The British Association of Plastic Surgeons (2003) 56 , 528–533
New split scar cheek flap in reconstruction of noma sequelae
q
Department of Otolaryngology, Head and Neck Surgery, University of Regensburg, Franz-Josef-Strauß-
Allee 11, D-93042 Regensburg, Germany
Received 30 January 2003; accepted 2 June 2003
KEYWORDS
Cancrum oris; Noma;
Reconstruction; Split scar flap; Results
Summary The use of a split-scar cheek flap is demonstrated for restoration of lining in reconstructing the oral commissure in cases of noma.
Q
2003 The British Association of Plastic Surgeons. Published by Elsevier Ltd. All rights reserved.
Introduction
Cancrum oris or noma is a devastating ulcerativenecrotising gingivo-stomatitis which affects primarily undernourished and immunosuppressed young
Noma, if not fatal in the first place leads to severe destruction of the mid-face, including lips and cheek, maxilla, mandible, nose and, in rare cases, the orbit. Whilst antibiotic treatment is essential and effective in the initial stage of the disease, the process will progress to noma by transmission to the soft tissues in contact with the gingival lesions if left untreated. In the end, the afflicted are left with gaping holes in their faces.
Without appropriate treatment, the mortality rate reaches 70 – 90% (WHO 1994).
The most common soft tissue defect in noma is full thickness loss of the cheek, involving the lateral parts of the lips.
The surgical strategy aiming at these cheek and lip defects is central to the presented study.
To achieve a good and lasting functional result, q
The paper has been presented at the 72nd Annual Meeting of the German ORL society.
*Corresponding author. Tel.: þ 49-941-944-9440; fax: þ 49-
941-944-9441.
E-mail address: thomas.kuehnel@klinik.uni-regensburg.de
an epithelium lining of the oral cavity is mandatory.
The defects require a three-layer closure, and an inner lining must be created.
The application of a new flap for reconstruction of soft tissue defects in noma patients developed and carried out in the years 1997, 1998 and 2000 is described. It is a procedure that suits the requirements of the host country and provides favourable functional and aesthetic results. The method described can predictably rehabilitate patients with noma defects of the cheek and lateral lips in a single operative setting. The use of the split scar cheek flap is illustrated, while functional and aesthetic impact is emphasised. If the cases are appropriate, we wish to recommend the technique described as an alternative to micro-vascular or pedicled tissue transfers.
Patients and methods
Patients who, after noma disease, were left with a soft tissue defect of the chin and commissure, chronic functional impairment with speech restriction, salivary leakage or inability to achieve adequate food intake or social disadvantages due
S0007-1226/03/$ - see front matter
Q
2003 The British Association of Plastic Surgeons. Published by Elsevier Ltd. All rights reserved.
doi:10.1016/S0007-1226(03)00225-X
New split scar cheek flap in reconstruction of noma sequelae 529 to cosmetic deformity were enrolled in this prospective clinical study. Exclusion criteria were acute disease and trismus. Informed consent was given by all patients and parents, respectively. The study was performed according to the declaration of Helsinki/Tokio at the Department of General
Surgery Hopital National de Niamey in the Republic of Niger. We included two male and five female
African children, ranging in age from four to 20 years with a mean age of 11.
An accurate assessment of every case was achieved, including examination by ENT- and maxillofacial surgeons and anaesthetists. Documentation and Op-plannings were performed with the help of digital photography and patients received preoperative nutritional preparation for
3 – 7 days. The features recorded were: age and gender of patients, size of the defects including adjacent scar, comorbidity and expectations of the patient concerning the aesthetic result of surgery, operation time per patient, length of postoperative hospital stay, postoperative nutrition stage improvement and subjective cosmetic results. As stated before,
the aim of this study was to allow the patients to achieve an adequate level of selfnutrition.
Anaesthesia
Endotracheal intubation and general anaesthetic were employed in all cases. A 4 mm fibreoptic endoscope proved helpful for nasotracheal intubation. Induction was performed with thiopentone or ketamine/midazolam sedation when fibrescopic intubation was used. Anaesthesia was maintained by halothane (due to the vaporisers available at the hospital) supplemented by analgetic doses of ketamine. No anaesthetic complications occurred.
Operative technique
After the onset of anaesthesia the steps of surgery, modified by Montandon,
were carried out as follows: local infective foci were removed by extraction of infected or displaced teeth, sequesters or scabs. Then the commissure was reconstructed. At this stage of the operation, the amount of soft tissue necessary for reconstruction may be estimated precisely. Before finally closing the defect of the cheek, the continuity of the inner lining in the oral cavity was reconstructed with the help of the split scar flap utilising the facial scar, which was split in half. The cases demonstrated required special consideration of the vestibulum. It had to be reconstructed, as the parietal layer had been destroyed by Noma disease.
