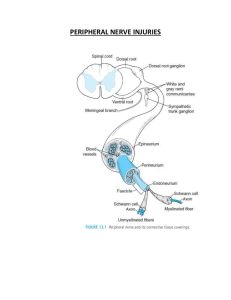
Lip Teh Page 1 5-Feb-20 BRACHIAL PLEXUS INJURIES Sources: CME Oct 00, Nov 00 CME Apr 04 HISTORY Smellie (1768) described obstetrical brachial plexus palsy Flaubert ( 1827) - Anatomic findings of avulsed nerves following trauma Duchenne (1872) - first systematic anatomic delineation of the muscle paralysis resulting from birth trauma Erb (1874) - localized the lesion to upper cervical roots with electrical stimulation Seeligmuller and Klumpke - further defined a subset of brachial plexus injuries involving the lower cervical roots known as Klumpke’s palsy William Thornburn(1900) - first report of successful surgery on an adult traction injury Kennedy (1903) - attempts to resect proximal plexus neuromas and to perform primary suture repair Fairbank (1913) – advocated muscle release to offset the characteristic internal rotation and adduction features. Wyeth and Sharp(1917); and Taylor(1920)- performed large series of primary nerve reconstructions on infants and claimed favorable results for early repair. Sever (1925) and Jepson (1930) - limited long-term success with early brachial plexus repair associated with high perioperative morbidity and mortality rates. Sedon (1947) - advised against primary brachial plexus reconstruction. 1930s-1970s – development of novel muscle transfers Millesi (1973); Gilbert (1980) - began reporting good results with early surgical intervention with nerve grafts in obstetric brachial plexus cases. Allieu (1982), Celli (1978), and Narakas(1980) - technique of extraplexal neurotization from accessory and intercostal nerves for severe avulsion injuries. Gu (1996, 1998) - phrenic nerve and contralateral C7 nerve transfers for specific plexus lesions. Ikuta (1980), Taylor and Ham(1976), and Berger and Becker (1994)- free muscle transfers and vascularized nerve grafts CLASSIFICATION Millesi Classification I Supraganglionic II Infraganglionic III Trunk IV Cord Lip Teh Page 2 5-Feb-20 Leffert Classification of Brachial Plexus Injuries I Open (usually from stabbing) II Closed (usually from motorcycle accident) IIa Supraclavicular - preganglionic: - avulsion of nerve roots, usually from high speed injuries with other injuries and LOC; - no proximal stump, no neuroma formation (neg Tinel's) - pseudomeningocele, denervation of neck muscles are common - horner's sign (ptosis, miosis, anhydrosis) - postgangionic: - roots remain intact; - usually from traction injuries; - there are proximal stump and neuroma formation (pos Tinel's) - deep dorsal neck muscles are intact, and pseudomeningocele will not develop; IIb Infraclavicular Lesion: - usually involves branches from the trunks (supraclavicular); - function is affected based on trunk involved; Trunk Injured Upper Middle Lower Functional Loss biceps , shoulder muscles Wrist and Finger Extension Wrist and Finger Flexion III Radiation induced IV Obstetric IVa Erb's (upper root) - waiter's tip hand; Arm adducted and internally rotated with the elbow extended, forearm pronated, wrist flexed, and the hand in a fist. IVb Klumpke (lower root); Arm supinated with the elbow bent and wrist extended. Four Patterns of Closed Injuries I Upper plexus palsy (Erb’s palsy in the OBPI cases) involves C5-C6 +/- C7roots. II Lower plexus palsy (Klumpke’s palsy) involves C8-T1 roots (and sometimes also C7) III Total plexus lesions involve all nerve roots C5-T1 IV Intermediate type that primarily involves the C7 root. Lip Teh Page 3 5-Feb-20 EPIDEMIOLOGY 0.38 to 2.6 per thousand term births Risk factors 1) gestational diabetes (odds ratio 1.9) 2) forceps delivery (3.4), 3) vacuum extraction (2.7) 4) shoulder dystocia (76.1) 5) intrauterine pressure a. high pressures exerted between the brachial plexus and maternal pelvis with labor 6) breech delivery a. vertex presentation (95%), breech (2%), ceasarian 1% 7) multiparity 8) macrosomia, 9) history of a previous child with brachial plexus injury Frequencies: o Erbs (73%), Total Plexus (25%), Klumpke’s (2%) o Right > Left o 4% bilateral (correlated with breech) Nerve Injuries Seddon Classification (1943): Neurapraxia o This is the least severe injury - a localized conduction block of the nerve. It can be o caused by streching or compression of the nerve. The axons inside the nerve remain intact, but there may be segmental demyelination of the nerve. Because there is no terminal structural damage to the nerve, this type of injury usually recovers quite quickly. Axonotmesis o The sheath of the nerve remains intact, but there is axonal disruption. The axons o can regenerate, and near to complete recovery can be expected in the injuries where the motor targets are close enough. Neurotmesis o This is an injury where the nerve has been ruptured. There will be no or very little recovery without surgical intervention. Neuroma-in-continuity: In some cases, the nerve has begun to rupture, but the rupture is incomplete. In such cases, the nerve can develop a neuroma Lip Teh Page 4 5-Feb-20 The most severe type of injury is an avulsion, in which the nerve root has been torn out of the spinal cord. Pathogenesis Excessive lateral cervical flexion at delivery creates a gradient of increasing traction from upper to lower cervical roots Lower roots 4x more likely than upper roots to avulse. Upper roots more likely to rupture(88%) than avulse. o Roots of C5 and C6 are anchored to the transverse process by a dense fibrous sheath and gives them more protection from avulsion. o Lower roots do not have this attachment, weakest point (elastic limit) is the point at which the roots leave the spine o The degree of injury is inversely proportional to the length of the nerve – the elastic limit of a short nerve is more quickly exceeded compared to a longer nerve. C5 and C6 injuries are more common as they are shorter nerves. o poorer return of function in conservatively managed lower root injury versus similarly managed upper root