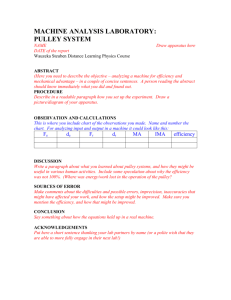
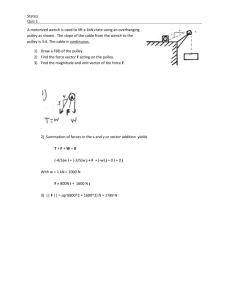
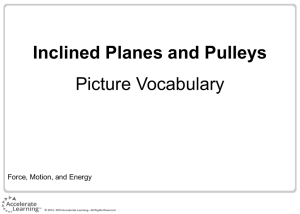
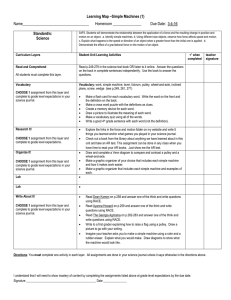
Journal of Hand Therapy 31 (2018) 416e420 Contents lists available at ScienceDirect Journal of Hand Therapy journal homepage: www.jhandtherapy.org JHT READ FOR CREDIT ARTICLE #563. Practice Forum Pulley injuries in rock climbers: Hand therapy clinical application Lori Algar OTD, OTR/L, CHT a, *, Matthew Moschetto OTS b a b Department of Hand Therapy, Orthopaedic Specialty Group, P.C., Fairfield, CT, USA Department of Occupational Therapy, Sacred Heart University, Fairfield, CT, USA New techniques using either taping and/or a custom fabricated pulley ring are recommended by these authors to treat pulley injuries in rock climbers. Either technique provides support to the injured pulley and allows rock climbers to continue their meaningful activity while the pulley heals. e KRISTIN VALDES, OTD, OT, CHT, Practice Forum Editor cohort study8 examined outcomes following pulley reconstruction with the use of a thermoplastic ring over the pulley for 90 days Introduction In the past, the frequency of treating rock climbers in the hand therapy clinic may in part have been determined by geographical location. However, the sport of rock climbing is increasing in popularity1 and will be included in the 2020 Olympic Games.2 This may cause an influx in the number of pulley injuries treated by hand therapists as these are the most common injuries sustained by rock climbers, occurring as 15.4% of all climbing injuries.3 Pulley injuries in rock climbers and traditional hand therapy pulley injury treatment Rock climbers often assume what is termed a crimp position (Fig. 1), a position of extreme flexion at the proximal interphalangeal (PIP) joint and hyperextension at the distal interphalangeal joint, to achieve greater strength in grip. This position applies approximately 287 Newtons (N) of force on the A2 pulley and 226 N at the A4 pulley.4 The A4 ruptures more often in climbers because the actual strength of the A2 pulley has been found to be greater than that of the A4.5 Flexion of the digit causes most stress to the distal end of the A2 pulley and the proximal aspect of the A4 pulley, as the A3 pulley does little in the way of supporting the tendon.6,7 Hand therapists are tasked with providing protection for the A2 and A4 pulleys for either conservative or postsurgical management. Our classic circumferential pulley ring may not be the best option for pulley protection especially in high-demand climbers. A recent * Corresponding author. Department of Hand Therapy, Orthopaedic Specialty Group, P.C., Fairfield, CT 06825, USA. Tel.: 203.337.2677; fax: 203.337.2675. E-mail address: lori.algar@gmail.com (L. Algar). Fig. 1. Crimp position. 0894-1130/$ e see front matter Ó 2017 Hanley & Belfus, an imprint of Elsevier Inc. All rights reserved. http://dx.doi.org/10.1016/j.jht.2017.05.019 Downloaded for Anonymous User (n/a) at University of Illinois System at Chicago from ClinicalKey.com by Elsevier on December 29, 2018. For personal use only. No other uses without permission. Copyright ©2018. Elsevier Inc. All rights reserved. L. Algar, M. Moschetto / Journal of Hand Therapy 31 (2018) 416e420 417 phalanx (just proximal to the PIP joint) for A2 pulley injuries as the tape did little to absorb flexor tendon force on the pulley or decrease bowstringing.9 In addition, studies on treatment outcomes for rock climbers who used conventional circumferential taping and thermoplastic rings to treat pulley injuries find increased tendon-phalanx distance (or bowstringing) via ultrasound.10, 11 Alternative methods for pulley protection H-tape Schoffl et al12 proposed the H-tape method for