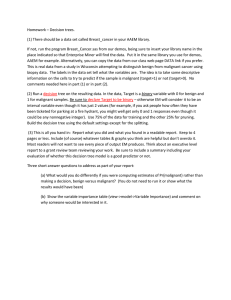
NEUROLEPTIC MALIGNANT SYNDROME Dr. Sumesh Balachandran Assistant Professor Dept. of Psychiatry Govt. Medical College Kannur, Kerala CONTENTS Case Vignette Introduction Diagnosis Pathophysiology Risk factors Causative drugs Laboratory findings Differential Diagnosis Management Prognosis Conclusion Case Vignette • A 45 year old woman • History of BPAD and hypertension • Hospitalized with depressed mood of one month’s duration. • In prior episodes, she had received antidepressants, lithium and ECT. • On admission, she was excited with idiosyncratic behavior with confused speech and thought. • Two doses of haloperidol were administered. • Her excitement subsided. • She became grandiose, garrulous and paced continuously. • Lithium carbonate was prescribed and fluphenazine hydrochloride (5 mg Q.D.S. daily) was added. • Within 48 hours, she exhibited bilateral cogwheel rigidity • Improved with IM promethazine hydrochloride. • The next day, she became tremulous, had persistent cogwheel and her temperature rose to 100 F. • Contemplating neurotoxicity, both lithium and fluphenazine were discontinued. • Her condition worsened and she became mute, tremulous and rigid and diaphoretic. • B.P. and heart rate increased, temperature rose to 103.5 F. • Lungs clear • Abdomen- soft, non- tender, nil bowel sounds • No meningism or focal neurological deficit • Pupils – normal, reactive • No clonus • Reflexes normal • WBC count was 13,500/ cubic mm and CPK was 1486 IU/l. All other investigations WNL (including CT Brain and EEG). How will you manage this case? • Neuroleptic Malignant Syndrome • Syndrome malin des neuroleptiques Introduction • • • • • Rare but potentially life-threatening idiosyncratic reaction First description (Delay et al. )- 1960 - Haloperidol Incidence – 0.02 to 3 % Males > females (3:2) Age - < 20 years and > 65 years • A retrospective study conducted in India showed an incidence of 0.14%. Chopra MP, Prakash SS, Raguram R. The neuroleptic malignant syndrome: an Indian experience. Compr Psychiatry. 1999 Jan-Feb. 40(1):19-23. • NMS usually occurs after exposure to an neuroleptic drug. • On an average, onset is 4-14 days after the start of therapy • 90% of cases occur within 10 days. • NMS can occur years into therapy. • Once the syndrome starts, it usually evolves over 24-72 hours. • Mnemonic- “ F.E.V.E.R.” Diagnostic criteria (DSM 5) (all 3 major or 2 major and 2 minor) • Major criteria (all required) 1. Exposure to dopamine antagonist or dopamine agonist withdrawal with 72hours 2. Muscle rigidity 3. Hyperthermia (>100.4 deg. F or > 38 deg. C, measured orally on at least two occasions) • • • • Nierenberg and colleagues’ criteria Levenson’s criteria Caroff and Mann’s criteria Hope’s criteria • Minor (at least 2 required) 1. Diaphoresis 2. Dysphagia 3. Tremor 4. Incontinence 5. Altered levels of consciousness 6. Mutism 7. Tachycardia 8. Elevated or labile B.P. 9. Leukocytosis 10. Elevated CPK (> 4 times) 70 % Altered consciousness Autonomic instability NMS Generalized rigidity with tremors Hyperthermia Altered mental state • Perplexity • Delirium • Stupor • Coma Rigidity • Generalized and extreme • Lead pipe rigidity • Superimposed on tremors cog- wheel • Generalized tremors • Dyskinesia, dysarthria and myoclonus • Catatonic symptoms (mutism, posturing, waxy flexibility, catalepsy) Autonomic instability • Tachycardia (in 88 percent) • Labile or high blood pressure (in 61 to 77 percent), • Tachypnoea (in 73 percent) • Dysrhythmias • Incontinence • Diaphoresis- profuse (“greasy” sweat) Hyperthermia • 100 to 105 degrees F • May not be evident with second generation