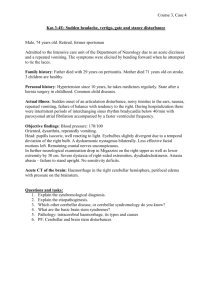
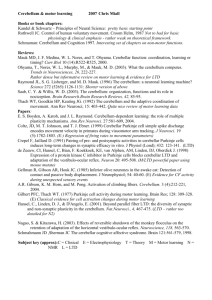
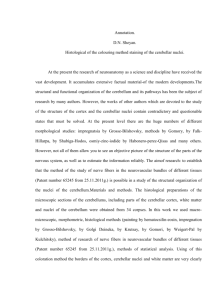
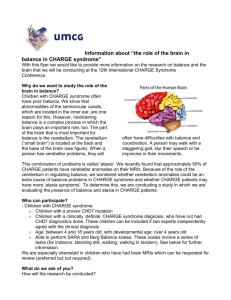
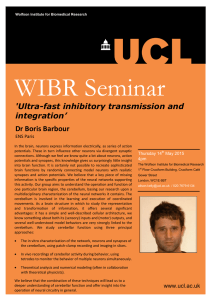
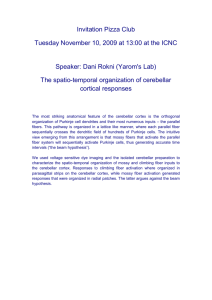
Chapter 16 Cerebellum LEARNING OBJECTIVES ▶ Identify cerebellar peduncles in gross anatomy specimens. Describe the contents of the cerebellar peduncles. ▶ Describe the internal circuitry of the cerebellum. ▶ Describe the etiopathogenesis and clinical features for Arnold–Chiari malformation. ▶ Describe the blood supply of the cerebellum. ▶ Describe the effects of alcohol on the cerebellum. ▶ Describe the effects of lesions in the various functional areas of cerebellum. ▶ Define the types of appendicular ataxias found in cerebellar disorders. ▶ Describe various forms of input to the cerebellum. ▶ Describe the etiopathogenesis and clinical features for Dandy–Walker syndrome. ▶ Describe the connections for the various functional areas of cerebellum. Das and Baugh, Medical Neuroscience Q&A (ISBN 978-1-62623-537-3), copyright © 2019 Thieme Medical Publishers. All rights reserved. Usage subject to terms and conditions of license. 16 Cerebellum 16.1 Questions Easy Medium Hard 3. Which of the following areas contains important communicating fibers from the cerebellum to the thalamus? A. Area A Consider the following image for questions 1 to 3: B. Area B C. Area C D. Area D E. Area E 4. A 56-year-old woman presents with intention tremor. Investigation reveals cerebellar hemorrhage that has affected the immediate input pathway for the deep cerebellar nuclei. Which of the following neurons might have been affected? A. Granule cells within the cerebellum B. Golgi cells C. Stellate cells D. Basket cells E. Purkinje cells Consider the following case for questions 5 and 6: A female newborn presented with flaccid paraplegia of the lower limbs. Neuroimaging revealed Arnold– Chiari (type II Chiari) malformation. 5. Which of the following features might have helped the clinician to diagnose her case? A. Herniation of cerebellar tonsils through foramen magnum B. Herniation of lower medulla through foramen magnum C. Enlarged posterior fossa 1. Which of the following areas contains important inputs from the cerebral cortex to the cerebellum? D. Atresia of foramen of Luschka E. Agenesis of cerebellar vermis A. Area A C. Area C 6. Which of the following additional features is most likely to be present in this case? D. Area D A. Syringomyelia E. Area E B. Myelomeningocele B. Area B C. Normal skull base 2. Which of the following areas contains climbing fibers to the cerebellum? A. Area A D. Normal supratentorial structures E. Hydrocephalus due to adhesions occluding the fourth ventricle B. Area B C. Area C D. Area D E. Area E 142 Das and Baugh, Medical Neuroscience Q&A (ISBN 978-1-62623-537-3), copyright © 2019 Thieme Medical Publishers. All rights reserved. Usage subject to terms and conditions of license. 16.1 Questions Consider the following case for questions 7 and 8: A 48-year-old woman presents with truncal and limb ataxia, and nystagmus. CT scan reveals evidence of hemorrhage in the left interposed and fastigial nuclei. 7. Which of the following vessels is most likely involved? A. AICA B. PICA C. SCA D. Pontine branches of basilar E. Vertebral artery 11. A 60-year-old woman presents with an unsteady wide-based stance and nystagmus. Which of the following is the most likely location of a lesion? A. Superior cerebellar peduncle (SCP) B. Cortex of the paravermal cerebellar area C. Cortex of the posterior cerebellar lobe D. Dentate nucleus E. Flocculonodular lobe Consider the following case for questions 12 and 13: A 69-year-old man is unable to rapidly slap his hand to his knee while alternating pronation and supination of his hand with each movement. 