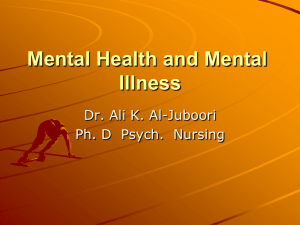
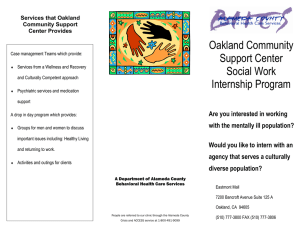
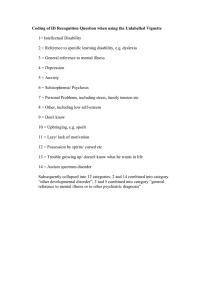
State Psychiatric Hospitals An Analysis of Political Economy John S. Hirschauer, Fairfield University Economics Class of 2018 “[The psychiatrist’s] counsel is one of intellectual amputation. If thy head offend thee, cut it off; for it is better, not merely to enter the Kingdom of Heaven as a child, but to enter it as an imbecile, rather than with your whole intellect to be cast into hell — or into Hanwell.” -G.K. Chesterton ❖ Preface It is fashionable to speak today of “mental health issues” as a gentle synonym for the myriad of overwrought emotional responses to everyday stressors that are formed, at least in part, by a generation of handwringing parents and their self-obsessed children. The purpose of this paper is not to examine the status of our nation’s “mental health”- we have entire government agencies dedicated to fighting such euphemistic battles- but rather to examine plainly the state hospital network and its various malcontents in the lens of political economy, and the lot of Americans with schizophrenia and other serious mental illnesses who utilize these services. There is not much in the piece to follow that one must take as axiomatic, but the following two assumptions flow logically out of the piece’s body and conclusion: first, a rejection of the Szaszian insistence that mental illness is a socially constructed reality and psychiatry is an exercise in disparate power dynamics, and second, that the greatest (or even a significant) barrier to treating the severely mentally ill is publicly installed “stigma” or a derivative species of self-flagellation that castigates society, particularly Western society, at large for the troubles of its ill. There is supply aplenty for such academic works of public derision, but this piece will not traffic in such questions. It seems to be a broad perception among Americans that state hospitals are something we have nationally discarded and that all of the mentally ill have been “deinstitutionalized.” The fact remains that almost every state still runs one or more state psychiatric hospitals that serve ever-dwindling populations, and their current stasis provides fascinating data points for the economist to examine questions of economies of scale, political economy, health economics, public finance, and more. I will be utilizing my own original research in tandem with data collected from the Treatment Advocacy Center, a non-profit dedicated to advocating for public policy surrounding the treatment of the severely mentally ill, and the book published by its founder Dr. E. Fuller Torrey, M.D. entitled American Psychosis: How the Federal Government Destroyed the Mental Illness Treatment System. Torrey’s work is littered with studies and cost analyses that will contribute to the conclusion and exposition undertaken in this piece. Underlying Economic Realities of Treating the Mentally Ill The Nature of Severe Mental Illness Before examining the economic factors in question surrounding funding and care delivery in the state mental facility, one must reasonably establish the principal economic and philosophical bases for mental illness treatment more broadly. Taken as an exogenous reality, mental illness and the corresponding need to treat those affected with it were the prima facie justification for the state hospital’s invention in the 19th century.1 What most profoundly distinguishes the care of the mentally ill from treating its somatic counterparts is the lack of agency many mentally ill individuals retain in the provision of their own care. This lack of agency is made manifest in two ways, both having the similar effect of either obscuring the demand signals that would trigger private intervention or fiscally precluding an individual from being able to afford the care they would otherwise require. Some seriously mentally ill persons, particularly ones with various schizoaffective conditions, have a comorbid affliction known as anosognosia, which prevents them from 1 History.com Staff. "Dorothea Lynde Dix." History.com. 2009. Accessed May 09, 2018. https://www.history.com/topics/womens-history/dorothea-lynde-dix. recognizing that they are sick. Patients with afflictions of all types, be they somatic or psychiatric, with an ability to recognize their illness will, in the gradated arc of their illness’ severity, reach a point of perfect inelasticity (and will often sooner reach a point inelastic enough to yield) to their demand for care. Non-anosognosiac patients can signal their demand for care in such a way as to ignite basic market forces to create a correspondent supply to match the demand for services- for instance, orthopedic specialists enter their chosen field precisely because there are individuals with broken bones demanding a remedy. Private actors have no fiduciary incentive to create treatment centers explicitly designed for individuals who have no idea they need treatment, and