxation or dislocation Aggravating factors Overhead work, repetitive movements, sports Relieving factors/treatments tried Rest, immobility, medications, other treatments History of Prior Shoulder Problems or Surgeries 30 Physical Exam - General Develop a standard routine protocol. Alleviate the patient's fears. Adequate exposure. Compare shoulders. 31 Physical Exam – Steps Inspection Palpation Range of motion (ROM) Strength testing Special tests 32 Inspection Swelling, asymmetry, muscle atrophy, scars, ecchymosis and any venous distention Note posture Deformities Scapular "winging" Atrophy - supraspinatus or infraspinatus - consider rotator cuff tear, suprascapular nerve entrapment or neuropathy. 33 Palpation Sternoclavicular joint Clavicle Acromioclavicular joint Subacromial bursa Coracoid process Bicipital groove Greater tuberosity Lesser tuberosity Scapula (spinatus muscles) 34 Palpation of AC Joint Patient's arm at his/her side Note swelling, pain, and gapping. 35 Palpation of Bicipital Groove Patient sitting, beginning with the arm straight Patient actively flexes biceps muscle while examiner provides supination and ER Examiner palpates the bicipital groove for pain 36 Range of Motion (ROM) Evaluate active ROM If movement limited by pain, weakness, or tightness, assist passively Lack of full ROM with active and passive exam is found in adhesive capsulitis and arthropathy Evaluate bilaterally for comparison 37 FLEXION( 180) EXTENSION( 4O) ABDUCTION(180) ADDUCTION EXTERNAL ROTATION(55) INTERNAL ROTATION(45) Apley scratch test for ER/IR External rotation and abduction Reach for upper scapula Compare bilaterally – note level reached Internal rotation and adduction Reach for lower scapula Compare bilaterally – note level reached NEER’S SIGN Patient seated with arm at side, palm down (pronated) Examiner standing Examiner stabilizes scapula and raises the arm (between flexion and abduction) Positive test = pain NEERS’ TEST Most diagnostic test LA 10ml lignocaine into subacromial bursa >50% relief – rotator cuff tendinitis or partial tear of bursal surface. Pain relief but weakness persists – full thickness tears No relief - incorrect diagnosis or wrong injection Hawkins Test Patient standing Examiner forward flexes shoulder to 90°, then forcibly internally rotates the arm Positive test = pain in area of superior GH joint or AC joint Sensitivity/Specificity Neer Impingement Sensitivity: 72% Specificity: 60% Hawkins-Kennedy Impingement Sensitivity: 79% Specificity: 59% Hegedus. British J Sports Med, 2012. JOBS TEST OR EMPTY CAN TEST Jobe s isolation test or empty can test. The patient is positioned sitting with arms straight out, elbows locked, thumbs down, and arm at 30 degrees (in scapular plane). The patient should attempt to abduct his arms against the examiner's resistance. Drop Arm Test Method: patient abducts (or examiner passively abducts) arm and then slowly lowers it May be able to lower arm slowly to 90° (deltoid function) Arm will then drop to side if rotator cuff tear Positive test: patient unable to lower arm further with control If able to hold at 90º, pressure on wrist will cause arm to fall DROP SIGN The affected arm is held at 90 degrees of elevation in the scapular plane and at almost full external rotation with the elbow flexed at 90 degrees. The patient is asked to maintain this position actively as the examiner releases the wrist while supporting the elbow LIFT OFF TEST The Gerber lift-off test The shoulder is placed passively in internal rotation and slight extension by placing the hand 5-10 cm from the back with the palm facing outward and the elbow flexed at 90°. The test is positive when the patient cannot hold this position, with the back of the hand hitting the patient's back. BELLY PRESS TEST patient presses the abdomen with the flat of the hand and attempts to keep the arm in maximal internal rotation. OTHER TESTS EXTERNAL ROTATION LAG SIGN- SUPRASPINATUS AND INFRASPINATUS. EXTERNAL ROTATION STRESS TESTINFRASPINATUS AND TERES MINOR. Hegedus. British J Sports Med, 2012 Cochrane Database Review 2013 – Hanchard, et al. Physical tests for shoulder impingements and local lesions of bursa, tendon or labrum that may accompany impingement. 33 studies involving 4002 shoulders Cochrane Database Review 2013 – Hanchard, et al. There is insufficient evidence upon which to base selection of physical tests for shoulder impingements, and local lesions of bursa, tendon or labrum that may accompany impingement, in primary care. The large body of literature revealed extreme diversity in the performance and interpretation of tests, which hinders synthesis of the evidence and/or clinical applicability. INVESTIGATIONS X RAY USG CT SCAN MRI X RAY AP VIEW AXILLARY LATERAL VIEW SUPRASPINATUS OUTLET VIEW X RAY AP VIEW – ER AND IR VIEWS The internal rotation view is for detecting Hill-Sachs lesions, and external rotation for the greater tuberosity and proximal humeral physis in skeletally immature patients. A true anteroposterior radiograph of the glenohumeral joint is forarticular cartilage of the glenoid and the humeral head. AXILLARY VIEW the anatomy of the glenoid rim, the acromion, the coracoid, and the proximal humerus. SUPRASPINATUS OUTLET VIEW Ultrasound Cheap and quick to perform. Good definition of rotator cuff. Allows dynamic examination. Operator dependant. Findings: Nonvisualization of cuff Localized absence Discontinuity Focal abnormal echogenicity MRI Best diagnostic aid. Defines site of cuff damage. Demonstrates