The split scar flap
The surgical strategy is comprised of three steps in principal:
1. Closure of the commissure or lip defects
2. Construction of an ‘inner lining’ using the split scar cheek flap
3. Closure of the cheek ‘outer lining’ using local flaps
1. The scar resulting from Noma is detached from the parts of the lips in sound condition. For a satisfying functional result, continuity of the orbicularis oris muscle has to be obtained.
Reconstruction is carried out by either using an
‘Estlander’-transposition flap or primarily joining the isolated stumps of the muscle.
In the case of a blunt commissure resulting from this technique, a commissuroplasty has to be performed in a second step.
2. Instead of radical excision of the scar, which is the common practice,
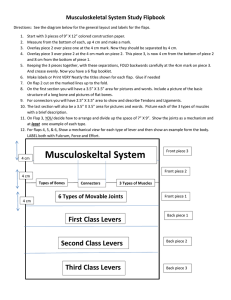
the scar is used to construct the ‘inner lining’. An incision throughout half of the layer is performed in the dorsal margin of the scar (
Fig. 1 ). Preparation proceeds in this plane
almost to the free rim of the scar anteriorly next to
the commissure ( Fig. 2 ). In doing so, the scar is split
in half. Caution has to focus on the basis of the flap.
As the blood supply to the scar is poor anyway, it has to be even broader than in common local transposition flaps. The lateral, mobile part of the flap is turned forward and is fixed to the commissure and to the gingival mucosa (
For satisfying functional results, a sufficient deep oral cavity has to be designed. Any excess of scar tissue may be removed at this time. The defect is now covered by a first layer with its epithelium facing the oral cavity (
3. Next, the outer defect is covered with local transposition flaps which originate from the submental, cervical and/or nasolabial region.
Results
Postoperative healing was uneventful in all cases.
Swallowing was re-established within a week.
Aesthetic results are shown in
. Trismus caused by scarring associated with a new increase of functional deficits was not seen during a 1-year follow-up period. Operation time was 2 – 4 h per patient, while the postoperative hospital stay was eight to 10 days. Moreover, postoperative nutrition levels in all seven patients showed a clinically significant improvement. All patients were highly satisfied with their aesthetic results.
530
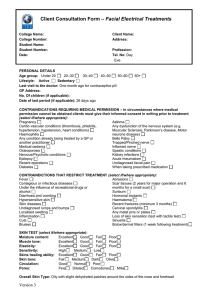
Fig. 1 Child with full thickness defect of the left cheek and lateral lips. Preoperative show. (A) Drawing, (B) photograph.
Fig. 2 The drawing (A) shows the flap split in half layer thickness, mobilised and turned forward. (B) Development of the split scar cheek flap anteriorly. To be closed just beneath the nasolabial fold. Intraoperative aspect.
New split scar cheek flap in reconstruction of noma sequelae 531
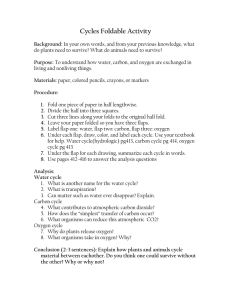
Fig. 4 Detail of oral vestibulum: reconstruction of inner lining with split scar.
Discussion
Noma or cancrum oris is a disease primarily found in
developing countries afflicting young children.
Poverty, concluding malnutrition, faecal contamination of foods and water supplies and poor oral hygiene are the predominant risk factors.
Fig. 3 Defect just before closure. Mobilisation of the local transposition flap to be added.
Long-term follow-up was accomplished by health year after the operations. No complications and no new scar formation to disabling extent was reported.
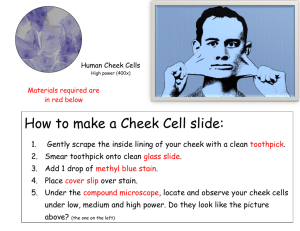
Fig. 5 Postoperative result (10th day).
532
Fig. 6 Preoperative aspect of another patient, operated in a similar manner.
Besides social rejection, the affected children are handicapped in terms of food intake and speech production. Since awareness of surgical options is more common nowadays, an increasing number of patients opt for plastic reconstruction.
Preven-
Fig. 7 Postoperative aspect of another patient, operated in a similar manner.
tion of the disease is technically simple but until socio-economic conditions improve, the disease will continue to occur. Factors which would help to prevent cancrum oris include the education of parents, the availability of protein rich food, dental healthcare and measles vaccinations, to address the most important items.
Consequences of the disease are both aesthetic and functional.
After having survived the acute disease, patients suffer from immense scarring and impairment of self-nutrition. Due to individual defects, sophisticated reconstructive surgery requires a wide spectrum of operative techniques in order to suit individual cases. No single standard is sufficient for all types of defects.