8. To control bleeding from the involved artery, which of the following vessels should be clamped at surgery? 12. Which of the following specifies this particular deficit? A. Internal carotid artery A. Asterixis B. Vertebral artery B. Dysrhythmia C. Rostral part of the basilar artery proximal to its bifurcation C. Dysmetria D. Caudal part of the basilar artery just distal to its formation E. Titubation E. Subclavian artery Consider the following case for questions 9 and 10: A 62-year-old chronic alcoholic presents with truncal instability, uncoordinated gait, and moderate ataxia of his arms. He has consumed alcohol for 40 years, averaging ~90 mL a day. D. Dysdiadochokinesia 13. Which of the following structures is most likely lesioned in this patient? A. Dentate nucleus B. Fastigial nucleus C. Flocculonodular lobe of cerebellum D. Vermal region of cerebellum E. Ventral spinocerebellar tract 9. Which of the following regions might have undergone significant degeneration? B. Superior vermis 14. Which of the following pairs correctly indicates the exclusive source and nature of climbing fibers to the cerebellar cortex? C. Flocculus A. Ipsilateral inferior olivary nuclei, inhibitory D. Paravermal area B. Contralateral inferior olivary nuclei, inhibitory E. Posterior lobe C. Ipsilateral inferior olivary nuclei, excitatory A. Inferior vermis D. Contralateral inferior olivary nuclei, excitatory 10. Which of the following cells will most notably be affected? E. Contralateral pontine nuclei, inhibitory F. Contralateral reticular nuclei, excitatory A. Granule cell B. Golgi cell Consider the following case for questions 15 and 16: C. Stellate cells A 10-year-old female presents with ataxia, mental retardation, and seizures. Examination reveals an enlarged posterior fossa with cystic dilatation of the fourth ventricle. Atresia of foramens of Luschka and Magendie was considered as the probable etiology for her symptoms. D. Basket cells E. Purkinje cells 143 Das and Baugh, Medical Neuroscience Q&A (ISBN 978-1-62623-537-3), copyright © 2019 Thieme Medical Publishers. All rights reserved. Usage subject to terms and conditions of license. 16 Cerebellum 15. Which of the following is the likely diagnosis? A. Type I Chiari malformation 19. Which of the following areas receives input from the ankle joint? B. Type II Chiari malformation A. Area A C. Dandy–Walker syndrome B. Area B D. Occipital encephalocele C. Area C E. Holoprosencephaly D. Area D 16. Which of the following is a likely associated finding? 20. Output from which of the following areas is contained within the uncinate fasciculus? A. Syringomyelia A. Area A B. Herniation of cerebellar tonsils through foramen magnum B. Area B C. Herniation of cerebellar vermis through foramen magnum D. Area D C. Area C D. Agenesis of cerebellar vermis E. Buckling (Z deformity) of the medulla 16.2 Answers and Explanations Consider the following image for questions 17 to 20: Easy Medium Hard Refer to the following image key for answers 1 to 3: A, SCP; B, inferior cerebellar peduncle; C, stria medullaris of the fourth ventricle; D, MCP; E, superior medullary velum. 1. Correct: Area D (D) Pontocerebellar fibers contain sensory information from the cerebral cortex (conveyed by corticopontine fibers to pontine nuclei) and travel to the contralateral cerebellum via the MCP (D). 2. 17. Which of the following areas is the primary destination for fibers conveyed within the MCP? A. Area A B. Area B C. Area C D. Area D 18. Which of the following areas functions by influencing the MLF? A. Area A B. Area B C. Area C D. Area D Correct: Area B (B) The inferior cerebellar peduncles (B) communicate between the cerebellum and the medulla. These carry climbing fibers (from the contralateral inferior olivary nuclear complex) to the cerebellum. All other input to the cerebellum are via mossy fibers. 