fatty changes in muscle -poor quality cuff. Exact size, shape and location of tear Non-invasive MRI Normal cuff Full thickness tear TREATMENT SEVERITY OF SYMPTOMS. AGE. ACTIVITY LEVEL. PATIENT REQUIREMENTS . Conservative management McLaughlin in 1962 advanced reasons to avoid early repair 25 % of cadavers had torn cuff -most of them were asymptomatic 50 % of patients would recover comfortably Results of early and late repair are similar Repair did not always permit anatomic restoration Early diagnosis is difficult NATURAL HISTORY IS UNPREDICTABLE Review of literature indicates that success rate of nonoperative treatment ranges from 33% to 92% Bartolozzi et al (Clin orthop, 1994) reported 66- 75% good or excellent results (mean follow up 20 months). Unfavorable prognostic factors were Tear> 1 cm2 Symptoms > 1yr Significant functional impairment REST ACTIVITY MODIFICATION NSAIDS PHYSIOTHERAPHY (streching and strenghtening exercises). INJECTION THERAPHY ( STEROID AND PRp) Orthotherapy Term used by Michael Wirth (OCNA 1997) Interactive exchange between patient and orthopedic surgeon directed at creating exercise regimen that gradually improves motion and strength in shoulder girdle. Three phases: Phase 1- restore full, painless range of motion. Codman pendulum exercise followed by passive movements in all direction Phase 2- designed to strengthened remaining muscles of rotator cuff, deltoid & scapular muscles Phase 3- gradual reinstitution of normal activities including work, hobby and sport. OPERATIVE TREATMENT ONLY IF CONSERVATIVE TREATMENT FAILS. (ATLEAST 6 WEEKS) Operative treatment Patient selection: Samilson & Binder : Patient physiologically younger than 60 yrs Clinically or arthrographically demonstrable full thickness cuff tear. Failure to improve on nonoperative management for minimum of 6 weeks Need to use shoulder in overhead elevation Full passive range of motion Ability & willingness to cooperate Poor prognostic factors Old age group (physiological age >60 years) Long history No history of trauma Smoker Multiple steroid injection Diffuse osteopenia Grade 3 or less of external rotation Upward migration of humeral head. Procedures Repair of tear open or arthroscopic Tendon to tendon or tendon to bone Arthroscopic debridement,SAD and acromioplasty with mini-open repair. Technique of open repair Approach- 5 to 7 cm incision extending from lateral aspect of ant third of acromion to lateral tip of coracoid Rotator cuff repair: Assess the nature of tear Mobilisation – Release of adhesion Release of coracohumeral ligament Interval slide Subscapularis tendon transfer Repair – tendon to tendon or tendon to bone(McLaughlin technique) Mobilisation Release of capsule from labrum Release of cuff tendons from coracoid Transosseous repair Advantages of open repair Easy to do No special equipment required Allows direct visualization of cuff repair and acromioplasty Good long term follow-up Disadvantages Deltoid detachment required False positive studies (arthrogram 2%, MRI 10%) will lead to unnecessary open exploration Unrepairable tear will be opened. Significant intraarticular pathology will be missed Arthroscopic repair of rotator cuff Advantages : Lesser morbidity Ability to identify and treat other pathology Truly outpatient Allows to address small undetected tears Patient acceptance Disadvantages : Technically difficult Implant cost-needs anchor Increased OR time High failure rate during learning curve Arthroscopic assisted mini open repair Lateral portal is expanded Useful for small & moderate shape tears Results comparable to open repair Post operative plan. Arthroscopic Immd active and passive ROM Avoid active abduction >60 degree for 3-4 wks Then electrical stimulation, resisting exercises for 3-4 mths High demand activities within 4-6 mths Open Proceed slowly (deltoid detached) Avoid active flexion or abduction for 4 wks Requires 1-2 additional months Partial thickness tear Surgical options: Debridement alone Debridement with arthroscopic subacromial decompression Open repair with acromioplasty Arthroscopic repair Arthroscopic subacromial decompression with mini open repair Partial thickness tear Before and after debridement Removal of inferior part of anterolateral acromion Arthroscopic SAD Open SAD Arthroscopic • No morbidity • Genuine benefit Arthroscopic rotator cuff repair Irreparable tears Pre operative diagnosis AHI <3 mms Profound loss of external rotation MRI-fatty degeneration of muscle Treatment options Debridement Tendon transposition Subscapularis Infraspinatus Muscle transfer Partial repair Allograft substitution COMPLICATIONS PROGRESSION OF LESION ROTATOR CUFF ARTHROPATHY LONG HEAD OF BICEPS TENDON RUPTURE ANTEROPOSTERIOR INSTABILITY Cuff tear arthropathy Radiograph: Superior translation of head of humerus Loss of articular cartilage Direct articulation of head with coracoacromial arch “acetabularization” of upper glenoid Treatment Intractable pain unresponsive to conservative treatment is the strongest indication for surgery Options : Shoulder arthrodesis Hemi replacement arthroplasty Total shoulder replacement Treatment (contd) Prerequisites for arthroplasty: Adequate deltoid power Preserved or reconstructed coracoacromial arch Conclusion Diagnosis is usually by good history and examination Non operative management remains the standard initial care Surgery in selective active individuals Arthroscopy - early mobilization and decreased morbidity Treatment according to patients functional needs