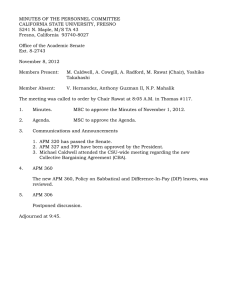
CED Original article Clinical and Experimental Dermatology Patients with a new variant of endemic pemphigus foliaceus have autoantibodies against arrector pili muscle, colocalizing with MYZAP, p0071, desmoplakins 1 and 2 and ARVCF A. M. Abreu-Velez,1 C. A. Valencia-Yepes,2 Y. A. Upegui-Zapata,3 E. Upegui-Quiceno,3 4,5 N. R. Mesa-Herrera, J. E. Velazquez-Velez6,7 and M. S. Howard1 1 Georgia Dermatopathology Associates, Atlanta, GA, USA; 2Department of Education, University of Antioquia, Medellin, Colombia; 3Pecet Group, University of Antioquia, Medellin, Colombia; 4Biogemo Institute, Medellin, Colombia; 5Department of Physiology and Biochemistry, School of Medicine, University of Antioquia, Medellin, Colombia; 6Department of Cardiology, Hospital General de Medellin, Medellin, Antioquia, Colombia; and 7Clinica CES Medellin, Medellin, Colombia doi:10.1111/ced.13214 Summary Background. We identified a new variant of endemic pemphigus foliaceus in El Bagre, Colombia, South America, which we term El Bagre-EPF, and observed reactivity to arrector pili muscle (APM), thus we tested for autoimmunity to APM. Methods. We took skin biopsies from 30 patients with El Bagre-EPF and 30 healthy controls (HCs) matched by age, sex and occupation, who were all from the endemic area, and tested these using direct immunofluorescence (DIF), confocal microscopy, immunohistochemistry and immunoblotting (IB). Results. Of the 30 patients with El Bagre-EPF, 27 had autoantibodies to APM that colocalized with commercial antibodies to myocardium-enriched zonula occludens-1associated protein (MYZAP), desmoplakin (DP)1 and DP2, plakophilin 4, and Armadillo repeat gene deleted in velo-cardio-facial syndrome (ARVCF) (P < 0.001, Fisher exact test). The positive staining also colocalized with Junctional Adhesion Molecule 1 (JAM-A), a control antibody for gap cell junctions. No HC samples were positive. In 27 of the 30 patients, serum that was APM-positive also displayed IB colocalization of their autoantibody molecular weights with the Progen antibodies (P < 0.001, Fisher exact test). Conclusions. Patients affected by El Bagre-EPF have autoantibodies to APM, colocalizing with the antibodies MYZAP, ARVCF, p0071, DP1 and DP2, suggesting that these molecules are El Bagre-EPF antigens. Further, all of these antigens represent components of cell junctions, indicating that the immune response is directed, at least partially, against cell junctions. The immune response in patients affected by El Bagre-EPF is polyclonal, and it includes B and T lymphocytes, mast cells, IgG, IgA, IgM, IgD, IgE, fibrinogen, albumin, complement/C1q, C3c and C4. Introduction Endemic pemphigus foliaceus (EPF) is a group of autoimmune blistering diseases considered variants of PF, but presenting in an endemic fashion.1–4 EPF was Correspondence: Dr Ana Maria Abreu-Velez, Georgia Dermatopathology Associates, 1534 North Decatur Road NE, Suite 206, Atlanta, GA, 303071000, USA E-mail: abreuvelez@yahoo.com Conflict of interest: the authors declare that they have no conflicts of interest. Accepted for publication 29 December 2016 874 Clinical and Experimental Dermatology (2017) 42, pp874–880 originally documented in recently deforested and mining areas near rivers; this presentation is particularly true in areas of Brazil, where mining and road construction have increased over the past century. EPF foci have also been described in Central American and other South American countries, as well as in Africa (Tunisia).1–5 Recently, the incidence and prevalence of EPF has decreased significantly, especially in Brazil.3,4 We have identified a new variant of EPF in El Bagre, Colombia, which we term El Bagre-EPF, and found that people with this disease have autoantibodies to desmoglein (Dsg)1 Dsg3, periplakin, envoplakin and ª 2017 British Association of Dermatologists Autoantibodies in a new variant of endemic pemphigus foliaceus A. M. Abreu-Velez et al. bullous pemphigoid antigen 1, and also to other, as yet unknown antigens.6 These patients also have autoantibodies to pilosebaceous units and associated neurovascular supply structures.7 In routine direct and indirect immunofluorescence (DIF and IIF) of these patients, we noticed a pattern