3. Correct: Area A (A) The superior (A) cerebellar peduncles carry efferent fibers from the cerebellum to the thalamus (dentatothalamic fibers), often via the red nucleus (dentatorubrothalamic tract). The stria medullaris of the fourth ventricle (C) consists of fibers travelling to the cerebellum from the arcuate nuclei (within the medulla) via the inferior cerebellar peduncle. The roof of the rhomboid fossa is formed by the superior medullary velum (E). The trochlear nerve decussates in the rostral aspect of the velum. 144 Das and Baugh, Medical Neuroscience Q&A (ISBN 978-1-62623-537-3), copyright © 2019 Thieme Medical Publishers. All rights reserved. Usage subject to terms and conditions of license. 16.2 Answers and Explanations 4. Correct: Purkinje cells (E) The internal circuitry of the cerebellum is depicted in the following flowchart: In the cerebellar glomerulus, the mossy fiber afferents synapse with granule cells (A). After this first processing stage, the granule cells convey this afferent information through the excitatory parallel fibers to the Purkinje cells and the Golgi cells (B). The Golgi cell exerts an inhibitory (feedback) influence on the synapse between the mossy fibers and the granule cells, within the glomerulus. The Purkinje cells also receive direct afferent information (excitatory) through the climbing fibers. Further inhibitory synapses with the Purkinje cells are from stellate cells (C) and basket cells (D). The Purkinje cells then send its efferent projections (inhibitory) to the deep cerebellar or vestibular nuclei. These nuclei serve as relay and processing stations for information coming from the cerebellar cortex to targets outside the cerebellum. Consider the following explanation for answers 5 and 6: Chiari malformations are defined as cerebellar herniation through foramen magnum due to a normalsized cerebellum developing within an abnormally small posterior fossa. 5. Correct: Herniation of lower medulla through foramen magnum (B) Chiari type II (Arnold–Chiari) malformation presents in infancy and is characterized by herniation of cerebellar vermis and lower medulla through the foramen magnum. Isolated herniation of the cerebellar tonsils (A) occurs in type I Chiari malformation. Enlarged posterior fossa (C), atresia of the foramens of Luschka and Magendie (D), and agenesis of the cerebellar vermis (E) occur in Dandy–Walker syndrome. 6. Correct: Myelomeningocele (B) Myelomeningocele is an inevitable association with Arnold–Chiari malformation. Buckling of the medulla, beaking of the tectum, colpocephaly, lacunar skull, and platybasia are associated signs. Syringomyelia (A) in which a cavity forms within the spinal cord can occur in type II Chiari malformations; however, it is much more frequent in type I. Platybasia, or flattening of skull base (C), is a frequent finding in type II Chiari malformation. 145 Das and Baugh, Medical Neuroscience Q&A (ISBN 978-1-62623-537-3), copyright © 2019 Thieme Medical Publishers. All rights reserved. Usage subject to terms and conditions of license. 16 Cerebellum Supratentorial structures (D) are often involved in type II Chiari malformation. Hypoplastic and irregular tentorium and falx (Chinese letter sign), enlarged interthalamic adhesion, and agenesis of corpus callosum could occur. Hydrocephalus, if present in Arnold–Chiari malformation, occurs from cerebral aqueduct stenosis. Hydrocephalus due to adhesions occluding the fourth ventricle (E) is commonly seen in type I Chiari malformation. 