Pediatric Constipation & FTPM: Causes, Diagnosis, Management
advertisement

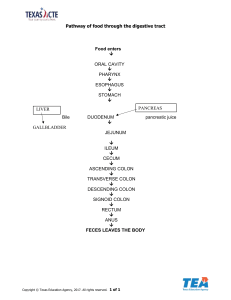
Pediatrics [CONSTIPATION + FTPM] Introduction “Slow gut” is a general term we’re using to describe a category of diseases that involve the bowel. Stratify this general concept into failure to pass meconium (FTPM) seen in the first days of life and infrequent hard stools in toddlers or older children. For FTPM, anything that prevents stool from getting from the stomach to the anus should be considered. Specifically, the obstructive diseases in bilious emesis in the Emesis lecture should be considered. But the diseases you should commit to memory are the three below. Usually 48 hours is the cutoff for this. However, almost 99% of term kids pass stool by 24 hours and 100% pass by 48 hours. The timing is delayed in premature infants. In general, once you’ve hit 24 hours the odds are there’s something wrong FTPM Imperforate Anus Meconium Ileus Constipation Voluntary Holding Hirschsprung's Hirschsprung's Bilious emesis Mom’s Mg, K Medications, Baby’s Mg, K 1) Imperforate Anus The earliest and most obvious of causes of FTPM. Just look at it - there’s no hole. This is why we NEVER take a baby’s first temp rectally. But there’s a continuum of disease. Do a cross table X-ray on the prone child with radiopaque perineal marking. This will give a relationship between gas bubble and anus. Low lesions (closer to the anus) can be corrected via dilation or a minor surgical procedure. There’s also a higher chance of maintaining continence. High lesions (away from the anus) need a colostomy with future correction. All patients need evaluation for VACTERL and should undergo sacral ultrasound and X-ray, VCUG, NG tube passage, and echocardiogram. 2) Meconium Ileus Usually seen in patients with cystic fibrosis, it’s a collection of meconium that too thick and viscous to pass as a result of pancreatic insufficiency. Typical location is in the ileum - hence its placement in the “small bowel” section. This can cause any combination of bilious vomiting or failure to pass meconium. X-ray can show an area of obstruction (air-fluid levels) with a gas-filled plug. Perform water-soluble contrast enema (like gastrografin) to help breakdown the obstruction. Sometimes surgical intervention is required. Complications include perforation which can lead to meconium peritonitis (which is an emergency). 3) Hirschsprung’s This is caused by absent ganglion migration to the Meissner and Auerbach plexuses in the colon. This means no motility – the muscles are unable to relax and contribute to peristalsis. It just so happens that it’s a migratory issue, which means only the proximal colon (area with ganglions) is effective. Regardless, the x-ray is the first step; it will show a dilated proximal colon (normal) and a normal looking distal colon (abnormal). There are two presentations; they drive the diagnostic step. The first is failure to pass meconium, occurring in 90% of cases. It’s diagnosed with a contrast enema, which shows a transition zone and is followed up by a biopsy. The second, occurring in 10% of cases, presents with overflow incontinence in the older child or a stool eruption after doing a digital examination in the nursery. Anorectal manometry is done which shows increased tone, followed by biopsy. Resect the affected area and connect (pull-through procedure). Severe cases (perforation, full colon involvement) require colostomy. © OnlineMedEd. http://www.onlinemeded.org Pediatrics [CONSTIPATION + FTPM] 4) Voluntary Constipation The most common cause of constipation is voluntary holding. Whether to avoid pain or simply due to embarrassment, kids may hold it in. The longer they hold it the more water gets taken out of it - the harder it gets. Because the colon is working, stool may sneak around and cause intermittent diarrhea or encopresis. To get the kid unplugged (voluntary may convert to involuntary) there may have to be a disimpaction in the OR. Make sure to teach the child that holding it in is dangerous! 5) Additional Causes Other Causes There are other causes of small bowel obstruction leading to failure to pass meconium that are covered under the Vomiting review as the presentation can include any combination of failure to pass meconium and bilious vomiting. These causes include duodenal atresia, malrotation/volvulus, and distal intestinal atresia. See Vomiting for more information. Medication-induced Sometimes we do things that cause other issues. Failure to pass meconium is no exception. Medications given to both mother and infant can affect stool transit. Think of the mother with pre-eclampsia that received magnesium. Think of the infant born with neonatal abstinence syndrome (narcotic withdrawal) who is receiving opiates. Metabolic-induced Electrolyte derangements can contribute to decreased gut motility. Keep in mind two “high” ones (hypercalcemia, hypermagnesemia) and two “low” ones (hypoglycemia, hypokalemia). Also consider additional endocrine causes such as hypothyroidism and adrenal insufficiency. CONSTIPATION IN GENERAL Overview There are a multitude of criteria that can be used to define constipation (Rome III is one). They’re not worth remembering as nobody agrees on a unified definition anyway. Just remember that essentially you’re looking for bowel movements associated with pain, straining, decreased frequency, or incontinence. Constipation can be broken down into two etiological categories: organic (underlying pathology) and functional (no underlying medical pathology). A thorough history and physical will be the best way to obtain a diagnosis. Ask about initial bowel movements as a history of delayed meconium passage could points towards organic cause. Also ask about stressors and history of previous continence as these could point towards a functional cause. Red flags include: fever, blood per rectum, complete obstruction, failure to thrive, and weight loss © OnlineMedEd. http://www.onlinemeded.org