of autoantibody deposits directed against arrector pili smooth muscle (APM). In the current study, we aimed to test for reactivity to the APM, using multiple antibodies, complement and other immunological activation markers. Methods A human quality assurance review board approved the studies at the Hospital Nuestra Se~ nora del Carmen in El Bagre, and all participants provided signed informed consent. Patients We tested 30 patients with El Bagre-EPF and 30 healthy controls (HCs) from the endemic area, matched by age, sex and employment activities. The patients were evaluated clinically, and biopsy samples were assessed by haematoxylin and eosin (H&E) histology, direct immunofluorescence (DIF), immunohistochemistry, confocal microscopy (CFM), ELISA, immunoblotting (IB) and immunoprecipitation (IP), as previously described.7–10 For DIF, biopsies were taken from perilesional skin on the chest; control biopsies were also obtained from the chest. Patients were included only after these tests were performed and if they fulfilled full diagnostic criteria for El Bagre-EPF: (i) the patient had the clinical and epidemiological features described for this disease; (ii) they lived in the endemic area; (iii) their serum displayed intercellular staining of the cell junctions (desmosomes) between epidermal keratinocytes (ICS) by DIF, and to the basement membrane zone (BMZ) of the skin by either DIF or indirect immunofluorescence (IIF), using fluorescein isothiocyanate (FITC)conjugated monoclonal antibodies to human total IgG or to IgG4, as previously described;11,12 (iv) their serum was positive by IB for reactivity against Dsg1 and plakin molecules, as previously described;6 (v) their serum immunoprecipitated a concanavalin A affinity-purified antigen bovine tryptic 45 kDa fragment of Dsg1;13 and (vi) the patient serum yielded a positive result using an ELISA when screening for autoantibodies to pemphigus foliaceus (PF) antigens.14 HC sera were assessed by the same tests. ª 2017 British Association of Dermatologists Direct immunofluorescence DIF was performed as previously described.7–10 The slides were counterstained with 4,6-diamidino-2phenylindole (DAPI) (Pierce, Rockford, IL, USA). Several years ago, the first author discovered new autoantigens to several organs other than the skin. Because of the complexity of the immune response in these patients, we contacted other experts including Dr E. H. Beutner in the USA, Dr T. Hashimoto in Japan and a scientist at the University of Heidelberg in Germany. All agreed that our data indicated new autoantigens. We sent identical serum for study to these scientists; all agreed this disorder was unique. A few months later, the primary owner of Progen Biotechnik (Heidelberg, Germany) commercialized these antibodies. Thus, we used the following antibodies from Progen: anti-ARCVF (Armadillo repeat gene deleted in velo-cardio-facial syndrome; cat. no. GP155), anti-desmoplakin (DP)1 and DP2 (cat. no. 65146), anti-p0071 (cat. no. 651166), and anti-MYZAP (myocardium-enriched zonula occludens1-associated protein; cat. no. 651169). Secondary antibodies were obtained from ThermoFisher Scientific (Waltham, MA, USA), for ARCVF we used Alexa Fluor 555 goat anti-guinea pig, while for DP1 DP2, p0071 and MYZAP, we used goat antimouse Texas Red-conjugated IgG. We also used rabbit anti-junctional adhesion molecule 1 (JAM-A) (ThermoFisher Scientific), as this antibody is positive against gap junctions present in APM. All experiments were performed with positive and negative control samples. Immunohistochemistry Immunohistochemistry performed as previously described.7–11 We tested for mouse anti-human ribosomal protein s6-ps240 (RIBO), and anti-metallothionein (both Dako, Carpinteria, CA, USA). We also used antihuman IgG antibody (Dako) as it is specific for APM. To confirm the identity of the APM, we used an antibody to smooth muscle antigen (SMA) (Dako), which stains APM. Immunoblotting For IB substrates, we used normal human skin from reduction plastic surgeries. For control samples, we used antibodies against DP1, DP2 and Dsg1.6,12–14 IB was performed using an enhanced chemiluminescence set (SuperSignal; ThermoFisher Scientific) on 4%, 7% Clinical and Experimental Dermatology (2017) 