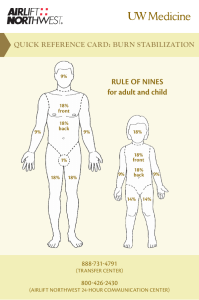
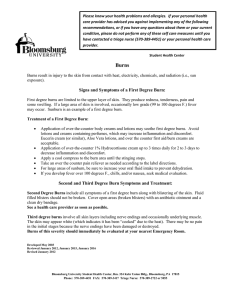
WRITING SAMPLE 1 This writing sample is extracted from a business case that I worked on and is based on the introduction section divided into sub-sections- on the severity of acute burns and its associated complications. 1 Burden of Disease Introduction Severe burns are one of the most common and traumatic injuries that trigger devastating morbidity and significant mortality. Despite decreasing incidence worldwide, severe burn injuries still have poor management and cause debilitating complications including infections. A plethora of factors guide the evaluation, management and treatment of severe burns including the amount of body surface area burned (expressed as a percentage of total body surface area (TBSA)) (2) and the degree of burns. The TBSA is determined by “rule of nines”, which helps guide treatment decisions such as fluid resuscitation. It is integrated as part of the treatment guidelines to determine if there is a need to transfer a patient to a burn’s unit. According to the rule of nines each body part is assigned a certain percentage as shown in the Figure 1 and Figure 2 below. Burns have four varying degrees depending upon the severity and the depth of the burn wound. Figure 1: Rule of nines percentages Anterior thorax 18% Posterior thorax 18% Leg 18% Arm 9% Head / neck 9% Perinuem 1% Figure 2: Rule of “nines” Panel A – Is often sued to estiamte the surface area of a burn in adults. However this approach is less accurate in children. Panel B- Lund -Browder use values for the legs and head that vary according to a patient’s age. *Subtract 1% from head for each year over one year of age **Add 1/2 % to each leg for each year over one year of age Epidemiology Severe burns are devastating injuries that cause significant morbidity and mortality as well as a financial burden to the health service with extensive hospitalization, rehabilitation and expensive treatments (3). The consequences of burns for patients can also be devastating and include hypertrophic scarring, disfigurement and functional impairment (3). Severe burns cause debilitating effects on the life of the patients and their families. The mortality rate of burn injuries in Europe is between 1.4-18% (4). In England and Wales only, 81,181 patients were referred for burn injuries in 9 years from 2003-2011, of which 57,801 were admitted to the hospital (5). Annual incidence of severe burns • 0.2 - 2.9 / 10,000 inhabitants in Europe (1) WHO estimates (2) • 180,000 deaths every year are casued by burns The major risk factors that may increase the mortality rate of patients due to acute burns include (6); Older age Higher total burned surface area (TBSA) ~ 80% Smoke Inhalation injuries Clinical Burden Severe burn injuries can lead to significant morbidity such as traumatic and physically debilitating conditions (7). Urgent specialized care is imperative in order to minimize morbidity and mortality. Surgical procedures are used to restore mobility and functional outcomes (8). Burn injuries often lead to complications including; Infections Functional impairment Scarring and disfigurement 1.3.1 Infections The maximum destruction and loss due to severe burns are caused to the skin. Since skin acts as the major protective barrier for the human body, its destruction and loss sets the patients up for invasion by microorganisms causing infection and sepsis (9). Infections pose a serious problem in burn management since they cause a delay in epidermal maturation and lead to additional scar tissue formation (10, 11). Burn wounds are the one of the most common sites of an infection (12). 75% of all deaths in patients with severe burns who have a TBSA of more than 40% , are due to infections, sepsis or inhalation injury (13). Invasive infections account for 51% of death in burn patients, are the primary reasons for death after the first 24 hours of admission to the hospital and often lead to death of the patients after the first 2 weeks of hospitalization. Infections due to sever buns are also expensive to treat. The estimates from National Healthcare System (NHS) United Kingdom (UK) suggest that the cost per patient for infections or complications of procedures with multiple interventions are high (14). Hence it is imperative for a burn treatment to target and prevent/cure infections in burn patients. Infection may lead to invasion of microorganisms into the layer of tissue below the dermis which might result in sepsis and/or impair organ function leading to multiple-organ dysfunction syndrome (MODS) (12) and increase the mortality rate (15). Several factors increase the risk of MODS including >20% TBSA, age, male gender sepsis, hypoperfusion and under-resuscitation. 1.3.2 Long term complications The long-term challenges for severely burn patients include scarring, functional impairment, change in appearance disfigurement among others. Burns near the face and hands are notably challenging and disturbing as they are always visible to other people. They lead to changes in the cosmetic appearance of the patient and can cause deleterious psychological effects. Burns occurring near joints often make them less mobile. Further, burn sites are sensitive to heat or cold from solar radiation or warmth which might cause pain and discomfort (8). Burns can also cause long term functional disabilities. It has been reported that 15-20% of patients who have more than 70% TBSA have serious physical disability even 15 years after the injury (16). If burn patients are not treated properly or if their deep dermal burns are not identified then scar contracture may form which can lead to disfigurement and/or functional impairment depending on the location of the burn (8). Functional impairment is a serious complication of acute burns since it intervenes and limits the daily activities of the burn patient. Most of the time functional impairment requires reoperation in order to enhance mobility. Despite several advances in the early treatment of burns, functional and aesthetic complications including slow wound healing, infection, pain, and hypertrophic scarring continue to remain the major challenges in burns management (17).