7. Correct: SCA (C) The SCAs supply the upper part of the cerebellum, which includes most of the deep cerebellar nuclei (dentate, interposed [globose and emboliform], and fastigial), rostral portion of the MCP, and SCP. The AICA (A) supplies anterior portions of the inferior cerebellum including the flocculus, caudal part of the dentate nucleus, and most of the MCP. The PICA (B) supplies majority of the inferior surface including inferior vermis and ICP. Pontine branches of the basilar artery (D) supply the pons. A pair of vertebral arteries (E) joins to form the basilar artery. 8. Correct: Rostral part of the basilar artery proximal to its bifurcation (C) The SCAs arise bilaterally near the rostral end of the basilar artery, proximal to its bifurcation. This region will, therefore, need to be clamped to operate on the bleeding SCA. Clamping the basilar artery just distal to its formation (D) will occlude blood supply to vital brainstem and cerebellar structures and should not be considered. The internal carotid (A), vertebral (B), or subclavian (E) arteries are too far and unrelated to the bleeding vessel. Consider the following explanation for answers 9 and 10: The most consistently reported structural damage in the cerebellum of alcoholics is tissue volume loss in the anterior superior vermis. Tissue volume loss in this area is due especially to either shrinkage or atrophy of Purkinje cells. Cerebellar shrinkage is most notable in older alcoholics with at least a 10-year duration of alcoholism. In contrast to alcohol, which exerts its greatest effect on the anterior superior lobules, normal aging primarily affects the posterior lobules. 9. Correct: Superior vermis (B) 10. Correct: Purkinje cells (E) 11. 146 Correct: Flocculonodular lobe (E) The flocculonodular lobe, via its bidirectional connections with the vestibular nuclei, influences the medial longitudinal fasciculus (MLF) and plays an important role in maintaining balance and vestibulo-ocular reflexes. Lesion to this part of the cerebellum leads to truncal ataxia, vertigo, and nystagmus. Ventral and rostral spinocerebellar fibers traverse the SCP (A) to project to the paravermal (B) area within the cerebellum. These structures influence distal limb coordination and their lesion might cause appendicular ataxia, intention tremor, hypotonia, etc. Output fibers from the posterior cerebellar lobe (C) and the dentate nucleus (D) form the dentatorubrothalamic tract and traverse the SCP (A). These tracts are involved in motor planning for the extremities and their lesion might cause different forms of appendicular ataxia (dysdiadochokinesia, dysmetria, etc.). 12. Correct: Dysdiadochokinesia (D) The patient is suffering from dysdiadochokinesia, which is a form of appendicular ataxia characterized by abnormalities of rapid alternating movements. Ataxic movements might have abnormal timing (dysrhythmia, B) or abnormal trajectories (dysmetria, C). Asterixis (A), or flapping tremor, is a form of brief rapid movement that is often seen in metabolic encephalopathies, particularly in hepatic failure. Titubation (E) is a peculiar tremor of the head or the trunk that occurs with midline cerebellar lesions. 13. Correct: Dentate nucleus (A) Output from the neocerebellar cortex is primarily to the dentate nucleus, which in turn projects to the red nucleus (parvocellular part) and from there to the VLC of the thalamus, making up the dentatorubrothalamic tract. From the thalamus, information projects back to motor (primary and association) areas of the cortex. This circuit is involved in planning motor programs for the extremities. Lesions to the involved structures cause different forms of appendicular ataxia (dysdiadochokinesia, dysmetria, etc.). The flocculonodular lobe (C), via its bidirectional connections with the vestibular nuclei, influences the MLF and plays an important role in maintaining