pulley protection. This method of taping considers the point at which the tendon has the greatest distance from the bone during flexion (the PIP joint), which is also where deflection of flexor tendon force is most important. In a research study using ultrasound on rock climbers with pulley injuries, the H-tape method was found to significantly decrease tendon-phalanx distance, whereas other tape applications did not change this measurement.12 Schoffl et al12 recommend a 10 cm by 1.5 cm piece of Leukotape. The tape should be cut in half through the length from both ends but leaving a 1-cm bridge uncut in the middle (Fig. 2). The tape should first be applied to the distal end of the proximal phalanx at the bridge of the tape and then the proximal straps should be wrapped around the proximal phalanx. The PIP joint should be flexed and then the remaining 2 distal straps secured around the proximal middle phalanx (Fig. 3).12 Fig. 2. Leukotape cut for H-tape application. Pulley-protection orthosis postoperatively. Only 18 of 30 participants had a return to near normal status related to flexor bowstringing.8 A biomechanical study found that it is minimally effective to apply tape circumferentially at the proximal phalanx and at the distal proximal In 2016, Schneeberger and Schweizer13 developed and tested a novel design of what they termed a pulley-protection orthosis. Their design is like the conventional pulley ring, but it has cutouts on the sides of the orthosis to allow firm fixation with inelastic tape Fig. 3. Application of the H-tape. Downloaded for Anonymous User (n/a) at University of Illinois System at Chicago from ClinicalKey.com by Elsevier on December 29, 2018. For personal use only. No other uses without permission. Copyright ©2018. Elsevier Inc. All rights reserved. 418 L. Algar, M. Moschetto / Journal of Hand Therapy 31 (2018) 416e420 Fig. 4. Pulley-protection orthosis. without compression of the digital nerves and blood supply (Fig. 4).13 The orthosis can be applied to provide force to the flexor tendon to keep close distance to the bone allowing the pulley to heal at an effective length.13 In a cohort study of 47 rock climbers with pulley injuries conservatively treated with this orthosis design, tendon-phalanx distance was reduced.13 To fabricate this orthosis, thin, long pieces of orthosis material covered with paper tape can be secured to the involved digit to allow the appropriate side cutouts (Fig. 5). The finished orthosis can be applied just proximal to the PIP joint and secured with inelastic tape (Fig. 6). Clinical implications: translating rock climbing interventions into other pulley injury cases Hand therapists are likely familiar with providing protection to injured finger pulleys after traumatic flexor tendon injury; however, we were not able to locate research on the use of pulley rings outside of the rock climbing research. The H-tape method and the pulley-protection orthosis may be appropriate substitutes for typical circumferential pulley rings. Hand therapists may consider use of these alternative designs to offer rock climbers and others with traumatic pulley injury best evidence-based practice. Fig. 5. Fabrication of the pulley-protection orthosis. Downloaded for Anonymous User (n/a) at University of Illinois System at Chicago from ClinicalKey.com by Elsevier on December 29, 2018. For personal use only. No other uses without permission. Copyright ©2018. Elsevier Inc. All rights reserved. L. Algar, M. Moschetto / Journal of Hand Therapy 31 (2018) 416e420 419 Fig. 6. Completed pulley-protection orthosis. Supplementary data Supplementary data related to this article can be found at http:// dx.doi.org/10.1016/j.jht.2017.05.019 References 1. Chang CY, Torriani M, Huang AJ. Rock climbing injuries: Acute and chronic repetitive trauma. Curr Probl Diagn Radiol. 