42, pp874–880 875 Autoantibodies in a new variant of endemic pemphigus foliaceus A. M. Abreu-Velez et al. and 14% precast gels (Invitrogen, Carlsbad, CA, USA). Samples were separated by both 4% and 7% SDSPAGE according to the Laemmli method, and transferred to PVDF membranes as previously described.6,12–14 Colocalization of the patient autoantibodies with commercial antibodies under confocal microscopy CFM colocalization analysis is often used to determine whether two molecules associate with the same cell structures; for example, to determine whether two particular proteins or molecules both display intracellular colocalization to a specific organelle. CFM was performed as previously described.10,11 In brief, we used standard 9 20 and 9 40 objective lenses; each photo frame included an area of approximately 440 9 330 lm. Images were obtained using image analysis software (EZ-1; Nikon, Tokyo, Japan). For colocalization experiments with serum autoantibodies, we used the aforementioned Progen antibodies to D1, D2, ARVCF, p0071 and MYZAP. Statistical analysis Statistical analysis was performed using GraphPad QuickCalcs (GraphPad Software Inc., La Jolla, CA, USA). We used the Fisher exact test to compare two nominal variables (e.g. positive and negative) of antibody response. P < 0.05 was considered statistically significant. Immunohistochemistry showed positivity against RIBO in 27 of the 30 patients (90%), whereas negative staining was noted in all the HCs (P < 0.001, Fisher exact test). In addition, 25 of the patients displayed reactivity to anti-metallothionein, which was negative in all HCs (83.3% vs. 0%) (P < 0.001, Fisher exact test). The identity of the APM was verified using anti-SMA (Fig. 1). Using histopathological examination with H&E stain, no noticeable changes were seen in the APM, with the exception of a few lymphocytes and histiocytes around these muscles (Fig. 1f). Immunoblotting All patient sera that had positive DIF results for APM also displayed IB colocalizations of their autoantibody molecular weights with the antibodies (all Progen) to DP1 (360 kDa), DP2 (260 kDa), p0071 (135 kDa) ARVCF (105 kDa) and MYZAP (54 kDa) (P < 0.001) (Fig. 1). Confocal microscopy CFM showed that in 27 of the 30 patient sera, the patient autoantibodies colocalized exactly with the antibodies to MYZAP, ARVCF, DP1, DP2 and p0071 (P < 0.001, Fisher exact test). The positive staining also colocalized with the JAM-A control antibody for gap cell junctions (100% vs. 10% respectively, P < 0.001, Fisher exact test) (Fig. 2). Discussion Results Staining results DIF results are shown in Table 1 and Fig. 1. Positive staining for all the antibodies also colocalized with the JAM-A control antibody for gap cell junctions. No control tissues were positive. During our previous DIF studies on patients with El Bagre-EPF,6,7 we observed disease reactivity to APM. In the current study, we specifically tested for APM reactivity and found a polyclonal immune response. We had previously documented a polyclonal response against other structures.6–11 APM is composed of smooth muscle and has many gap junctions. For the Figure 1 Colocalization of antibodies from patients with El Bagre endemic pemphigus foliaceus (EPF) and the commercial antibodies to Armadillo repeat gene deleted in velo-cardio-facial syndrome (ARCVF), desmoplakin (DP), p0071 and myocardium-enriched zonula occludens-1-associated protein (MYZAP) in arrector pili muscle (APM). (a) Direct immunofluorescence (DIF) shows colocalization of p0071 (red/yellow staining) and fluorescein isothiocyanate (FITC)-conjugated anti-human IgG patient antibodies (green staining) (black arrow) (original magnification 9 400). (b) Immunohistochemistry (IHC) shows positive (brown) staining for IgG in patient APM (black arrow) (original magnification 9 200). (c) DIF shows positive (green) with FITC-conjugated anti-human IgG in patient APM (white arrows) (original magnification 9 100). (d) IHC shows positive (brown) staining for human ribosomal protein s6-ps240 (RIBO), in APM (black arrow) (original magnification 9 400). (e) Histology showing a lymphohistiocytic infiltrate around a patient APM (black arrows) (haematoxylin and eosin, original magnification 9 40). (f) Immunoblotting results: Lanes A and B progressing right indicate sera from a patient with El Bagre-EPF; lane C, negative control; lane D, positive controls Note the positive staining from top to bottom: 360 kDa (DP1) 260 kDa (DP2), 160 kDa (Dsg1), 135 kDa (p0071), 105 kDa (ARVCF), 67 kDa (unknown), 54 kDa (MYZAP) and 47 KDa (unknown). 