Reconstruction in cancrum oris sequelae is complex and is looked upon as a surgical challenge that requires a hospital equipped with the latest technology, which is not always achievable in the origin countries.
Local flaps provide excellent colour and texture match
and are recommended for a one-stage method because of their short postoperative course. Furthermore, one-stage methods of treatment offer several advantages: first, economising expenses is an urgent requirement in the treatment of these patients, who are all being treated on a charity basis. Second, due to local implications return to a hospital turns out to be very difficult due to there being great distances between the patients’ homes and the hospitals. Third, a short operation time means less physical stress and risk of postoperative wound infection. Complicated by the typical conditions of malnutrition, these aspects become of greatest value. To prevent complications, the patients in this study underwent adequate preoperative nutritional preparation prior to reconstructive surgery. A split scar flap using the scar as the inner lining of the oral cavity was implemented in soft tissue defects of the cheek and lateral portion of the lips. Postoperative recovery proved to be uneventful in all cases and patients returned to their families within 10 days. In detail, though the scar has a seriously impaired blood supply, it is capable of establishing an inner lining if covered by healthy tissue.
To prevent recurrence of functional impairment by scarring, an inner lining of the oral cavity is mandatory. As experience shows, a two layer closure by mere transposition flaps is not adequate.
We introduce an alternative to microvascular tissue transfers, pedicled and prefabricated flaps; our alternative features a short operating time, low surgical morbidity and excellent functional and aesthetic results.
In contrast to prior publication,
by integrating the scar into the operative concept we succeeded in
New split scar cheek flap in reconstruction of noma sequelae 533 creating an inner lining that could be covered with local flaps in all cases.
The aesthetic and functional results in these cases compare favourably with those reported using musculocutaneus flaps, such as pectoralis major and latissimus dorsi flaps
References
1. Lazarus D, Hudson DA. Cancrum oris—a 35-year retrospective study.
S Afr Med J 1997; 87 :1379—82.
2. Enwonwu CO, Falkler WA, Idigbe EO, et al. Noma: a neglected scourge of children in sub-Saharan Africa.
Am J
Trop Med Hyg 1999; 60 :223—32.
3. Enwonwu CO. Infectious oral necrosis (cancrum oris) in
Nigerian children: a review.
Community Dent Oral Epidemiol
1985; 13 :190—4.
4. Montandon D, Pittet B. Humanitarian plastic surgery.
Personal experience and reflections.
Ann Chir Plast Esthet
1999; 44 :27—34.
5. Tempest MN. Cancrum oris.
Br J Surg 1966; 53 :949—69.
6. Sawyer DR, Nwoku AL. Cancrum oris (noma): past and present.
ASDC J Dent Child 1981; 48 :138—41.
7. Adolph HP, Yugueros P, Woods JE. Noma: a review.
Ann Plast
Surg 1996; 37 :657—68.
8. Adekeye EO, Lavery KM, Nasser NA. The versatility of pectoralis major and latissimus dorsi myocutaneous flaps in the reconstruction of cancrum oris defects of children and adolescents.
J Maxillofac Surg 1986; 14 :99—102.
9. Adekeye EO, Ord RA. Cancrum oris: principles of management and reconstructive surgery.
J Maxillofac Surg 1983; 11 :
160—70.
10. Dean JA, Magee W. One-stage reconstruction for defects caused by cancrum oris (noma).
Ann Plast Surg 1997; 38 :
29—35.
11. Durrani KM. Surgical repair of defects from noma (cancrum oris).
Plast Reconstr Surg 1973; 52 :629—34.
12. Barmes DE, Enwonwu CO, Leclercq MH, et al. The need for action against oro-facial gangrene (noma) [editorial].
Trop
Med Int Health 1997; 2 :1111—4.
13. Montandon D, Lehmann C, Chami N. The surgical treatment of noma.
Plast Reconstr Surg 1991; 87 :76—86.
14. Calhoun KH. In: Calhoun KH, Stiernberg CM, Bailey BJ, Holt
GR, editors.
Sugery of the lip , 1st ed. New York: Thieme;
1992. p. 42—8.
15. Adams RW, James JH. Cancrum oris: functional and cosmetic reconstruction in patients with ankylosis of the jaws [see comments].
Br J Plast Surg 1992; 45 :193—8.
16. Evrard L, Laroque G, Glineur R, Daelemans P. Noma: clinical and evolutive aspect.
Acta Stomatol Belg 1996; 93 :17—20.
17. Horning GM. Necrotizing gingivostomatitis: NUG to noma.
Compend Contin Educ Dent 1996; 17 :951—8.
18. Erdmann D, Schierle H, Sauerbier M, Germann G, Lemperle
G. [Reconstruction of severe facial defects due to noma].
Chirurg 1998; 69 :1257—62.