injury. In breech deliveries, upper roots also tend to be avulsed Classification of Severity Medical Research Council Scale M0 - No contraction M1 - Flicker contraction M2 - Muscle contraction with active motion with gravity eliminated M3 - Full range of motion against gravity M4 - Full range of motion against gravity with some resistance M5 - Full range of motion against gravity with maximum resistance for that muscle Active Movement Scale (Clarke and Curtis) Based on overall joint motion rather than individual muscle testing – thus more useful in pediatrics The 7-point scale ranges from no contraction to full motion with gravity eliminated and against gravity. Motions assessed include shoulder flexion, abduction, adduction, internal rotation, and external rotation; elbow flexion and extension; wrist flexion and extension; and finger flexion and extension. Gravity Eliminated No contraction Contraction, no motion Motion <= ½ Motion >= ½ Full Motion 0 1 2 3 4 Lip Teh Against Gravity Motion <= ½ Motion >= ½ Full Motion Page 5 5-Feb-20 5 6 7 Mallet Classification Grade 0-5 scale based on voluntary upper extremity movements, including active abduction, external rotation, hand to nape of neck, hand to back, and hand to mouth. Mallet and AMS have both been shown to be most reproducible in OBP MRC scale more useful in adult palsies. Imaging studies Xrays CXR – clavicle, scapular, ribs (intercostals potential source for neurotisation), diaphragm Cervical xrays – fractures of the transverse processes might indicate avulsions of the corresponding roots, due to the attachments of the deep cervical fascia between the cervical roots and the transverse processes Humeral/elbow xrays – potential radial, ulnar, median nerve injuries Ultrasound Lip Teh Page 6 5-Feb-20 In children with a persistent, passively tight, internal rotation contracture of the shoulder to rule out a posterior glenohumeral dislocation. CT/Myelography Accuracy of predictability is not the same for all roots Avulsed roots can exist despite a normal myelogram. However in experienced centres, the reliability is high, enhanced with CT (95% PPV) Better to perform the myelography at least 1 month after the injury to allow for the pseudomeningocele to be sealed and to prevent the dye from flowing freely to the surrounding spaces. MRI Advantage of good visualization of the brachial plexus beyond the spinal foramen. Visualization of intradural portion of the rootlets is difficult due to the insufficient contrast between the subarachnoid space and the neural structures, a problem caused mainly by cerebrospinal fluid pulsatility. Overall sensitivity 81 percent. 50% for root avulsions Electrodiagnostic studies Study of paraspinal muslces help diagonose root avulsions SNAP’s and somatosensory potentials improve the accuracy of the diagnosis o Normal sensory conduction velocities in conjunction with a flail anesthetic arm implies root avulsion, Electromyography (EMG) and nerve conduction studies are less useful for patients with OBPP than they are for adults with brachial plexus injuries. With electromyography, fibrillations are associated with denervation and will become apparent approximately 3-6 weeks following injury. Motor unit potentials suggest reinnervation or collateral sprouting. In general, EMG findings may be misleadingly optimistic. Most surgeons believe that clinical examination is a better prognostic indicator than is EMG. MANAGEMENT 1) Treat life threatening injuries 2) Look for associated Injuries o Clavicular or humeral bone fractures o Phrenic nerve palsy (upper roots) o recurrent laryngeal and facial nerve paralysis o Horner syndrome (lower roots) 3) Assess brachial plexopathy History, Examination Lip Teh Page 7 5-Feb-20 4) Management in a multidisciplinary setting Prognosis Poor prognostic factors: 1. presence of Horners syndrome 2. severe neuropathic pain 3. fractures of the clavicle, cervical transverse processes, or winged scapula 4. Very poor prognosis with scapulothoracic dissociation 5. Lower trunk lesions Indications 1) Maintain Passive range a. Serial followup to look for improvement 2) Criteria for surgery – remains controversial a. Clinical motor testing is the key factor for selecting patients for surgery b. Most use recovery of biceps function as indicator c. More accurate if use recovery of multiple muscle groups rather than just using one. d. Gilbert recommends surgery if biceps recovery is not evident by 3 months, Waters suggests waiting until 4 months, and Strombeck discouraged using deltoid or biceps activity at 3 months as the criterion for surgical intervention and came to the conclusion that children with little or no deltoid and biceps activity at 6-9 months were more appropriate candidates. e. Clarke has developed an active movement scale and scores recovery to determine the need for surgery. At 9 months, the infant is assessed with the cookie test, which requires the child to put a cookie to his or her mouth with limited neck flexion. If the infant does not pass the cookie test, then surgery is recommended. f. Shenaq - global injury that i. does not improve by 3 months of age; ii. lack of motor function of one or more muscle units (elbow flexors, shoulder abductors and external rotators, and wrist and finger flexors) at 3 to 6 months iii. grade I-II muscle units with no progress at 6 months or beyond Results of the spontaneous recovery following obstetrical palsy: Landmark study “thesis of Tassin” / Gilbert et al 44 children followed for 10 years / no surgical intervention Analysis: complete recovery possible if deltoid and biceps M1 by 2nd month Results good but incomplete if recovery of biceps and deltoid by 3-3.5 months Highly unsatisfactory results if biceps not M3 by 5 months With 3 or more root avulsion prioritize 1. external rotation for the shoulder 2. flexion at the elbow 3. extension of the wrist Lip Teh 4. Page 8 flexion of the digits 5-Feb-20