876 Clinical and Experimental Dermatology (2017) 42, pp874–880 ª 2017 British Association of Dermatologists Autoantibodies in a new variant of endemic pemphigus foliaceus A. M. Abreu-Velez et al. (a) (c) (e) ª 2017 British Association of Dermatologists (b) (d) (f) Clinical and Experimental Dermatology (2017) 42, pp874–880 877 Autoantibodies in a new variant of endemic pemphigus foliaceus A. M. Abreu-Velez et al. Table 1 Results of direct immunofluorescence staining of arrector pili muscle. Marker Positive cases, n* IgG Fibrinogen Albumin Complement/C3c Complement/C1q IgA IgD IgE 27 20 13 9 8 9 9 0 Staining strength ++++ ++++ +++ +++ ++ ++ ++ – *Out of 30. disease fogo selvagems, the Portuguese medical literature prior to the introduction of steroids includes postmortem studies documenting pathological findings in smooth muscle of the stomach, intestine, ocular ciliary muscles, urinary bladder and blood vessels.15,16 Our findings are thus in agreement with these early fogo selvagem results regarding smooth muscle reactivity. At least one-third of patients with El Bagre-EPF have systemic autoreactivity, and we are in the process of documenting these new data. In the current study, we found that 90% of the patients with El Bagre-EPF displayed autoantibodies to APM. APM is responsible for piloerection, and we previously showed that patients with El Bagre-EPF have autoantibodies to the pilosebaceous units and that these antibodies colocalize with ARVCF, p0071, DP1 and DP2 antibodies, which are all present in the cell junctions.7 At the time we reported those findings, our samples did not display significant APM reactivity; we later collected additional samples. In the current study, we found autoantibodies Figure 2 (a) Direct immunofluorescence (DIF) using fluorescein isothiocyanate (FITC)-conjugated anti-human IgG (green), epidermal intercellular staining (red arrow) and staining along the basement membrane zone (BMZ) (yellow arrow) and in arrector pili muscle (APM) (black arrow) (original magnification 9 100). (b) DIF using FITC-conjugated anti-human IgG (green staining) colocalizing with myocardium-enriched zonula occludens-1-associated protein (MYZAP) (red/yellow staining) in patient APM (black arrow). (c) Immunohistochemistry shows positive (brown) staining with IgG against patient APM (red arrow) (original magnification 9 400). (d) Verification that this tissue was APM was performed using smooth muscle antigen antibody (brown staining) (original magnification 9 400). 878 Clinical and Experimental Dermatology (2017) 42, pp874–880 ª 2017 British Association of Dermatologists Autoantibodies in a new variant of endemic pemphigus foliaceus A. M. Abreu-Velez et al. to APM in patients with El Bagre-EPF. We are not aware of any clinical implications of our current findings. We had also shown previously that these commercial antibodies from Progen colocalized exactly with structures in the heart, including the Purkinje system and heart cell junctions.8 These findings suggested that the specific molecules that belong to the 120 (catenin)/plakophilin subfamily of Armadillo-like proteins (i.e. ARVCF and p0071) are El Bagre-EPF autoantigens. ARVCF, DP1, DP2, and p0071MYZAP are components of cell junctions in most parts of the body. This is supported by our results here, as their reactivity colocalized with the JAM-A control antibody for gap junctions; these colocalizations were confirmed by confocal microscopy, and the molecular weight of these proteins was similar to those of El Bagre-EPF autoantigens. In the current study, we also found that RIBO and metallothionein were overexpressed in APM, indicating a pathological process.17 Metallothioneins represent a family of cysteine-rich, low molecular weight proteins18 that bind both pathological and xenobiotic heavy metals through the thiol group of their cysteine residues. We previously reported that patients with El Bagre-EPF live in an area with high levels of