in the absence of some method of involuntary commitment those individuals will not seek treatment even were it provided free of charge. The second confounding reality of treating the seriously mentally ill is the debilitating nature of the disease. This problem is not unique to those with psychiatric conditions, of course, but can have a particularly vicious incidence in the population with severe mental illness. Any disease that totally incapacitates a person almost certainly reduces (if not eliminates) their ability to be productive in any economic capacity. Able economic actors acting rationally will take out insurance, create a private savings account for “rainy days” or engage in other methods of smoothing their consumption curves given the possibility of falling victim to catastrophe. Individuals without this period of “ability”- specifically those whose incapacitation begins in childhood, before they are fully capable of taking responsibility for attaining instruments to smooth consumption in the event of catastrophe- are dependents upon either their immediate families or the state. For some severely mentally ill individuals, their life arc is often such that attaining functional competence is never completely possible. It is believed that severe mental illnesses like schizophrenia, bipolar disorder, autism, and forms of obsessive-compulsive disorder and melancholic depression are neuropsychiatric conditions- brain conditions much like Parkinson’s or epilepsy- in nature that often affect individuals from a young age, in antecedence of an age of accountability. 23 Even late-developing forms of severe mental illness are frequently incapacitating; a sprained ankle or a herniated disc can partially reduce a person’s level of productive functioning, but diseases with features of psychosis can be utterly debilitating, making it difficult for such individuals to ascertain the requisite funds to treat their malady. Economic Fundamentals of Mental Illness Treatment Society, as it stands, has three fundamental options in the face of these realities and the broader reality of this population’s existence: it can arrange publicly provided care, persons with agency can coordinate care in the private sector, or it can choose to do nothing. Each of these three options has costs associated with them, delineated below: The Public Provision of Care Public provision of treatment for the severely mentally ill induces two primary costs, one explicit and the other implicit. The explicit cost is, of course, the actual monies and resources expended on treatment, and the sum total thereof is neatly available when the receipts are tallied on whatever means of delivery the state chooses. Implicitly, however, the costs associated with any program funded with taxpayer resources can be exorbitant. The first implicit cost is the next-best alternative use of the resources pooled from taxpayers. Other implicit costs- the long-term effects on localities from the imputation of new taxation and/or a mental facility into the local 2 Reidbord, Steven, M.D. "Are Psychiatric Disorders Brain Diseases?" Psychology Today. December 12, 2015. Accessed May 9, 2018. https://www.psychologytoday.com/us/blog/sacramento-street-psychiatry/201512/arepsychiatric-disorders-brain-diseases. 3 Torrey, E. Fuller. American Psychosis: How the Federal Government Destroyed the Mental Illness Treatment System. 141. Oxford University Press, 2014. community on demography and regional income distribution- are more difficult to project than any opportunity cost calculation. The Private Provision of Care The private provision of care for the severe mentally ill is wrought primarily with the issues described in the preceding paragraphs. For those with non-severe or late-developing mental illness, the private market can function in facilitating efficient exchange. In a private market for the treatment of the severely mentally ill, the capacity of the demand side of the market to signal its need for services can be thwarted either partially or entirely by anosognosia, or by the potential benefactors’ inability to reliably pay for the profundity of the care they require. Both make the market relatively impotent in being the exclusive dealer of care for the severely mentally ill, but the right subsidy incentive structure from the state can offset these foundational issues. The underprovision of psychiatric care can have additional external costs as will be described below. Inaction, or Dismissing Market Failures Choosing to dismiss market failures (specifically, the underprovision of services for the severely mentally ill) and choosing to leave them without remedy does save monies otherwise allocated to various services. But inaction has the broader effect of levying society at large with all sorts of costs related to the maladaptive behaviors and lost productivity resultant from the untreated severely ill. For instance, as discussed in Psychosis, it is estimated that the social costs of violent crime committed by the mentally ill is roughly $925,000 per crime. 