balance and vestibulo-ocular reflexes. Lesion of this part of the cerebellum leads to truncal ataxia, vertigo, and nystagmus. Afferents from the vestibular nuclei also project to the vermis (D). The midline vermis projects to fastigial nuclei (B) and is important in the control of proximal limb and trunk muscles. Lesions of these structures will primarily cause truncal ataxia. The ventral spinocerebellar tract (E) originates from leg interneurons within the spinal cord and projects to the intermediate or paravermal area within the cerebellum. Lesion of this structure is unlikely to cause upper limb ataxia. Das and Baugh, Medical Neuroscience Q&A (ISBN 978-1-62623-537-3), copyright © 2019 Thieme Medical Publishers. All rights reserved. Usage subject to terms and conditions of license. 16.2 Answers and Explanations 14. Correct: Contralateral inferior olivary nuclei, excitatory (D) Climbing fibers carry excitatory inputs from the contralateral inferior olivary nucleus and synapse directly onto Purkinje cells. The inferior olivary nuclei are fed by several important structures including cerebral cortex, red nucleus, brainstem, and spinal cord. 15. Correct: Dandy–Walker syndrome (C) The patient has classical features of Dandy–Walker syndrome, which presents with hydrocephalus, ataxia, mental retardation, and/or seizures. Type I Chiari malformation (A) presents in young adults and is characterized by herniation of cerebellar tonsils. Type II Chiari malformation (B) presents in infancy and is characterized by herniation of cerebellar vermis and lower medulla. Occipital encephalocele (D) is characterized by herniation of brain tissue (enclosed in meninges) through a defect in the occipital bone. Holoprosencephaly (E) occurs when the prosencephalon fails to cleave down the midline such that the telencephalon contains a single ventricle. 16. Correct: Agenesis of cerebellar vermis (D) Components of Dandy–Walker syndrome include enlarged posterior fossa, elevated tentorial attachment, agenesis of cerebellar vermis, and cystic dilation of the fourth ventricle. Herniation of cerebellar tonsils (B) and syringomyelia (A) are features of Chiari type I malformation. Herniation of cerebellar vermis (C) and buckling of medulla (E) are seen in type II Chiari malformation. Refer to the following image key 17 to 20: A, intermediate/paravermal area; B, vermis; C, lateral region; D, flocculus. 17. Correct: Area C (C) Broad areas of cerebral cortex project to the ipsilateral pontine nuclei (corticopontine fibers). From the pontine nuclei, fibers cross the midline (pontocerebellar fibers) and, via the MCP, project to the lateral areas of the cerebellar hemisphere. 18. Correct: Area D (D) The flocculonodular lobe, via its bidirectional connections with the vestibular nuclei, influences the MLF and plays an important role in maintaining balance and vestibulo-ocular reflexes. 19. Correct: Area A (A) Unconscious proprioception from lower limb muscles and joints is relayed to Clarke’s nucleus in the spinal cord. From there, the fibers travel as dorsal spinocerebellar tract through the ICP to the paravermal or intermediate area of the cerebellum. 20. Correct: Area B (B) Afferents from the vestibular nuclei project to the vermis. The midline vermis projects to fastigial nuclei. Contralateral fibers from the fastigial nucleus form the uncinate fasciculus and projects back to vestibular nuclei. 147 Das and Baugh, Medical Neuroscience Q&A (ISBN 978-1-62623-537-3), copyright © 2019 Thieme Medical Publishers. All rights reserved. Usage subject to terms and conditions of license. Das and Baugh, Medical Neuroscience Q&A (ISBN 978-1-62623-537-3), copyright © 2019 Thieme Medical Publishers. All rights reserved. Usage subject to terms and conditions of license.