xenobiotics such as mercuric selenides, iodine, heavy metals and metalloids, and they are also exposed to materials used in cocaine processing, such as permanganate, sulphuric acid, caustic sodium ammonium sulphate and lime.18 APM are rich in enzymes; some, including acetylcholinesterase, are inhibited by mercury. Acetylcholine is one of the primary neurotransmitters of nerves in the autonomic nervous system.19 We previously documented that patients with El Bagre-EPF are exposed to high environmental levels of mercury,18 and in other studies, that autoantibodies in patients with El Bagre-EPF were present in smooth muscle areas, nerve receptors and pilosebaceous unit tissue.7–9 In a previous study of 72 patients with dermatitis herpetiformis, IgA was observed in 19 cases in the APM, and, in a few cases, complement/C3, IgM, and IgG were also identified.20 This indicates that the auto-reactivity to APM is important in other autoimmune blistering diseases. We have previously shown that DP1, DP2 and members of the p120 (ctn)/plakophilin subfamily of Armadillo-like proteins (ARVCF and p0071) are recognized by the autoantibodies from patients with El Bagre-EPF.7,8 All these molecules are part of cell junctions in multiple human organs.19,21 MYZAP has ª 2017 British Association of Dermatologists recently been identified as a component of the cytoplasmic plaques of the area composita of myocardial intercalated disks, and in the adherens junctions in vascular endothelia. Most patients with El Bagre-EPF have autoantibodies to these structures. We have also previously demonstrated that the immune response in patients with El Bagre-EPF is polyclonal, and that it includes B and T lymphocytes, mast cells, IgG, IgA, IgM, IgD, IgE, fibrinogen, albumin, complement/C1q, C3c, and C4.7–14 The El Bagre–EPF disease focus differs from other foci of EPF. Patients with El Bagre-EPF are exposed to tropical and parasitic disease agents including malaria (both Plasmodium vivax, and Plasmodium falciparum), tuberculosis, Hirudinea spp., Haementeria spp., Glossiphoniidae spp., Oxytychus ornatus, Enterobacter cloacae, Bordetella bronchiseptica, Enterococcus faecalis, Klebsiella oxytoca and Klebsiella pneumoniae. They are also exposed to multiple metals and metalloids, which may explain the polyclonal immune response. In the current study, we found that patients with El Bagre-EPF had reactivity to APM, which colocalized with the commercial antibodies DP1, DP2, ARVCF, MYZAP and p0071; these may represent putative new antigens in patients with El Bagre-EPF. All these molecules are components of cell junctions, indicating that the immune response is possibly directed, at least partially, against these structures. As noted previously, APM contain multiple enzymes, including acetylcholinesterase. Moreover, these enzymes may be altered by mercury and other metals and metalloids that prevail in the endemic area; these enzymes may also be altered by chemicals used in cocaine processing. Conclusion We have identified a new variant of EPF in El Bagre, Colombia, South America, which we term El BagreEPF (also called pemphigus Abreu–Manu) and detected a polyclonal reactivity to APM and its cell junctions, indicating that the immune response in this variant of pemphigus is not only directed to the desmosomal antigens but also to smooth muscle cells and their junctions. The implications of these results for immune response triggers still remain unsolved and warrant further study. Acknowledgements We thank J. S. Jones, HT (ASCP), Georgia Dermatopathology Associates, for excellent technical assistance. This study was supported financially by Georgia Clinical and Experimental Dermatology (2017) 42, pp874–880 879 Autoantibodies in a new variant of endemic pemphigus foliaceus A. M. Abreu-Velez et al. Dermatopathology Associates (Atlanta, GA, USA); Mineros SA (Antioquia, Colombia); Embassy of Japan (Colombia) Municipality of El Bagre (Antioquia, Colombia) and Hospital Nuestra Se~ nora de El Bagre (Antioquia, Colombia). What’s already known about this topic? 10 11 • Patients with EPF have autoantibodies to epi- dermal keratinocyte cell junctions. 12 What does this study add? 13 • Patients with El Bagre-EPF have autoantibodies to APM. • These antibodies colocalize with antibodies to ARVCF, DP1, DP2, p0071 and MYZAP. 