4 Many of the severely mentally ill, given an appropriate continuum of care and support network, can be productive T.R. Insel, “Assessing the Economic Costs of Serious Mental Illness,” American Journal of Psychiatry 165, no 6 (2008): 663-665; D.E. Marcotte and S. Markowitz, “A Cure for Crime? Psycho-pharmaceuticals and Crime Trends,” Working Paper 15354 (Cambridge, MA: National Bureau of Economic Research, 2009), http://www.nber.org/papers/w15354 (Citation qtd. Torrey, American Psychosis) 4 members of the domestic economy. 5 Abrogating the provision of their care has all sorts of moral warts, but its economic effects are just as profound. Historical Considerations “God save us from people who mean well.” -Vikram Seth ❖ Historic Legislative Trajectory As a means of guiding the exposition to follow, it is worth preemptively characterizing the legislative environment that fueled the public financing changes of the state hospital that we will examine in subsequent paragraphs. The treatment of the mentally ill was a fiscal prerogative of the states, save for St. Elizabeth’s Hospital in Washington, D.C. and narcotics hospitals under federal jurisdiction, until the first domino fell in 1946 with the creation of the National Institute of Mental Health (NIMH), under the broad auspices of “coordinating research relating to neuropsychiatric disorders; to provide for more effective methods of prevention, diagnosis, and treatment of such disorders…and for other purposes.”6 The legislative epoch came in 1963 with President John Kennedy’s Community Mental Health Act, which created a federal system to usurp the previously localized model. “Community mental health” became the new rhetorical elixir; an amorphous concept since its inception, its apotheosis was the “community mental health center” as conceived by one of its ideological parents, Robert Felix: “To be fully effective, a good mental health program must include some provision for social action so that the total community environment is a mentally healthy one. 5 Vaughn Tesei, Jill. "Meeting with Jill Vaughan Tesei APRN." Interview by John S. Hirschauer, Jr. Qtd. Torrey, E. Fuller. American Psychosis: How the Federal Government Destroyed the Mental Illness Treatment System. 23-24. Oxford University Press, 2014. 6 This is particularly important for those areas, such as family life and school experience, which affect the individual most closely.” 7 The question of who would control the direction and bear the fiscal burden of these community mental health centers (CMHCs), was hotly contested at the program’s inception, but by 1965 the federal government was not only subsidizing the creation of these centers but paying staffing costs. States had previously been emptying portions of their state hospitals in response to the advent of psychotropic medication prior to this legislation and were already involved in the creation of programs for discharged patients. A functioning continuum of care was beginning to develop on a state level, with the state hospital still existing as an appendage of that continuum. The advent of federal involvement as both staffer and bursar of top-down solutions frustrated many state mental health directors.8 President Lyndon Johnson’s Great Society initiatives and the creation of federal aid programs like Medicare and Medicaid further warped fiscal incentives for states. This will be discussed further in forthcoming sections. Attempts at sustaining the federal direction of the CMHC program faltered in 1981 when President Ronald Reagan block granted CMHC funding to the states. Federal involvement in treating mental illness would still remain, given the complicating existence of Johnson-era entitlement programs. As Torrey puts succinctly in Psychosis, “Whereas the original state treatment programs had been funded almost exclusively with state and local funds, the emerging treatment system 7 Ibid, Qtd. 47. Torrey, E. Fuller. American Psychosis: How the Federal Government Destroyed the Mental Illness Treatment System. 51-61. Oxford University Press, 2014. 8 included funding by federal Medicaid, Medicare, SSI, SSDI, block grants, food stamps, employment programs, housing, etc.”9 The resultant stasis of care for the mentally ill encompassed a wide spectrum of facilities ranging from nursing homes to halfway houses, CMHCs, state hospitals, psychiatric wards of general hospitals, prisons, and more. A Narrative Companion Torrey’s tome begins- and so, in turn, this section- with the story of Rosemary Kennedy. Using Rosemary Kennedy’s tragic arc as precedent for the legislative maneuvering that follows her is not sophistry or a useful literary device but is testament to her malaise as a driving cause of the political decisions made in the immediate thereafter. Rosemary Kennedy, sister of President John Kennedy and member of the storied Kennedy political family, was born in 1918. A strain of influenza had been circulating prior to Rosemary’s birth that had been demonstrably