antipsychotics • May be fluctuating • - “Atypical” NMS: DSM 5 criteria not met Milder form Only hyperthermia and/or rigidity Clozapine, Aripiprazole and paliperidone Pathophysiology • Secondary to decreased dopamine (DA) activity in central nervous system (CNS): • • Blockade of dopamine type 2 receptors (D2 receptors) • • Decreased availability of DA itself. • Direct effect on peripheral skeletal muscles may play an additive role • Hypothalamic D2 receptor blockade results in an elevated temperature set point • Impairment of heat-dissipating mechanisms (eg. cutaneous vasodilatation, sweating) • Nigrostriatal blockade results in muscular rigidity. • Peripherally, antipsychotics lead to increased calcium release from the sarcoplasmic reticulum • Increased contractility, which can contribute to hyperthermia, rigidity, and muscle cell breakdown. • Removing tonic inhibition from the sympathetic nervous system. • The resulting sympathoadrenal hyperactivity and dysregulation leads to autonomic dysfunction. • Animal model studies- orexin-A (an excitatory neuropeptide) can cause thermogenesis in a manner unrelated to muscle activity. • Orexin-1 receptor plays a role in the effects of psychotropics on dopamine pathways • And probably the clinical effects of these agents (therapeutic and side effects). Risk factors • • • • • • • Genetics Young Males Dehydration/ malnutrition Exposure to high ambient temperatures Agitation or excitement Catatonic features, past or present Tardive dyskinesia, akathisia, EPS Risk factors (contd..) • Past history of NMS • Sudden dose escalation of antipsychotics • High potency antipsychotic or two or more antipsychotics • High potency antipsychotic with an antidepressant or mood stabilizer (lithium) • IM antipsychotic or depot antipsychotic • Recent alcohol abuse with liver dysfunction Risk factors (contd..) • • • • • Alcohol use Trauma Infections Thyrotoxicosis, Premenstrual/ Post partum phase Early signs • Rapidly developed extra-pyramidal signs of tremors, rigidity, dyskinesia to low or modest doses of an antipsychotic • Mania with fever • Within 24 hours of initial - Catatonia antipsychotic administration - Sialorrhoea - Autonomic instability Pharmacological agents Withdrawal of: • Levodopa (L-DOPA) • Tolcapone/entacapone • Dopamine agonists (e.g. bromocriptine) • Amantadine • Clozapine Introduction of: • Neuroleptics: Phenothiazines, butyrophenones, thioxanthenes • “Atypical” antipsychotics: clozapine, olanzapine, risperidone, quetiapine Intoxication with: • Disulfiram • Steroid • Anticholinergics • Cocaine • Metoclopramide • Promethazine Abnormal laboratory findings • Very high CPK - 1000 – 10000 IU/L • Low serum iron (11- 32 µmol/L) - sensitive marker - 5.17 µmol/L • High LDH • Leukocytosis with a left shift (10,000 to 40,000) Abnormal laboratory findings • Proteinuria • Myoglobinuria • Thrombocytosis • Metabolic acidosis • Liver transaminases elevated • Diffuse EEG slowing • High CSF proteins • - Dyselectrolemia Hypocalcaemia, Hypomagnesaemia Hyperkalemia Hyper/ hyponatremia Differential Diagnosis • • - Other neuroleptic induced reactions Dystonia Akathisia Dyskinesias Pseudoparkinsonism Malignant Catatonia prodrome of excitement and agitation with hyperthermia prior to the onset of rigidity - episodes of catatonia while a patient is not taking neuroleptics - Serotonin syndrome - Clonus and hyperreflexia, hypertonia - Malignant hyperthermia • • • • • • • • • • • • Central nervous system infections Status epilepticus Stroke Brain trauma Neoplasms Acute intermittent porphyria Tetanus Thyroid Storm Heat stroke Sepsis Pheochromocytoma Drug intoxication Management • Mainly