2016;45:205e214. 2. Bisharat A. Olympics add climbing, surfing, and skateboarding for 2020. Natl Geogr Mag. 2016. Available at: http://www.nationalgeographic.com/adventure/ activities/climbing/climbing-surfing-skateboarding-at-2020-olympics/. Accessed March 19, 2017. 3. Schoffl V, Popp D, Kupper T, Schoffl I. Injury trends in rock climbers: evaluation of a case series of 911 injuries between 2009 and 2012. Wilderness Environ Med. 2015;26:62e67. 4. Schoffl I, Oppelt K, Jungert J, Schweizer A, Neuhuber W, Schoffl V. The influence of the crimp and slope grip position on the finger pulley system. J Biomech. 2009;42:2183e2187. 5. Lin GT, Cooney WP, Amadio PC, An KN. Mechanical properties of human pulleys. J Hand Surg Eur. 1990;15:429e434. 6. Marco RA, Sharkey NA, Smith TS, Zissimos AG. Pathomechanics of closed rupture of the flexor tendon pulleys in rock climbers. J Bone Joint Surg Am. 1998;80:1012e1019. 7. Hume EL, Hutchinson DT, Jaeger SA, Hunter JM. Biomechanics of pulley reconstruction. J Hand Surg. 1991;16:722e730. 8. Bouyer M, Forli A, Semere A, Chedal Bornu BJ, Corcella D, Moutet F. Recovery of rock climbing performance after surgical reconstruction of finger pulleys. J Hand Surg Eur. 2016;41:406e412. 9. Schweizer A. Biomechanical effectiveness of taping the A2 pulley in rock climbers. J Hand Surg Eur. 2000;25B:102e107. 10. Gabl M, Rangger C, Lutz M, Fink C, Rudisch A, Pechlaner S. Disruption of the finger flexor pulley system in elite rock climbers. Am J Sports Med. 1998;26: 651e655. 11. Schoffl V, Hochholzer T, Winkelmann HP, Roloff I, Strecker W. Pulley injuries in sport climbers [in German]. Handchir Mikrochir Plast Chir. 2004;36:224e230. 12. Schoffl I, Einwag F, Strecker W, Hennig F, Schoffl V. Impact of taping after finger flexor tendon pulley ruptures in rock climbers. J Appl Biomech. 2007;23:52e62. 13. Schneeberger M, Schweizer A. Pulley ruptures in rock climbers: outcome of conservative treatment with the pulley-protection splint- a series of 47 cases. Wilderness Environ Med. 2016;27:211e218. Downloaded for Anonymous User (n/a) at University of Illinois System at Chicago from ClinicalKey.com by Elsevier on December 29, 2018. For personal use only. No other uses without permission. Copyright ©2018. Elsevier Inc. All rights reserved. 420 L. Algar, M. Moschetto / Journal of Hand Therapy 31 (2018) 416e420 JHT Read for Credit Quiz: #563 Record your answers on the Return Answer Form found on the tear-out coupon at the back of this issue or to complete online and use a credit card, go to JHTReadforCredit.com. There is only one best answer for each question. #1. In rock climbers pulley injuries are the most common injury and account for approximately________ of their injuries a. 30% b. 25% c. 20% d. 15% #2. The crimp position of the digits includes a. hyperextension of the DIP and PIP b. extreme flexion of the PIP and DIP c. hyperextension of the DIP along with extreme flexion of the PIP d. hyperextension of the PIP along with extreme flexion of the DIP #3. The most vulnerable pulley to rupture in the crimp position is the________ pulley a. A4 b. A3 c. A2 d. A1 #4. The status of pulleys has been studied using a. X-rays b. ultrasound c. MRIs d. EMGs #5. The authors offer an H type pulley protection system as an alternative to the traditional O ring design a. false b. true When submitting to the HTCC for re-certification, please batch your JHT RFC certificates in groups of 3 or more to get full credit. Downloaded for Anonymous User (n/a) at University of Illinois System at Chicago from ClinicalKey.com by Elsevier on December 29, 2018. For personal use only. No other uses without permission. Copyright ©2018. Elsevier Inc. All rights reserved.