linked to the later onset of schizophrenia and other mental disorders.10 It was clear soon after Rosemary was born and began to develop that she had moderate mental retardation; her behavior grew increasingly immature and inappropriate as she physically matured. In late adolescence, Rosemary developed comorbid mental illnesses that further weakened her level of functioning. After years of shielding Rosemary out of the public eye with progressively intricate facades, the Kennedy family decided to lobotomize her in 1941. The surgery resulted in Rosemary losing the moderate level of functioning she once possessed 9 Ibid. 89. Crosby, America’s Forgotten Pandemic, 20; N.Takei et.al., “Prenatal Exposure to Influenza Epidemics and Risk of Mental Retardation.” European Archives of Psychiatry and Clinical Neuroscience 245, no. 4-5 (1995): 255-259; W. Erickson, J. M. Sundet, and K. Tambs, “Register Data Suggests Lower Intelligence in Men Born in the Year after Flu Pandemic,” Annals of Neurology 66, no.3 (2009) S.A. Mednick et al., “Adult Schizophrenia following Prenatal Exposure to an Influenza Epidemic,” Archives of General Psychiatry 45, no. 2 (1988): 189-192. (Citation qtd. Torrey, American Psychosis) 10 and living out the remainder of her life with the mental capacity of an infant. She lived in an institution in rural Wisconsin until her death in 2005. 11 Around the same time as the Kennedy family’s unfortunate brush with the burgeoning psychosurgery industry in the United States, there were a small but growing number of ideologues who believed the deficiencies found in the mid-20th century asylums were not a matter of poor administration but at the very core of the model itself. These thinkers fashioned themselves as visionaries and imagined psychiatry not primarily as a science focused on treating the severely mentally ill but as a profession properly dedicated to promoting the ethereal concept of “mental health” via social engineering and political guidance. Consider the radical vision of Leonard Duhl, an early officer at the NIMH: “The city... is in pain. It has symptoms that cry out for relief. There are the symptoms of anger, violence, poverty, and hopelessness. If the city were a patient, it would seek help...The totality of urban life is the only rational focus for concern with mental illness...our problem now embraces all of society and we must examine every aspect of it to determine what is conducive to mental health.” These contemporaries of the 1963 legislative push helped shape the “community mental health” movement to be an avantgarde crusade with a principal vitriol toward the state hospital as such. Such antipathy from prominent progressive psychiatric professionals involved in this movement is perhaps best revealed in the following quote from Mike Gorman, a member of the Communist Party and a major player in the CMHC movement: “My hidden agenda was to break the back of the state mental hospital.” 12 If paralysis was the goal, Gorman and his ilk undoubtedly played their part in achieving it. Leamer, The Kennedy Women, 433, 712, 795; G. Zielinski, “A Life Outside the Spotlight: Rosemary Kennedy Lived Quietly for Decades as Her Family Made History,” Milwaukee Journal Sentinel OnLine, January 9, 2005, http://nl.newsbank.com/sites/mwsb/; Nasaw, The Patriarch, 628 (Citation qtd. Torrey, American Psychosis) 12 See “Notes” American Psychosis. Chapter 2 Notes, Citations No. 25, 28. 11 The confluence of what Torrey characterizes as the guilt of the Kennedy family over the fate of their daughter, the high-minded idealism of President John Kennedy himself, and the nascent “mental health” ideologues in the early twentieth century were, in tandem, one of the biggest blows to the state mental hospital. The largest normative question inevitably begged by this section- whether the problems displayed by state hospitals in the twentieth century were a product of a primitive understanding of psychotic disorders or a paradigmatic flaw in congregate methods of care more broadly- will be discussed with greater clarity in the piece’s conclusion. Public Finance and the IMD Exclusion “One of the great mistakes is to judge policies and programs by their intentions rather than their results.” -Milton Friedman ❖ Individuals who study deinstitutionalization often frame the ideological underpinnings of the movement as a curious bipartisan agreement on means but not ends: state conservative legislators believed it was fiscally prudent to reduce the role of the state hospitals, while their progressive counterparts believed that the model per se was a species of oppression. This characterization is right, as far as it goes. State Republican legislators were often all too happy to shift costs to the federal level, and civil libertarians and aggrieved activists fought to make involuntary commitment to a state hospital fundamentally impossible save for the most extreme circumstances. But this outline fails to adequately articulate how devastating federal policy was to the state