supportive!!! • Prevent complications • ICU care is quintessential • Discontinue all antipsychotics • Assessment of the airway, breathing, and circulation (ABCs) • Assess safety and restrain if needed (chemical preferred) • Thiamine, dextrose (or rapid glucose determination), and/or naloxone, in case of alcohol withdrawal, hypoglycemia, and opioid overdose • Take a detailed drug history Conservative management • • • • • • • • Circulatory and ventilatory support as needed. Antipyretics Evaporative cooling Ice packs (axilla) Cooled intravenous (IV) fluids Cooling blankets Ice water gastric lavage Prophylactic intubation for patients with excessive salivation, swallowing dysfunction, coma, hypoxemia, acidosis, and severe rigidity with hyperthermia • • If B.P. is significantly elevated Nitroprusside (cutaneous vasodilatation) Clonidine Heparin or low molecular weight heparin for prevention of deep venous thrombosis • - Consultations – eclectic team approach Neurologist Nephrologist Cardiologist Psychiatrist • Aggressive fluid resuscitation and alkalization of urine • Sodium bicarbonate - prevent acute renal failure and - enhance excretion of muscle breakdown products Pharmacotherapy • Benzodiazepines - For mild NMS - Lorazepam -1 to 2 mg IM or IV every four to six hours - Diazepam 5 to 10 mg IV every eight hours. • Bromocriptine mesylate - Dopamine agonist - 2.5 mg orally two or three times a day, increased by 2.5 mg per 24 hours to a total daily dose of 45 mg. - Can worsen psychosis and hypotension. - Precipitate vomiting - should be used carefully in patients at risk of aspiration. - Premature discontinuation results in rebound symptoms - Safe in pregnancy - Continue for 10 days followed by a slow taper to minimize relapse • Dantrolene - Direct acting skeletal muscle relaxant - 1–2.5 mg/kg body weight administered initially - followed by 1 mg/kg every 6 hours if rapid resolution of the fever and rigidity is observed - Maximum dose- 10 mg/kg - Taper or switch to oral dantrolene after the first few days. - Oral dantrolene doses - 50 to 200 mg/d - Continue for 10 days followed by a slow taper to minimize relapse - Side effects may include impairment of respiratory or hepatic function - Only in cases of NMS with extreme temperature elevations, rigidity, and true hypermetabolism • With depot neuroleptics, treatment should be continued up to 2–3 weeks beyond clinical recovery. • - Amantadine Dopamine agonist Initial dose is 100 mg orally or via gastric tube Titrate upward as needed to a maximum dose of 200 mg every 12 hours - Caution- worsening of psychosis - Levodopa, combined with the dopadecarboxylase inhibitor carbidopa- effective in reversing hyperthermia • Serial follow-up of CK and myoglobulin levels. • Do not suddenly withdraw treatment despite recovery. • High chances of recurrence • With depot neuroleptics, treatment should be continued up to 2–3 weeks beyond clinical recovery. • Electro-convulsive therapy (ECT) - Can help with the alteration of temperature, level of consciousness, and diaphoresis. - Effective if symptoms are refractory to supportive care and pharmacotherapy - Idiopathic malignant catatonia due to an underlying psychotic disorder - persistent residual catatonia and parkinsonism after resolution of NMS • Six to 10 treatments with bilateral electrode placement - It may also be useful in treating the underlying psychiatric disease in patients who are unable to take neuroleptics. - ECT with anesthesia has generally been safe - No increased incidence of malignant hyperthermia from succinylcholine administration. • Risks- cardiac arrest, ventricular fibrillation and status