14 References 1 Anhalt GJ, Martins C, Rivitti E et al. Endemic pemphigus foliaceus (fogo selvagem). Adv Dermatol 1989; 4: 73–93; discussion 94. 2 Ortega-Loayza AG, Ramos W, Gutierrez EL et al. Endemic pemphigus foliaceus in the Peruvian Amazon. Clin Exp Dermatol 2013; 38: 594–600. 3 Abreu-Velez AM, Messias-Reason LJ, Howard MS et al. Endemic pemphigus foliaceus over a century: part 1. N Am J Med Sci 2010; 2: 51–9. 4 Abreu-Velez AM, Roselino AM, Howard MS et al. Endemic pemphigus foliaceus over a century: part 2. N Am J Med Sci 2010; 2: 114–25. 5 Morini JP, Jomaa B, Gorgi Y et al. Pemphigus foliaceus in young women. An endemic focus in the Sousse area of Tunisia. Arch Dermatol 1993; 129: 69–73. 6 Hisamatsu Y, Abreu-Velez AM, Amagai M et al. Comparative study of autoantigen profile between Colombian and Brazilian types of endemic pemphigus foliaceus by various biochemical and molecular biological techniques. J Dermatol Sci 2003; 32: 33–41. 7 Abreu-Velez AM, Howard MS, Smoller BR. Antibodies to pilosebaceous units, in a new variant of pemphigus foliaceus. Eur J Dermatol 2011; 21: 371–5. 8 Abreu-Velez AM, Zhe J, Howard MS et al. Heart immunoreactivity in patients affected by a new variant of endemic pemphigus foliaceus in El-Bagre, Colombia, South America. J Clin Immunol 2011; 31: 985–97. 9 Abreu-Velez AM, Howard MS, Grossniklaus HE et al. Neural system antigens are recognized by autoantibodies 880 Clinical and Experimental Dermatology (2017) 42, pp874–880 15 16 17 18 19 20 21 from patients affected by a new variant of endemic pemphigus foliaceus in Colombia. Clin Immunol 2011; 31: 356–68. Abreu-Velez AM, Howard MS, Hashimoto K et al. Autoantibodies to sweat glands detected by different methods in serum and in tissue from patients affected by a new variant of endemic pemphigus foliaceus. Arch Dermatol Res 2009; 30: 711–18. Abreu-Velez AM, Beutner EH, Montoya F et al. Analyses of autoantigens in a new form of endemic pemphigus foliaceus in Colombia. J Am Acad Dermatol 2003; 49: 609–14. Abreu-Velez AM, Hashimoto T, Bollag WB et al. A unique form of endemic pemphigus in Northern Colombia. J Am Acad Dermatol 2003; 4: 599–608. Abreu-Velez AM, Javier Pati~ no P, Montoya F et al. The tryptic cleavage product of the mature form of the bovine desmoglein 1 ectodomain is one of the antigen moieties immunoprecipitated by all sera from symptomatic patients affected by a new variant of endemic pemphigus. Eur J Dermatol 2003; 4: 359–66. Abreu-Velez AM, Yepes MM, Pati~ no PJ et al. A costeffective, sensitive and specific enzyme linked immunosorbent assay useful for detecting a heterogeneous antibody population in sera from people suffering a new variant of endemic pemphigus. Arch Dermatol Res 2004; 295: 434–41. Vieira JP. Novas Contribuicß~oes ao Estudo do P^enfigo Foliaceo (Fogo-selvagem) no Estado de S~ao Paulo. S~ ao Paulo: Empresa Gr afica da Revista dos Tribunais, 1940. ~o ao estudo do p^enfigo foli Silva F. Contribuicßa aceo. Brasil Medico 1938; 87: 1–7. Abreu-Velez AM, Googe PB Jr, Howard MS. Ribosomal protein s6-ps240 is expressed in lesional skin from patients with autoimmune skin blistering diseases. N Am J Med Sci 2013; 5: 604–8. Abreu-Velez AM, Warfvinge G, Leon-Herrera W et al. Detection of mercury and other undetermined materials in skin biopsies of endemic pemphigus foliaceus. Am J Dermatopathol 2003; 25: 384–91. Pieperhoff S, Rickelt S, Heid H et al. The plaque protein myozap identified as a novel major component of adhering junctions in endothelia of the blood and the lymph vascular systems. J Cell Mol Med 2012; 16: 1709–19. Barnadas MA. Dermatitis herpetiformis: a review of direct immunofluorescence findings. Am J Dermatopathol 2016; 38: 283–8. Franke WW, Borrmann CM, Grund C et al. The area composita of adhering junctions connecting heart muscle cells of vertebrates. I. Molecular definition in intercalated disks of cardiomyocytes by immunoelectron microscopy of desmosomal proteins. Eur J Cell Biol 2006; 85: 69–82. ª 2017 British Association of Dermatologists


![[BRACKETS INCLUDE SUGGESTED INFORMATION THAT MAY BE INCREASED] DEPARTMENT OF FORESTRY](http://s2.studylib.net/store/data/013068471_1-cfecf471b59af83eb9fbee25e61f8411-300x300.png)