hospital. When President Johnson enacted Medicaid as part of his Great Society initiative, he continued the ideological inheritance of his fallen predecessor when he created the Institutions for Mental Diseases (IMD) exclusion. The IMD exclusion prohibits federal Medicaid monies from being allocated toward any “hospital, nursing facility, or other institution of more than 16 beds, that is primarily engaged in providing diagnosis, treatment, or care of persons with mental diseases, including medical attention, nursing care, and related services.” The Legal Action Center claims this was “intended to ensure that states, rather than the federal government, would have principal responsibility for funding inpatient psychiatric services,” though that characterization fails to mention the simultaneous absurdity of presuming Lyndon Johnson was motivated by subsidiarity and fiscal federalism when his entire political record suggests otherwise, and the shared ideological loyalties that he had with his immediately predeceased Commander in Chief.13 Torrey notes how the IMD exclusion lead states to aggressively release patients from state hospitals who were not capable of handling community life by anecdotally highlighting Illinois: “Illinois not only [encouraged] the placement of severely mentally ill individuals in nursing homes but also abetted the process by intentionally misdiagnosing patients so that they would be eligible for federal Medicaid.” 14 As a 1998 Chicago Tribune report discovered, “the state has modified at least 1,000 psychiatric patient files at 20 other nursing homes, collecting an extra $30 million from Medicaid since 1995.” The Inexplicability of State Policy Fig. 1: Number of Psychiatric Inpatients Over Time PBS. Material from Chapters 1, 3 and the Appendix of: Out of the Shadows: Confronting America's Mental Illness Crisis by E. Fuller Torrey, M.D. (New York: John Wiley & Sons, 1997). 13 "The Medicaid IMD Exclusion: An Overview and Opportunities for Reform." Legal Action Center. Accessed May 11, 2018. https://lac.org/wp-content/uploads/2014/07/IMD_exclusion_fact_sheet.pdf. 14 Torrey, E. Fuller. American Psychosis: How the Federal Government Destroyed the Mental Illness Treatment System. 106. Oxford University Press, 2014. First, I aggregated data from the Treatment Advocacy Center to examine state by state figures on the incidence of severe mental illness and the state’s number of public psychiatric beds. The results are highlighted in Figure 2: Fig. 2 Metrics from www.treatmentadvo cacycenter.org/brow se-by-state Remarkably, there is a weak negative correlation (-0.07) between the incidence of severe mental illness in a state and the number of public psychiatric hospital beds available. This isn’t altogether unsurprising, despite being rhetorically inexplicable- first, a simple correlation coefficient without supporting multivariate analysis is highly subject to noise, potentially muting a hidden relationship between the two. More broadly, however, I think it’s possible that decisions about deinstitutionalization were made with little regard for the (likely Bayesian) distribution of the severely mentally ill nationwide. I additionally utilized data from The American Journal of Political Science to compare their “ideology score” (a score that quantifies a state electorate as conservative or liberal on a gradated scale based on various metrics; 100 is most liberal) and compared that to the availability of public psychiatric hospital beds (Fig. 3).15 I was initially predisposed to think that, perhaps counterintuitively, conservative states would be slightly more friendly to state hospitals if only because progressive states pursued deinstitutionalization on humanitarian grounds quite early and aggressively. The resultant coefficient of roughly -.051 signals quite little other than random noise, though it’s possible that the aforementioned theory played a minor role in the loose relationship established. Citations Torrey, E. Fuller. American Psychosis: How the Federal Government Destroyed the Mental Illness Treatment System. Oxford University Press, 2014. Fig. 3 15 William D. Berry, Evan J. Ringquist, Richard C. Fording, Russell L. Hanson. 1998. Measuring Citizen and Government Ideology in the American States, 1960-93. American Journal of Political Science, Vol. 42, No. 1 (Jan.), pp. 327-348. The prevailing lesson from these futile attempts to ground these policies in rhyme or reason is just that; these policies have been pursued largely in the absence of grand coordination, with mostly rhetorical visions driving otherwise incoherent policy gestures. Conclusion “The freedom to be insane is a cruel hoax perpetrated on those who cannot think clearly by those who will not think clearly.” -Dr. E. Fuller Torrey, M.D. ❖ Acknowledging the Spurious Assumptions of Deinstitutionalization In his review of Dr. Torrey’s book in The New York Times, psychiatrist Dr. Richard A. Freidman notes that the idealists of the mid-twentieth century “were certain that severely