epilepticus What will happen if you don’t intervene? • Dehydration • Electrolyte imbalances • Acute renal failure associated with rhabdomyolysis • Cardiac arrhythmias including torsade de pointes and cardiac arrest • Myocardial infarction • Cardiomyopathy • Sepsis • Reversible dilated myocardiopathy ( Takotsubo myocardiopathy) • Respiratory failure from chest wall rigidity, aspiration pneumonia, pulmonary embolism • Deep vein thrombosis (DVT) • Thrombocytopenia • Disseminated intravascular coagulation (DIC) • Seizures from hyperthermia and metabolic derangements • Hepatic failure Restarting of antipsychotics • Likelihood of developing NMS again as high as 30% • reports of previous episodes should be checked for accuracy • indications for antipsychotics should be clearly documented • alternative medications should be considered • risk factors should be reduced • At least 2 weeks should be allowed to elapse after recovery from NMS before rechallenge. • 6 weeks for depot injections • Low doses of low-potency conventional antipsychotics or atypical antipsychotics should be titrated gradually after a test dose. • Patients should be carefully monitored for early signs of NMS. • Documented written consent Prognosis • Resolve within 2 weeks (reported mean recovery times are 7–11 days). • Cases persisting for 6 months with residual catatonia and motor signs are reported. • Risk factors for a prolonged course are depot antipsychotic use and concomitant structural brain disease. Prognosis • Most patients recover without neurologic sequelae • Except where there is severe hypoxia or grossly elevated temperatures for a long duration. • Reported mortality rates for NMS are 5–20%. • Disease severity and the occurrence of medical complications are the strongest predictors of mortality. Conclusion • Neuroleptic malignant syndrome is rare but lifethreatening medical emergency • A diagnosis of exclusion • Following usage of neuroleptics and abrupt withdrawal of some drugs. • Tetrad: Altered mental state, Rigidity, Hyperthermia and Autonomic dysfunction • Due to blockade of D2 receptors • No pathognomonic lab tests. • Early recognition and prompt treatment has shown encouraging outcome (reduced mortality). References • Eelco FM Wijdicks. https://www.uptodate.com/contents/neurolepticmalignant-syndrome- 2019 • Stanley NC, Cabrina EC. Drug- Induced Extrapyramidal Syndromes. Psychiatric Clinics of North America 2016;Vol 3, No 3: 399- 400 • Vivian Ngo, Alfredo G, David L, et al. Emergent Treatment of Neuroleptic Malignant Syndrome Induced by Antipsychotic Monotherapy Using Dantrolene. Clin Pract Cases Emerg Med. 2019 Feb; 3(1): 16–23. • Oruch R, Pryme IF, Engelsen BA, Lund A. Neuroleptic malignant syndrome: an easily overlooked neurologic emergency. Jan 2017 Volume 2017:13 Pages 161—175 References (contd.) • P. Adnet, P. Lestavel, R. Krivosic‐Horber. Neuroleptic malignant syndrome. BJA: British Journal of Anaesthesia, Volume 85, Issue 1, 1 July 2000, Pages 129–135 • Jeffrey RS, Paul EK, Stanley NC. Neuroleptic Malignant Syndrome. Am J Psychiatry 164:6, June 2007: 870- 876. • Brian DB. Neuroleptic Malignant Syndrome: A Review for Neurohospitalists. 2011 Jan; 1(1): 41–47 • Max Fink, Allan Taylor. Catatonia: A clinician’s guide to diagnosis and treatment. 2003: 45- 51. • Caroff SC, Mann SC, et al. Catatonia: From Psychopathology to Neurobiology. 2004: 105-115 • Theodore IB. Neuroleptic Malignant Syndrome. Dec 2018 Medscape • Lurdes Tse, Alasdair M. Barr, Vanessa Scarapicchia Fidel VilaRodriguez. Neuroleptic Malignant Syndrome: A Review from a Clinically Oriented Perspective. Current Neuropharmacology, 2015, 13, 395-406. Thank You