mentally ill patients in state hospitals — many living there for decades — would magically adjust to the community and do well with outpatient treatment. How wrong they proved to be.” The seriously mentally ill can indeed function and flourish in society with the right supports. But a sizable minority of that population may need acute or long-term inpatient services, and to deny that certainty is to disconnect oneself from reality the way it is in favor of the way we wish it were. Federal mental health monies are being drowned in rhetorical campaigns to fight “stigma,” and the funding of various advocacy measures to convince the American public to disassociate untreated severe mental illness with violence is little more than a putrid reeducation campaign. Those with severe schizoaffective mental illness who go untreated are more violent than those without, and the facts bear it out plainly. From University of Virginia law professor John Monahan: “The data that have recently become available, fairly read, suggest the one conclusion I did not want to reach: Whether the measure is the prevalence of violence among the disordered or the prevalence of disorder among the violent, whether the sample is people who are randomly selected for treatment as inmates or patients in institutions or people randomly chosen from the open community, and no matter how many social or demographic factors are statistically taken into account, there appears to be a relationship between mental disorder and violent behavior.”16 As more deinstitutionalized persons languish on our streets suffering homelessness or facing incarceration, or the incidence of concerning acts of violence from a minority of those with untreated schizoaffective disorders rises, society as well as individuals have been hurt by the federal abrogation of the states’ role in mental illness treatment. I will finish with a quote from psychiatrist Dinesh Bhugra: “We must never forget that there are always people who will need asylum.” 17 Shouldn’t we as a society provide it? The State Hospital Today Oregon State Hospital Wikipedia Bryce Hospital Wikipedia 16 17 See “Notes” American Psychosis. Chapter 6 Notes, Citation No. 39. See “Notes” American Psychosis. Chapter 8 Notes, Citation No. 13. South Carolina State Hospital Wikipedia Bibliography Torrey, E. Fuller. American Psychosis: How the Federal Government Destroyed the Mental Illness Treatment System. Oxford University Press, 2014. History.com Staff. "Dorothea Lynde Dix." History.com. 2009. Accessed May 09, 2018. https://www.history.com/topics/womens-history/dorothea-lynde-dix. Reidbord, Steven, M.D. "Are Psychiatric Disorders Brain Diseases?" Psychology Today. December 12, 2015. Accessed May 9, 2018. https://www.psychologytoday.com/us/blog/sacramento-street-psychiatry/201512/arepsychiatric-disorders-brain-diseases. T.R. Insel, “Assessing the Economic Costs of Serious Mental Illness,” American Journal of Psychiatry 165, no 6 (2008): 663-665; D.E. Marcotte and S. Markowitz, “A Cure for Crime? Psycho-pharmaceuticals and Crime Trends,” Working Paper 15354 (Cambridge, MA: National Bureau of Economic Research, 2009), http://www.nber.org/papers/w15354 (Citation qtd. Torrey, American Psychosis) Vaughn Tesei, Jill. "Meeting with Jill Vaughan Tesei APRN." Interview by John S. Hirschauer, Jr. Crosby, America’s Forgotten Pandemic, 20; N.Takei et.al., “Prenatal Exposure to Influenza Epidemics and Risk of Mental Retardation.” European Archives of Psychiatry and Clinical Neuroscience 245, no. 4-5 (1995): 255-259; W. Erickson, J. M. Sundet, and K. Tambs, “Register Data Suggests Lower Intelligence in Men Born in the Year after Flu Pandemic,” Annals of Neurology 66, no.3 (2009) S.A. Mednick et al., “Adult Schizophrenia following Prenatal Exposure to an Influenza Epidemic,” Archives of General Psychiatry 45, no. 2 (1988): 189-192. (Citation qtd. Torrey, American Psychosis) Leamer, The Kennedy Women, 433, 712, 795; G. Zielinski, “A Life Outside the Spotlight: Rosemary Kennedy Lived Quietly for Decades as Her Family Made History,” Milwaukee Journal Sentinel OnLine, January 9, 2005, http://nl.newsbank.com/sites/mwsb/; Nasaw, The Patriarch, 628 (Citation qtd. Torrey, American Psychosis) “Notes” American Psychosis. Chapter 2 Notes, Citations No. 25, 28. "The Medicaid IMD Exclusion: An Overview and Opportunities for Reform." Legal Action Center. Accessed May 11, 2018. https://lac.org/wp-content/uploads/2014/07/IMD_exclusion_fact_sheet.pdf. William D. Berry, Evan J. Ringquist, Richard C. Fording, Russell L. Hanson. 1998. Measuring Citizen and Government Ideology in the American States, 1960-93. American Journal of Political Science, Vol. 42, No. 1 (Jan.), pp. 327-348. PBS. Material from Chapters 1, 3 and the Appendix of: Out of the Shadows: Confronting America's Mental Illness Crisis by E. Fuller Torrey, M.D. (New York: John Wiley & Sons, 1997). “Notes” American Psychosis. Chapter 6 Notes, Citation No. 39. “Notes” American Psychosis. Chapter 8 Notes, Citation No. 13. Treatment Advocacy Center